

Covid 1/14: To Launch a Thousand Shipments

Pardon me while I make my way to the rooftops.
So I’m sure it’s not that simple especially because of regulatory issues, but... did you hear the one where humanity could have produced enough mRNA vaccine for the entire world by early this year, and could still decide to do it by the end of this year, but decided we would rather save between four and twelve billion dollars?
If not, there’s a section on that.
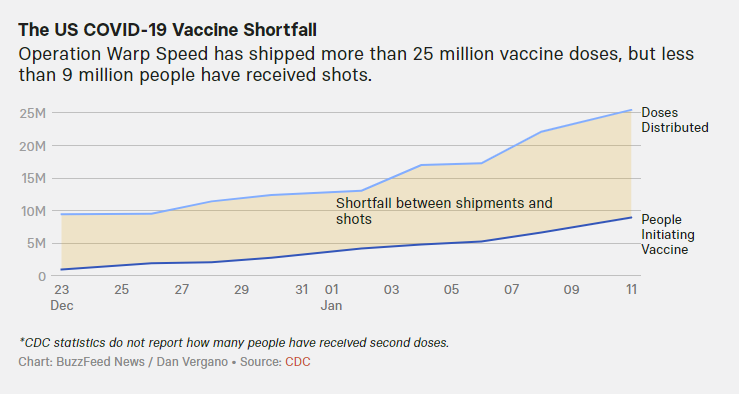
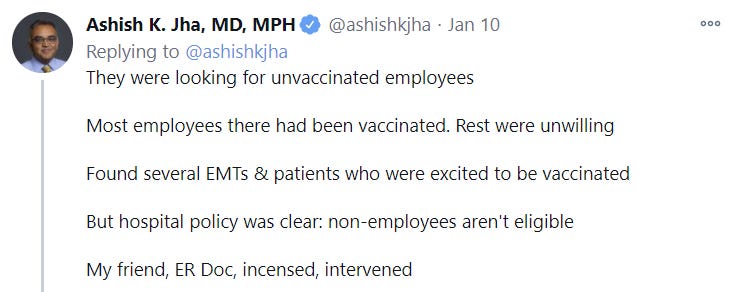
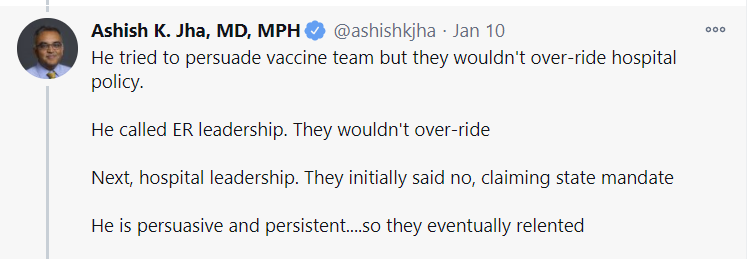
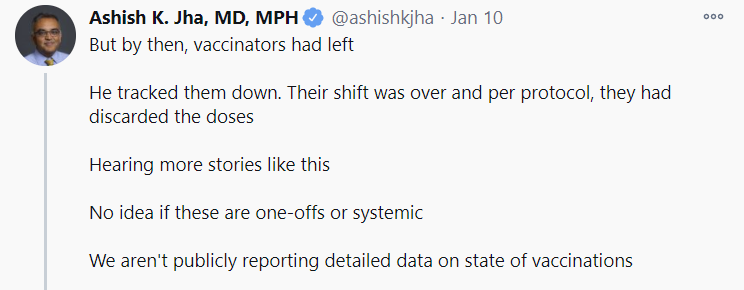
Meanwhile, we also can’t figure out how to put the vaccine doses we already have into people’s arms in any reasonable fashion. New policies are helping with that, and we are seeing signs that things are accelerating, but wow is this a huge disaster.
We took some steps this week towards sane policy. Everyone over 65 is eligible in most places due to new CDC guidance. All doses we have will be distributed rather than reserved. Distribution will be based on the speed at which existing doses are put into arms. Mass vaccination centers are coming online. One can be hopeful for the path of future policy. At a minimum, it’s a start.
In the near term, deaths are way up, the majority of which is almost certainly a real increase, and they probably won’t peak for another week or two. Positive test rates are down a little, but that’s explained by the thankfully rising test counts, so we have not yet meaningfully turned the corner after Christmas.
We likely won’t have that much time to do so before things get worse again. The English strain is definitely coming. It looks like it won’t be as bad as it looked like it might be, so we’ll have some more time and the end result won’t be as severe, and it looks like England has been able to use sufficiently extreme measures to contain it in the last few days, but it’s definitely here, definitely spreading and definitely going to make things a lot worse.
