

Covid 3/18: An Expected Quantity of Blood Clots

This week’s Covid news was that most of Europe suspended administration of the AstraZeneca vaccine over reports of blood clots. This was ludicrously stupid several times over. There was always going to be something that happened to correlate with vaccination days to some extent, somewhere, over some time period. The number of blood clots experienced after vaccination wasn’t even higher than the base rate you would otherwise expect. And even if all the observed clots were extra, all were caused by the vaccine, all were fatal, and that represented the overall base rate, and we ignore all population-level benefits and economic issues, the vaccine would still be worth using purely for personal health and safety by multiple orders of magnitude.
The WHO and EMA said there was no evidence there was an issue.
None of that mattered, as one by one countries suspended injections as part of a blame avoidance strategy. As a result vaccinations are hold, thousands (or more) will die as a direct result, with many European countries seeing things getting worse rather than better and facing possible new restrictions, and with a permanent new weapon in the arsenal of vaccine skeptics that we’ll have to hear about for decades, long after this is proven to be a non-concern.
Meanwhile, in the United States, deaths are happily way down, but case numbers have stopped dropping due to the rise of the new strains, and will likely start ticking upwards once again for a while. Whether or not this will count as a last surge/wave is unclear, it looks like the strains aren’t as additionally infectious as we feared and vaccinations are going well, so it might not be so bad.
Also, we (myself and the anonymous donor) awarded the Covid Microgrants, for details see the section on that below.
Let’s run the numbers.
The Numbers
Predictions
Prediction (WaPo numbers): Positivity rate will be 4.2% (unchanged) and deaths will fall by 12%.
Results from WaPo Covid page, which I picked last week as the data source:

Positivity rate was indeed close to unchanged, but I see a contradiction with the Wikipedia data. The Washington Post source says there were 26% fewer tests and an essentially unchanged positive rate. Wikipedia reports essentially a flat number of positive tests. Those two things can’t both be true at the same time, so someone has this wrong. John Hopkins has 4.7% positive rate right now, but their data a week ago was jumping around due to an anomaly so it’s hard to get a good week over week number out of them here.
I think this comes down to the data anomaly a week ago, which different places are handling differently? Which previously was easy to handle since I had a good chart, now I have a bunch of graphs and have to dig for actual raw numbers when I want them. Oh how I miss the Covid Tracking Project.
My guess and hope is that such disagreements between sources will usually be much smaller than this, and my best guess on what happened is that the real positivity rate didn’t change much. I’m going to treat tha 26% decline in reported tests at WaPo as not real, and assume that’s where the mistake is.
On deaths, we did much better than I expected. A 12% decline is good, a 28% decline is fantastic.
Prediction (WaPo numbers): Positivity rate of 4.3% (up 0.2%), deaths decline by 8%.
I don’t think we can sustain this huge decline in deaths because the decline in cases mostly stopped about a month ago, but given how slow deaths were to decline there’s clearly a bunch of extended and variable delays in death reporting, even more so than previously appreciated, so some additional decline seems likely. Also, whenever there’s a huge jump there’s a decent chance some of it is shifting things in time, and there will be a bit of reversion.
Positivity rate likely starts creeping back upwards in the short term.
Deaths
DateWESTMIDWESTSOUTHNORTHEASTTOTALJan 28-Feb 3552430788071341020083Feb 4-Feb 10493726877165342918218Feb 11-Feb 17383722215239270013997Feb 18-Feb 24365224334782242713294Feb 25-Mar 3383416695610195813071Mar 4-Mar 1025951775371415399623Mar 11-Mar 1714921010321714027121

This is excellent news as deaths continue to decline steadily. We’re finally seeing the full impact of the decline in cases, especially in the Midwest and West. This was essentially the best case scenario, as substantially bigger declines would have mostly caused me to suspect data issues.
The bad news is that these declines are probably going to stall out soon, since cases aren’t declining at these rates anymore.
Positive Tests
DateWESTMIDWESTSOUTHNORTHEASTFeb 4-Feb 10144,90299,451255,256149,063Feb 11-Feb 1797,89473,713185,765125,773Feb 18-Feb 2480,62564,857150,493110,339Feb 25-Mar 366,15158,295151,253115,426Mar 4-Mar 1062,93557,262114,830109,916Mar 11-Mar 1749,69659,881109,141115,893