Let’s run the numbers.
The Numbers
Predictions
Prediction last week: 17.0% positive rate on 9.5 million tests, and an average of 2,800 deaths. The holidays are over, there will be some fallout, with things getting slightly worse, but with the main boost in deaths from Christmas mostly coming later.
Results: 15.2% positive rate on 11 million tests, and an average of 3,325 deaths.
This guess turned out to be backwards. We got a lot more rise in the death rate than I guessed. The positive test rate improved as we cleared past the holidays and got more testing online, but reported deaths increased much faster than I expected despite there not being enough time for people to have died from infections over Christmas, a lot of which was presumably our reporting getting back online and catching up.
I treat this as likely a single conceptual error, where I underestimated and misunderstood the warping effects of reporting and measurement from the holiday. We saw a real effect from Thanksgiving, and I expected that again, but this was larger, and I didn’t properly adjust for that. I think that’s where most of the mistake lies, rather than a misunderstanding of the physical situation on the ground in terms of infections or deaths.
The new strain is having a small effect on infections, but not enough to notice on a graph or chart. That will come later.
Prediction: 14.0% positive rate on 11.7 million tests, and an average of 3,650 deaths.
We’re already almost three weeks past Christmas, so I don’t expect the death rate to rise that much more, but I also didn’t expect this much this week. My guess here attempts to split the difference.
Deaths
DateWESTMIDWESTSOUTHNORTHEASTTOTALNov 5-Nov 111089271225358707206Nov 12-Nov 1812552934281811278134Nov 19-Nov 25176141693396171411040Nov 26-Dec 2162838142742193910123Dec 3-Dec 9243755084286274414975Dec 10-Dec 16327853244376354116519Dec 17-Dec 23382651585131377217887Dec 24-Dec 30336336684171364014842Dec 31-Jan 6455341275019416217861Jan 7-Jan 13628039637383475222378

That’s a disaster, far worse than I expected. Christmas lags in reporting can explain some of it, but with rises this big, that is little comfort. Things are very, very bad out there. We do know the Midwest has peaked, but the other regions are definitely not there yet, and this is far above previous peaks.
Two things I track on my spreadsheet but don’t post are the 14-day and 21-day lagged rolling 7-day average CFRs. Those numbers had been dropping steadily over time, rose a bit and peaked on 12/22, then dropped once again. They are now back at their 12/22 peak, presumably because of cases we missed two or three weeks ago due to lack of testing.
There’s at least some worry that the true IFR has also risen more than I realized, due to hospitals being overwhelmed in many areas.
I still think this wave of deaths will peak within a few weeks, and will then start declining until the new English strain shows up in force, as we feel the full Christmas effect in terms of both deaths and reporting, but I’m far from certain, and it’s not likely to be that steep a slope down even before the next crisis starts.
Positive Test Percentages
PercentagesNortheastMidwestSouthWest11/12 to 11/186.99%18.90%11.64%10.66%11/19 to 11/257.00%16.62%10.41%11.75%11/26 to 12/28.38%17.90%12.45%12.79%12/3 to 12/910.47%17.94%13.70%12.76%12/10 to 12/1610.15%15.63%15.91%13.65%12/17 to 12/239.88%14.65%15.78%13.82%12/24 to 12/3010.65%14.54%17.07%12.90%12/31 to 1/612.18%17.03%19.69%15.94%1/7 to 1/1311.70%14.81%18.14%15.12%

Encouraging numbers, but likely mostly due to increased testing.
Positive Tests
DateWESTMIDWESTSOUTHNORTHEASTNov 26-Dec 2256,629357,102294,734185,087Dec 3-Dec 9354,397379,823368,596263,886Dec 10-Dec 16415,220315,304406,353260,863Dec 17-Dec 23439,493271,825419,230236,264Dec 24-Dec 30372,095206,671373,086225,476Dec 31-Jan 6428,407251,443494,090267,350Jan 7-Jan 13474,002262,520531,046306,604

These increases are due to more testing rather than higher test percentages, so no reason to be alarmed, but also no reason to feel especially good about the situation either.
Test Counts
DateUSA testsPositive %NY testsPositive %Cumulative PositivesNov 5-Nov 118,290,41710.8%1,059,5592.4%3.16%Nov 12-Nov 189,040,42612.4%1,155,6702.9%3.50%Nov 19-Nov 2510,419,05911.8%1,373,7512.9%3.88%Nov 26-Dec 29,747,02611.8%1,287,0104.0%4.23%Dec 3-Dec 910,465,25413.9%1,411,1424.9%4.67%Dec 10-Dec 1610,701,13413.9%1,444,7254.9%5.12%Dec 17-Dec 2310,716,18913.7%1,440,7705.1%5.57%Dec 24-Dec 309,082,25713.9%1,303,2866.0%5.95%Dec 31-Jan 69,333,47016.4%1,365,4737.3%6.42%Jan 7-Jan 1311,054,68515.2%1,697,0346.6%6.93%
Testing is back, and we’ve finally broken 11 million tests in one week. Hopefully this represents a return to growing test counts, and we’ll see continued increases. It does mean that the drop to 15.2% positive tests is not as encouraging as it otherwise looks, as the rise in tests mostly explains it. We can’t be confident that things are improving much yet. It does mean we don’t have to be worried about the rise in positive test counts we saw this week.
Covid Machine Learning Projections
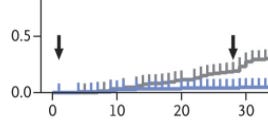
Now with vaccinations! That’s what the extra two lines are on the top graph, with the light blue being first dose and the dark blue being second dose.
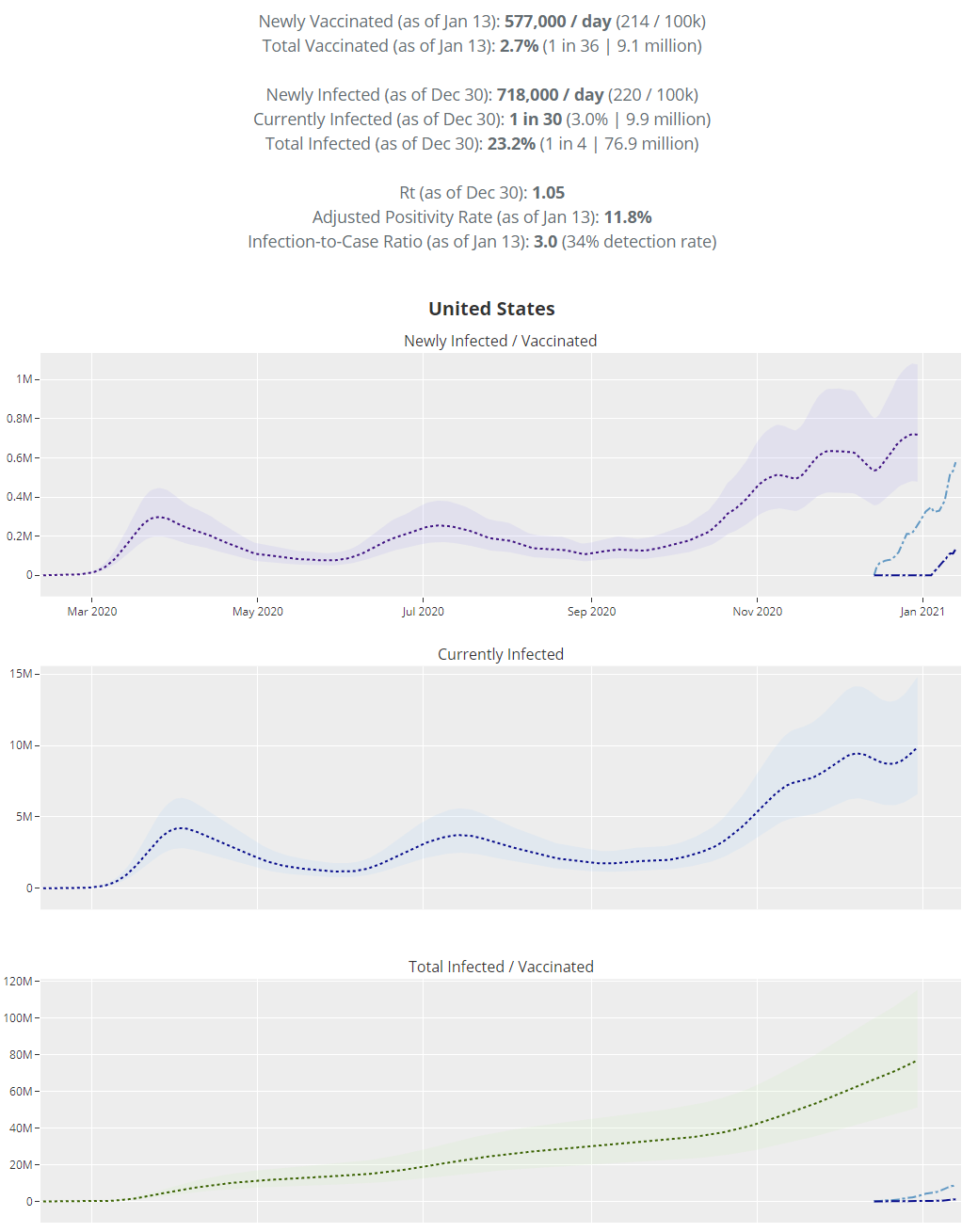
The projections here seem to not think much of Christmas, which is odd. They had total infections as of December 23 at 21.7% last week, which the model still believes, and it thinks as of December 30 the number is now 23.2% infected. As usual, I consider these lower bounds, and that means herd immunity is making rapid progress on two (alas, mostly uncorrelated) fronts.