All hail the control system, which has successfully once again reasserted itself. We will face increasing pressure from further reopenings and increased dominance of the new strains, and will get steady additional help from vaccinations and warmer weather. Soon we will see which side of that is stronger. In the long run, of course, the vaccinations will win out unless new strains manage to escape them and we don’t respond in time, but in the short run things are more likely to get somewhat worse first before they get better.
Vaccinations

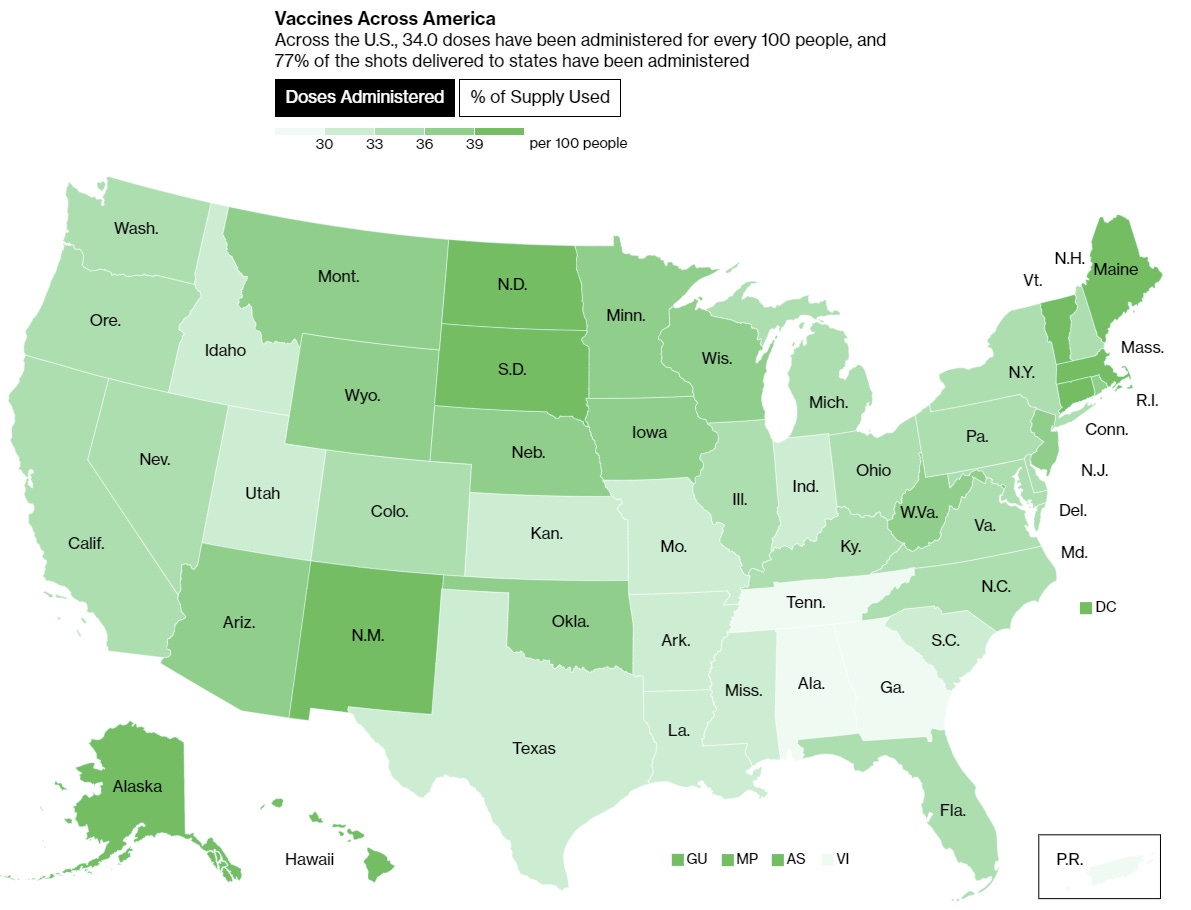
Things are going well on the vaccination front in America. Regional differences exist but steady progress is being made everywhere, and additional supply steadily comes online. We may be a little bit ahead of ourselves with the weekly number due to the giant spike earlier in the week, but much of that was given back the next day, and the steady improvement in volume seems quite real.
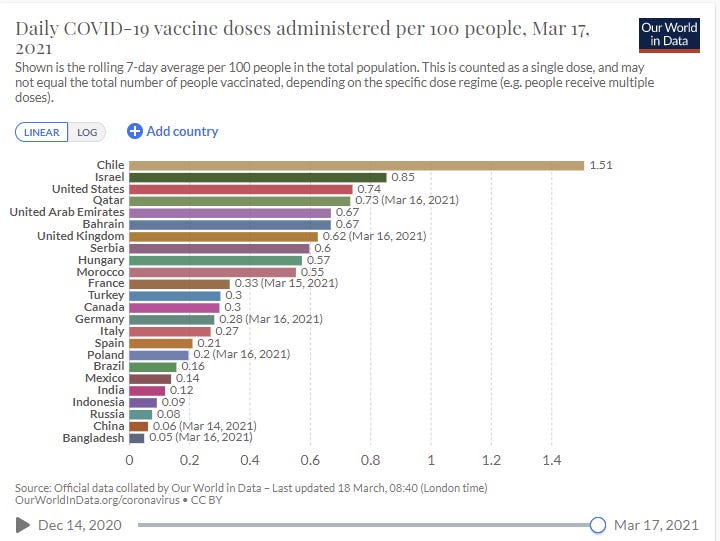
The news in Europe is not as good, because not only were they already far behind, now they’re suspending AstraZeneca shots for no reason, which is the big news item this week.
(I’m going to stop showing the Europe graphs each week as I don’t think they’ve been worthwhile recently, but if you want to find that info yourself you can always get it at OurWorldInData.)
Europe Panics Over Actual Nothing, Halts AstraZeneca Vaccinations
The AstraZeneca vaccine does not cause blood clots.
At all. No, seriously. It simply doesn’t cause blood clots. Wenodis. We are aware of this.
The whole incident is so mind-bogglingly insane and stupid that I don’t even know where to begin.
From what I can tell, the sequence of events was something like this.
A lot of people got the AstraZeneca vaccine.