For vaccinations, the model is smoothing out weekends, which it probably shouldn’t do, as the day-of-the-week cycle of activity is very much real, but it does make the graph easier to read.
The point where vaccinations exceed new infections looks like it will arrive sometime near the end of January. That doesn’t mean we’re ‘winning’ in any real sense, but it is at least something.
Vaccinations
This twitter thread can be useful, because it provides the daily delta in number of doses administered in an easy to view format.
To avoid getting too depressed by the overall look, remember that the colors indicate relative vaccinations, because the color scheme adjusts each week.
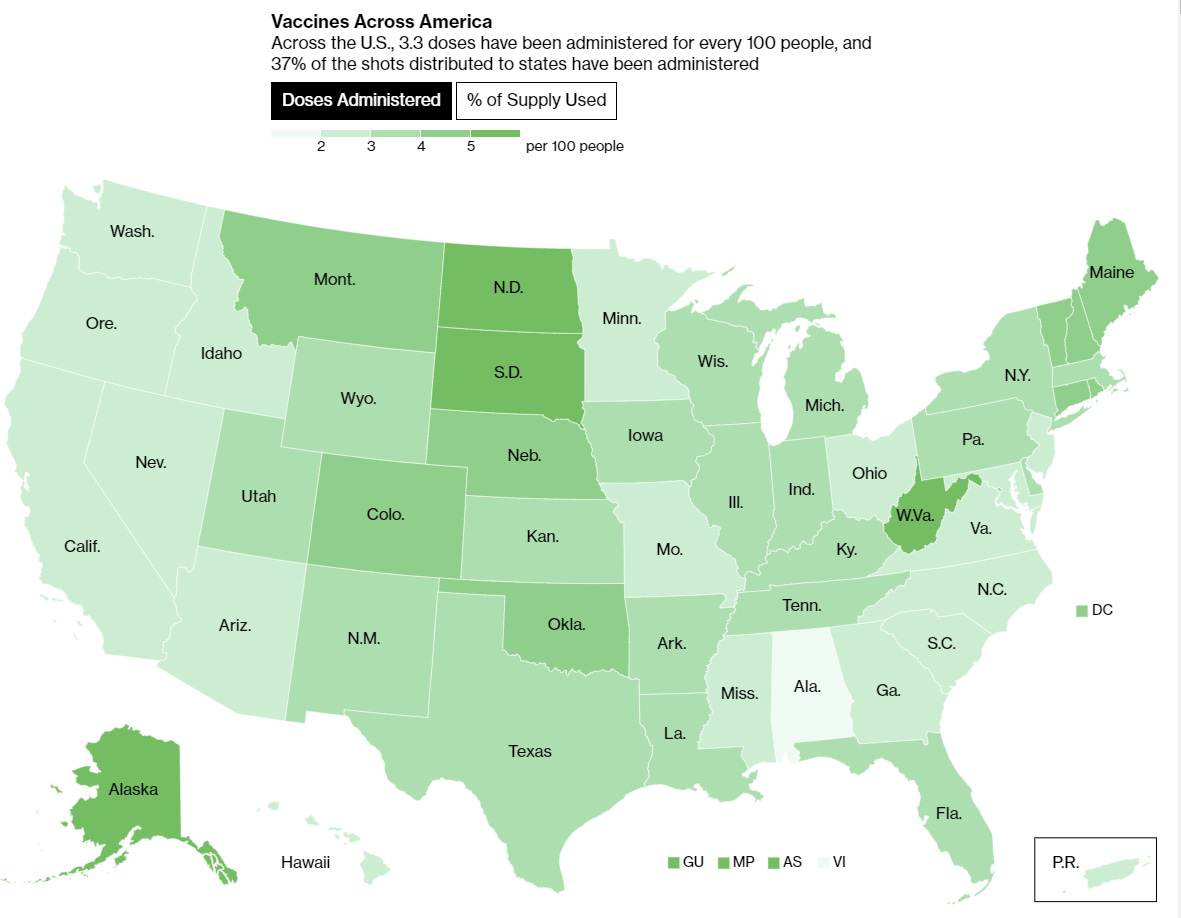
That doesn’t mean this isn’t a horrible, no good, very bad performance. Only 37% of all distributed doses have been given, with some of them ending up in the trash by choice. We need to do much better.
The good news is that things are accelerating, and so far decisions made by the incoming administration are highly encouraging and should speed things along further. As I’ve noted before, doing things fast early on is crucial since gains compound, but the real game is ensuring that as we scale up supply we are ready for that, and it all gets shot into arms, and we don’t let supply go to waste.

Europe
In the interest of consistency I’m not going to alter who is on the graph, but see the next section for a discussion of Ireland.
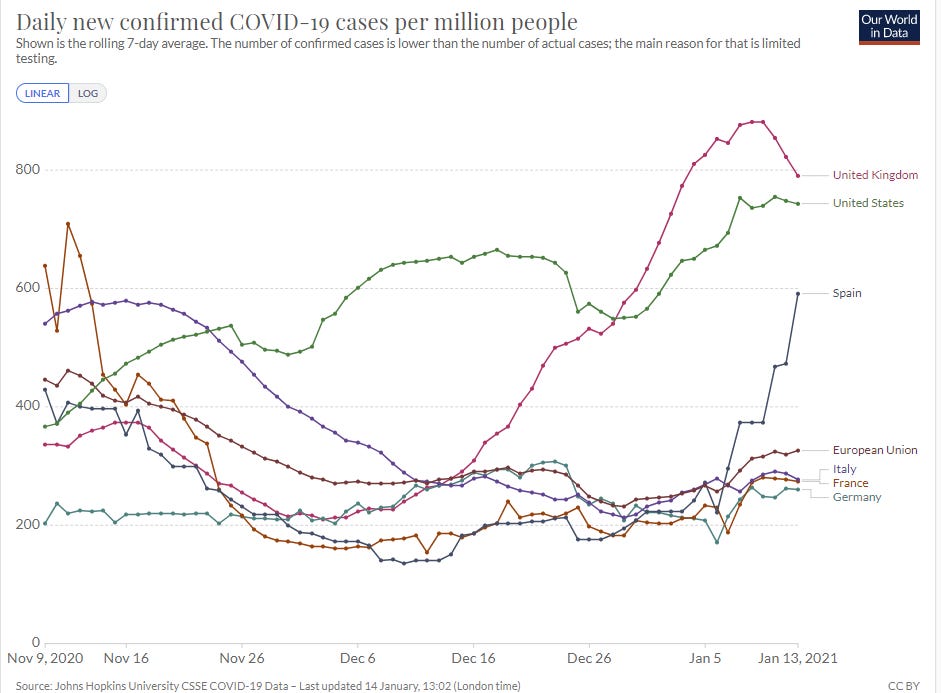
From what I see it looks like the Spanish hockey stick here is not due to increased testing. I also don’t know any sequencing data from Spain, so we don’t know if the new strain is involved here, but this rise is too fast for that to even be a full explanation, either there or in Ireland.
The most interesting part of all these graphs are those last few days from the United Kingdom. Positive test counts are declining again, as is the positive test percentage.
Did the control system manage to pull it off once again?