Because we are paranoid about possible side effects, there’s extensive reporting of anything that happens to people right after getting the vaccine.
Because of #1 and #2, we record a lot of stuff that happens by coincidence, because this isn’t Unsong.
At some point, in some region, over some time period, something bad will happen more often than chance within that region and period, because that’s how probability works.
In this case #4 is certain types of blood clots in some places at some times.
Many did not notice or care that the overall rate of blood clots for those getting vaccinated is actually below the population base rate, and similar to the rate for those getting the Pfizer vaccine.
Many did not notice or care that even if all the blood clots were due to the vaccine, and then in addition even if all the blood clots were fatal, neither of which is possibly true, the vaccine would still be worth taking by multiple orders of magnitude.
Even the WHO and EMA said there was no evidence and nothing to worry about.
Everyone in Europe lost their minds and collectively massively sabotaged the vaccine effort, and likely all vaccine efforts everywhere permanently, by halting vaccinations ‘as a precaution.’
People will die.
People will also get more blood clots, because Covid-19 does cause them.
People everywhere will have new stupid arguments that will make people not get vaccinated, likely for all vaccines, permanently, which is already happening.
All of this due, effectively, to pure p-hacking, without even bothering to pretend otherwise.
In addition to being below the base rate, the incidents with AstraZeneca weren’t substantially different from the incidents with Pfizer, because again they are random.
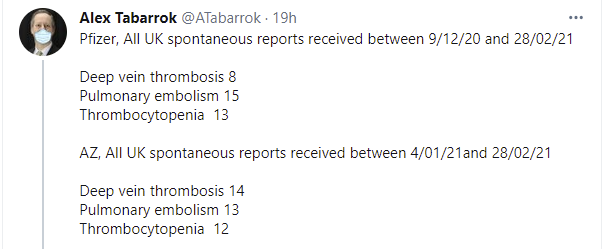
Or as my friend put it when in an unfairly charitable mood:


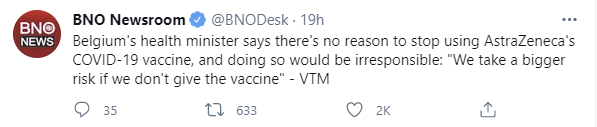
Or, in the words of one of the few remaining possibly sane European health authority figures:
Again, let’s be crazy generous and say all 39 cases both were entirely caused by the vaccine (which they weren’t, since again below base rate) and also killed all the patients (which they didn’t, death rate from blood clots is 10-30% per Google). That’s 39 deaths in 9.7 million doses, for a fatality rate of one in 300,000. For example, if that happened to the entire United States it would kill about a thousand people, so purely in terms of deaths it would be about the price of delaying vaccinations by one day.
Also, by the way, there’s this:

So it’s not remotely fair to use the background population rate when you’re explicitly targeting your elderly population for vaccinations. This is so much more insane than it looks at first glance.
It’s purely and simply this (link to Reuters):

Another simple Fermi calculation:
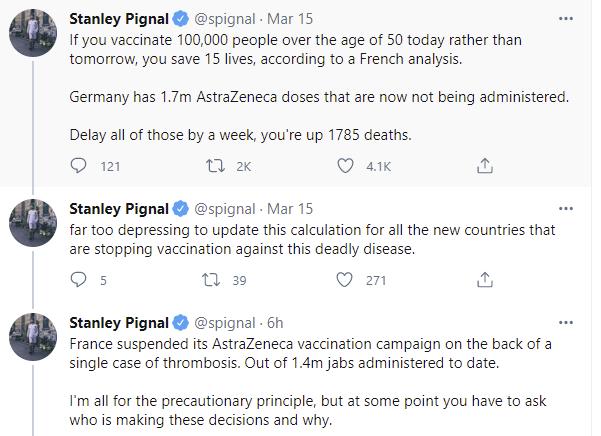
And again, how many people could this possibly kill, even if several things went impossibly badly, in exchange for saving those 1,785 lives?
Six.
Not six thousand. Not six hundred. Six.
What do you idiots slash mustache-twirling villains have to say for yourselves, and do you have a preference as to which of those two ways would you prefer to be primarily identified?

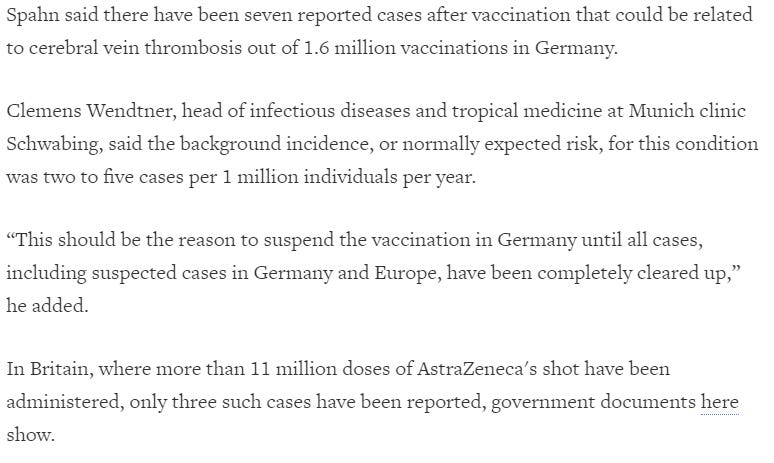
Link to the Q&A here (in German). Translated, here’s the meat of it:

So of all the potential things that can go wrong you managed to find one subsection of one thing that happened more often than chance, and let’s be super generous and again assume that all seven were lethal and also that all seven were caused by vaccination and that’s the typical rate going forward, and (does math) yeah you’re still off by more than two orders of magnitude and you know it, but you have a legal obligation to these people that forces your hand, because ‘there could be legal consequences’? And there’s no way to, say, pass a new law to fix that, even if you should have fixed it long ago? So that’s it, nothing you could do, huh?
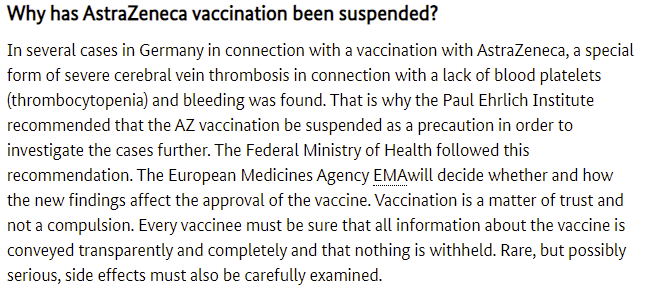
Also there was this:

Read that last line again and think about what it implies in the context of this question.
The amount of damage this is already doing to vaccination effort is staggering. I got this comment on my last post:
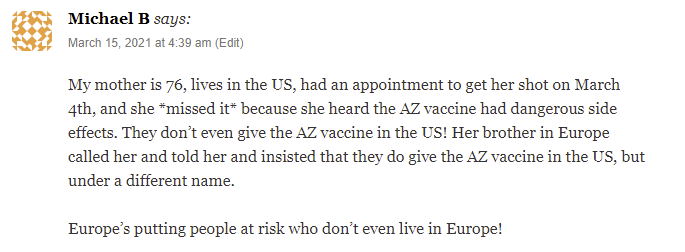
On her first day back after our trip, my wife saw five patients. Two of them expressed serious concern about getting vaccinated in the United States, where they don’t even give the AstraZeneca vaccine, due to these concerns, and she had to spend a bunch of time explaining the several-layered absurdity of that concern. A twitter poll I did already found multiple people saying they know of a shot that was missed. This is only going to get worse.
On my todo list is to do a standalone pure ‘why vaccinations are safe and effective and everyone should get one as soon as possible if they’re able to do so’ post, if no one else has one that does the job well enough. Is there a good one already in existence? Several people have asked, and there’s nothing I’m fully happy pointing people towards. The concern is not ‘you should take one now even if you’re worried others need it more’ but rather ‘if and when there’s enough shots for everyone you really really need to take one,’ which is the error that matters far more overall.
Better To Have Vaccinated And Stopped Than Never To Have Vaccinated At All
Europe halted AstraZeneca vaccinations. And that’s terrible.
Then again, at least they started doing AstraZeneca vaccinations, without which halting them would have been impossible. America didn’t even start them, and have been holding hostage tens of millions of doses? Isn’t at least starting a pretty good relative result? Isn’t it a mistake to bring down the shame hardest on the person who at least interacted with the problem and did some good, even if they nonsensically stopped, rather than the one who did no good whatsoever?
In this case, I don’t think that applies, because halting distribution is causing large active harm over and above the lack of doses being administered, and because halting it now after approving it is far more indefensible than failing to approve in the first place. Failing to approve also isn’t defensible, but if you’re committed to defending power and ‘ethics’ and counterproductive principles above all else then at least it makes some sense. It can be argued it’s at least consistent and it doesn’t quite fully mean You Fail Statistics Forever. Halting now is some combination of malice and pure madness. It is choosing to cover one’s ass against blame for the perception of irresponsibility at the cost of thousands of lives. Perhaps the blame dynamics involve this, which would be an impressive shooting of one’s nose to spite one’s face...
...or it’s (also) something worse.
There isn’t a better option.
That doesn’t let the United States off the hook. But I am very happy that we are not right now halting one of the vaccines for no reason, because that would do that much more damage. And I do think the suspensions are a much worse sign of dysfunction than America’s failure to begin in the first place. To get this result, the rot must go far deeper.