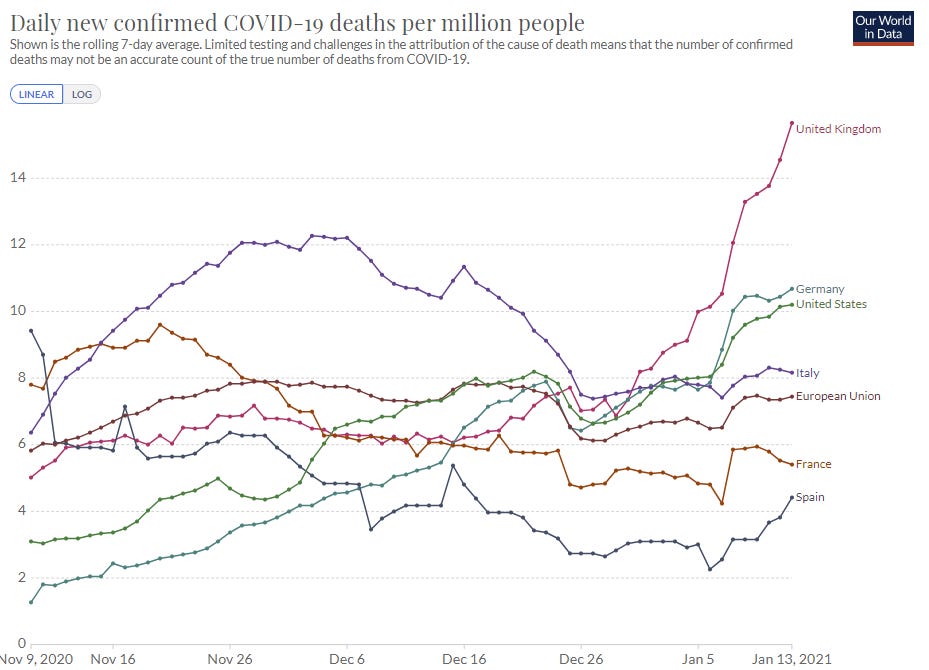
Even if that did happen, things got quite bad before that happened. The death rate in the UK is now 50% higher per capita than it is in the United States, and they have several weeks to go before that is likely to stabilize, so it’s likely going to go at least 25% higher than that.
Despite that, this seems like it happened, and it happened fast, and it shows that the control system does have enough ammo left to stabilize matters if those involved care enough to do so. I’m highly skeptical the United States could match this performance, even if the United Kingdom does sustain things from here, especially before things get much worse than they are right now in America.
Still, one must acknowledge that this happened, and without much vaccine help, and we should update our expectations accordingly.
Also worth noting is that despite their massive lead in vaccinations, Israel's short term situation in terms of cases is quite bad. They test a lot, so their positive rate is still only a little over 6%, and their death rates remain well behind ours, but it’s clear that the vaccines have not let them turn the corner on infections yet despite being over 20% complete. I do expect them to turn the death rate corner soon, since so many of their vulnerable are now protected, but it seems infections are continuing to rise.
This seems like more evidence that people have the perverse response of increasing risk taken when they are about to get the vaccine, due to some sort of risk budget or perception of risk, and a sense that ‘it’s over,’ rather than seeing it as the time to be extra careful. That’s not a good sign.
The English Strain: Are We F***ed? Is it Over?
We’re fucked. It’s over.
That still leaves plenty of room for our decisions to matter, and determine how bad things get before they get better. The strain is not growing as rapidly as we feared. This is going to suck, but my attempts to model things have me more optimistic that we can vaccinate enough people to muddle through without things getting too bad.
But the central assumption seems clear. The strain is here, and it’s going to take over by March.
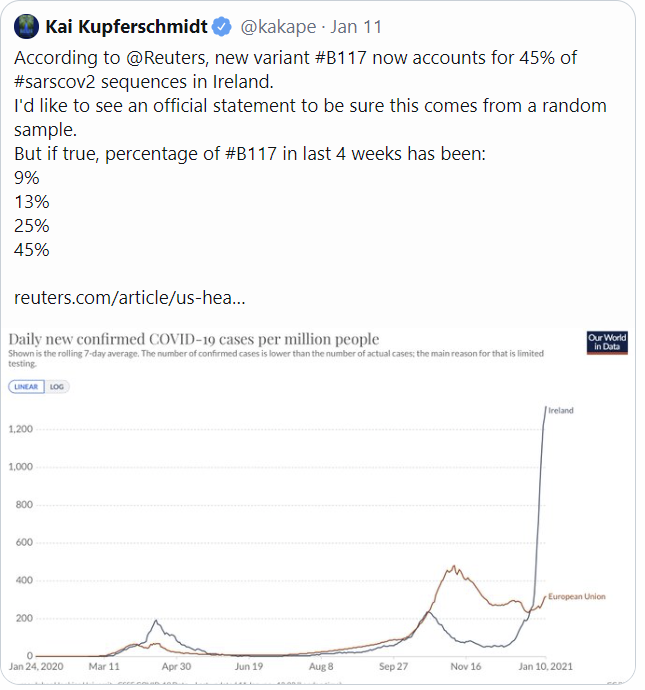
Ireland is being overwhelmed by the new strain, and it’s about as bad a graph as we’ve seen (link to Reuters):
Here’s the data from Denmark, suggesting 59% additional infectiousness.
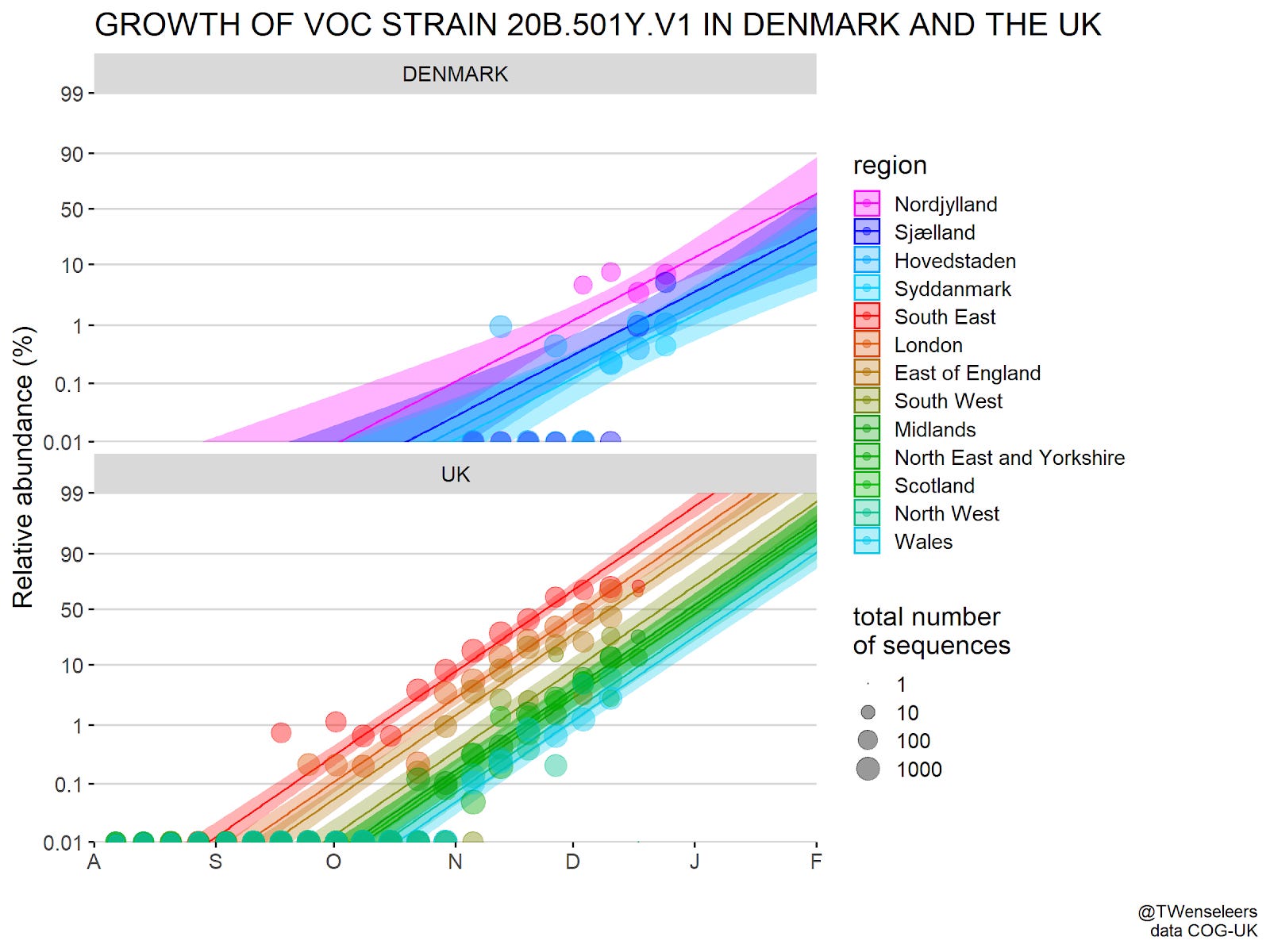
Here’s another data source that gives these results:
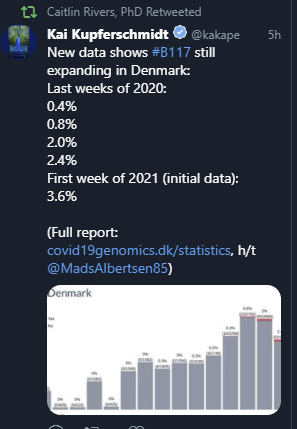
The good news is that this is noticeably less than one doubling per week.
There seems little remaining doubt over the infectiousness or growing presence of the new strain. The only question is what we do about it, and how bad things are going to get.