The most harmful act of all around AstraZeneca, of course, is the United States deciding to hold onto tens of millions of doses indefinitely, left to sit in warehouses unused, while it refuses to approve it and also refuses to send it out, although it is now considering sending some to Mexico and Canada, both of whom have asked for doses. Then again, that’s exactly as harmful as never making those doses in the first place, so it’s hard to know what’s effectively being punished if we accept that politics and power won’t let us export the doses. Economists talk about ‘tax incidence’ and who effectively ends up with the bill for a tax (e.g. the ‘employer half’ and ‘worker half’ of social security are not economically distinct and making one side pay all of it would change very little) and this makes me think about blame incidence, especially now that I (may? have begun to?) understand how central blame is in decision making.
The English Strain
From the Washington Post, in a standard issue ‘look at the irresponsible ones’ article :
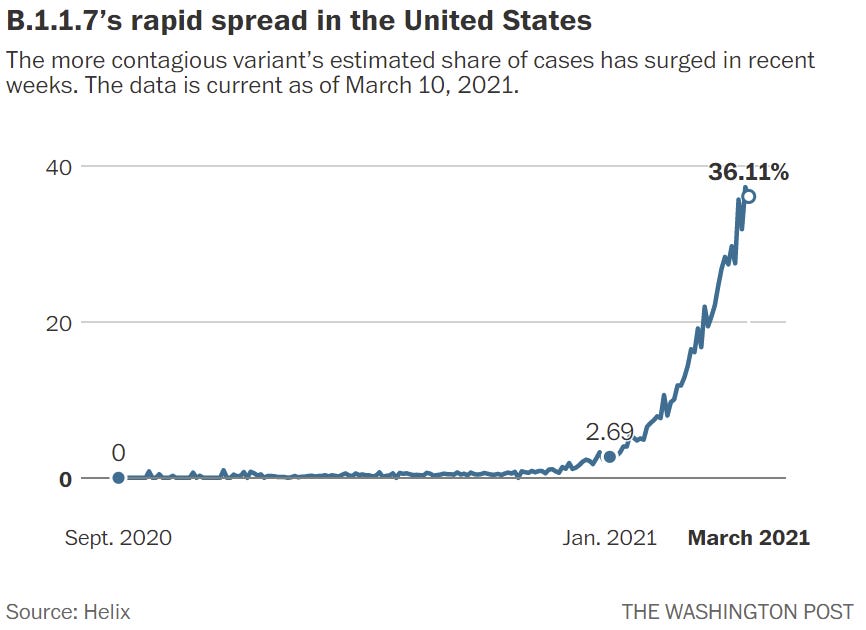
How does that stack up against what the naive model said? If we have 2.7% in January, and assume it means something similar to what ‘March’ means here, we can compare that to a predicted 2.88% for the week of January 18. Then we compare the 36% endpoint to our naive prediction of about 72%, and notice that things are substantially behind schedule since then. That’s great news. Curve fitting gives a rise in R0 from the new strain of only 35%. If that’s accurate, then the model predicts that the new strain prolongs our pain, but there is never a last surge.
What that model isn’t doing is drawing any distinctions between regions. It presumes that spread is evenly distributed around the country, which is obviously false. That could plausibly mean that we’re underestimating the danger substantially and will see surges in the harder hit places.
Prediction for the control system is hard to evaluate, and will be key to how this plays out. Clearly levels of precaution are declining, but putting a figure on how much they are declining is very difficult. Could be a small impact, could be a large one.
The alternate explanation is that my five-day cycle is too short, which would be bad news, but would still mean we have more time than we expected and it’s probably not so bad.
Six Feet Good, Three Feet Acceptable In Pinch
The CDC suggests child prison social distancing requirements could soon change, and be reduced from six feet to three feet. You see, there was one recent study that said with full and proper masking that three feet distancing was “safe.”
This is what happens when various political requirements and elite demands are dominant over decision making, with the scientific justifications being designed to fit whatever the elites need, combined with the obsession with telling people strict/absolute simple rules rather than anyone involved treating the world as a physical object.
What happened here seems simple. The CDC said 6 feet distancing because they’ve been saying 6 feet distancing for a year, and if you suddenly said 3 feet in a school then everyone would quite rightfully ask what the hell the whole 6 feet thing had been about this whole time, whereas the 6 feet rule is the one thing that everyone has mostly agreed to agree upon even if in practice it often gets ignored.
So the CDC basically came out with guidance that said for child prisons to do their best to follow existing CDC rules for adults, even for children as young as 2, and then do their best to reopen.
(You should know this already: The actual physical effect, of course, is gradual rather than a step function, likely similar to an inverse square law, so 3 feet I am guessing is about four times riskier than 6 feet, if everyone is exactly 3 or 6 feet apart respectively, and the goal of a 6 foot restriction is to get people to at least be a few feet apart and not crowd into spaces too aggressively.
There’s also what they see as a necessary distinction between ‘safe’ actions, which allow the retention of a state of grace, and ‘unsafe’ actions, which are blameworthy, and to label everything as either one or the other, with the ability of guidelines to change which is which when the guidelines change, because they don’t think people can handle anything else.)
Then a lot of child prisons, and especially teachers and teachers’ unions, interpreted the guidelines as actual requirements rather than goals or suggestions, and it was clear a lot of child prisons would remain largely or entirely closed, with prisoners forced to go remote.
People in power didn’t like that, they wanted the child prisons open, and things will soon be in a place where if the 6 foot rule became 3 feet in general in many places it wouldn’t be that big a disaster, so now the rules are changing, with the one Massachusetts study being used as a fig leaf, despite no one being fooled that we suddenly had learned something from it, let alone that it was strong evidence.
As always when thinking about child prisons, it’s hard for me to get behind putting our children in child prisons, but given that the alternative is virtual child prisons that are very clearly even worse, and the economic aspects of all this, I’m fine with treating the desire to reopen the child prisons as legitimate. Given that need, and the real physical risks involved, the previous guidelines were wrong and the potential new guidelines are better.
So this change would be good, even if the process that got us here wasn’t great, and even if issuing the first set of guidelines will continue to cause a bunch of issues. With children (who are effectively largely immune) and vaccinated teachers (almost entirely immune) and masks everywhere, of course you can loosen the distancing requirement.
The even more interesting question here is, if these guidelines do get issued, how do people react more broadly? Do they think ‘oh the six foot thing was all a lie?’ Do all elites memory hole that we ever said six feet and start saying three feet, and how much whiplash does that cause? If the one central rule goes out the window does everyone start treating all of it as one big joke? It would be quite an interesting experiment that should increase popcorn sales.
Alternatively, perhaps that’s a lot of the pseudo-intent here? Use the schools as a backdoor way to loosen distancing requirements without having to out loud admit they were arbitrary, by counting on The People to notice the contradiction, once we get to a place where we want some continued caution but not to go nuts, as we are likely to be in August?
We Must Protect This House
The House of Representatives has a problem. They would like to return to normal operations, but 25% of their members are being idiots and refusing to get vaccinated (or getting vaccinated but then neglecting to inform others of this, presumably for political reasons). With so many unvaccinated members, the Office of the Attending Physician is unwilling to relax social distancing guidelines.
The problem isn’t lack of supply. That would be even more insane, and congress has its own supply. As much as crippling the speed at which the house can do business appeals to me, our representatives should have and do have full vaccine access at this point.
At least there’s this, which is some small comfort:

But they still have to put up with things like this:

If I were in charge of the house, I’d tell everyone to get vaccinated because starting in a few weeks I was going to expel anyone who wasn’t, or at least bar the doors and not let them in until they fix it, whether or not there’s a way to let them do remote voting anyway, unless they somehow have a physician’s note saying why they can’t get it. There are plenty of workplaces doing the same. Dare the other side to defend not getting vaccinated and make a big deal out of it.
What I’m curious about is to what extent the refusals are about ‘worried that their crazy base will see it as a betrayal to get the vaccine,’ to what extent it is actual failure to understand that the vaccines are safe and effective and worthwhile, to what extent it is their hatred of the other members of the House and a desire to make their lives as difficult as possible, and to what extent it is a strategic move to delay the work of the legislature.
I like to think the last one is primary, a lot of them secretly did get vaccinated but are refusing to say so in order to prolong the delays as long as possible, and that these Representatives are mostly like the one who had a cloth mask on that said “I’m just wearing this so I don’t get fined” while having an N95 on underneath. The alternatives involve sufficient disconnection from reality that they are even more concerning.
One response to this is that a 75% uptake rate is better than what the public is reporting, and that’s without the ones who got vaccinated, so the number is not so bad especially given some of the 25% presumably did get vaccinated, and we don’t need an explanation.
Covid Microgrants Have Been Awarded
I was very happy with the results here. We got many good responses, and I am proud to announce that we are giving out $39,000 in grants to ten applicants.
Or at least, we are trying to give out $39,000. It’s proven surprisingly difficult, because several people who thought they had a working PayPal account were often surprised to learn that a four-figure international transfer required much additional paperwork. Hopefully all of that sorts itself out, and as of this edit on Thursday afternoon nine of ten payments have been resolved successfully.
The recipients are:
Someone who wishes to remain anonymous, who is working on the vaccine availability website vaxxmax.com, which interfaces with RiteAid.
Someone else who wishes to remain anonymous, who is working on the vaccine availability website vacfind.org.
Someone else who also wishes to remain anonymous, who is working on https://forecasting-covid.com/, which will recreate covid19-projections.com using a new data source, likely Johns Hopkins.
Konstantin Likhter, who is working on the vaccine availability website covidwa.com for residents of the state of Washington.
Po-Shen Loh, who is working on a better app-based method to do multi-stage contact tracing.
Lisa Hakkert, who is working on pandemic modeling and how the pandemic interacts with internet access.
Jakob Jonnerby, who is working on school reopening plans.
Dylan Alban, who gets special mention for stopping before accepting the money to note that his team had pivoted to working primarily on a different project, the vaccine availability website https://vaccinespotter.com, and making sure we still wanted to support him.
Abraham Hinteregger, who is working on advocacy for First Doses First.
Garrett Schilkey, who is working on 3D modeling of UVC lighting and its preventative effects.
There’s a clear theme here. These are all IT or modeling projects, and the bulk of it are websites that help track availability of vaccine appointments. This was informative on several levels, not least of which it was a pointed reminder of who reads these posts. More than that, it drove home that this is the strongest current source of small low-hanging fruit an individual can easily pick. Offering information on where appointments are available is not illegal or even regulated, and that’s a sharp contrast to other many areas.
The vaccine rollout is a hodgepodge of different stuff, so helping ensure that people can find appointments reasonably, and that vaccine does not sit idle, is a big game that can be accomplished for relatively little investment.
I’m sad we didn’t get to do this earlier, when there was more room to have a bigger impact, but better late than never.
Our plan is to follow up later to see how things went, and report back. There’s some chance this or something similar will be open again some time, but we do not have any concrete plans at this time for doing so.
In Other News
Not Covid-19 directly but central to how this column makes decisions: Politics is way too meta.
Badly needed, but actually, given we just now did it and only this much, it seems it’s incredibly hard...

In case there were still doubts what Cuomo is:

It’s not every day you get to look this clearly into a glass house and watch the residents throw stones, I mean wow just wow:

Novavax vaccine 96% effective in preventing mild and severe illness, still not approved.
Yo-Yo Ma uses post-vaccination observation period as a concert for newly inoculated.
Not centrally covid, but seems like a worthwhile data point that private equity purchases of nursing homes found to have very large harmful effects.
Would you go for it, or just let it slip?

Remember, you miss 100% of the shots you don't book an appointment for. See everyone next week.