So, how far along is this? Here’s a guess by Helix posted on January 11:
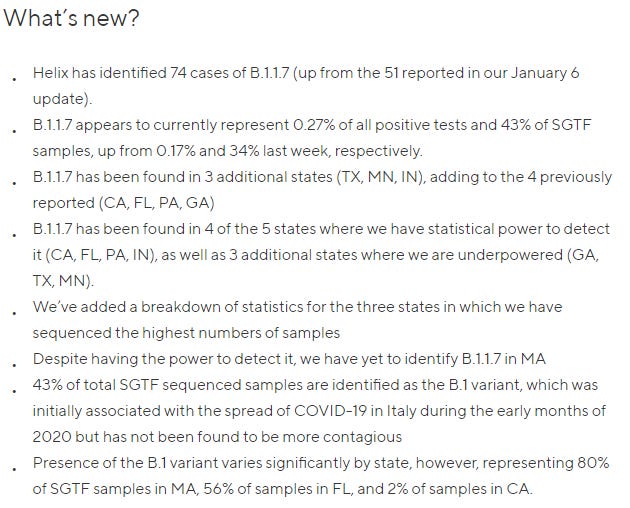
This is not a complete listing of sequencing tests, only listing the places they have the statistical power to look. New York last week identified four cases, three of which are linked and one that was distinct from the first three.
Also note the sample sizes here for SGTF-positive samples are not large until recently.
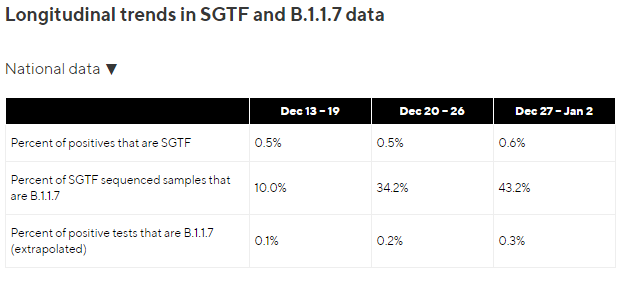

The data for that final week seems reasonably robust, so I’m down with saying that tests completed that week are 0.3% positive for the new strain. The previous weeks seem to have much less robust sizes, and the Dec 13-19 one is literally 1 out of 10, so extrapolation from that would be unwise.
Taken at face value, thus, this is all good news. We only have 50% week over week growth in cases detected, rather than a doubling each week. Even boosting that to factor in the first week of data, that’s a much slower acceleration than we see in Ireland. If we do have almost twice as much time and also the endgame isn’t as bad as feared, then that’s definitely a ‘we can muddle through this’ scenario.
In terms of where we are along the curve, 0.3% on tests done at the end of the year (which are presumably infections from a week before that) is modestly ahead of my previous estimates when I created my toy model, corresponding to a ‘starting strain size multiplier’ of about 4, and putting us about two weeks further along.
The South African Strain: Are We Even More Fucked? Is It Even More Over?
As far as I can tell, we continue to await the experimental data that will tell us for sure.
For now, what we do know is that the mutation common to both new strains does not interfere with the mRNA vaccines.
What we still do not know is whether the other changes in the South African variant do interfere with the mRNA vaccines, or to what extent this might compromise vaccine effectiveness. We can find this out easily if we use post-vaccination serum and see if it works against the new variant, but so far no one has done this, so we don’t know.
My father’s current best guess is that the vaccines will work for some people, but not others: “E484K is a radical mutation. E (glutamic acid) is negatively charged at physiological pH and K (lysine) is positively charged. Antibody to the epitope that includes 484 is not likely to work against the variant, but there are other epitopes that are targets for neutralizing antibody. That's why convalescent serum from some people, but not others, neutralize the variant. So my guess is that the vaccine will protect some people, but not others.”
I also have not seen any reports that this strain is being detected much in other places. That can be little comfort in an exponential growth situation, but at a minimum this problem is not as imminent as the English strain. Hopefully soon we will know more about the situation.
The “Columbus” Strain
When I posted about the English strain, the standard counter-argument was that mutations happen all the time, and new variations end up dominating all the time, and mostly it doesn’t mean much. With that in mind, we now have a third strain emerging, this one seemingly homegrown, that carries the 501Y mutation that is the presumed primary cause of the increased infectiousness.
It’s going about how you’d expect if that were the case: “This strain quickly became the dominant coronavirus variant in Columbus, Ohio, over a three-week period from late December 2020 to early January, according to the researchers, who hope to post their findings soon on the pre-print database bioRxiv.”
There are no signs this version is functionally different from the English strain in a way we’d be worried about, so presumably all this does is speed up the timeline. The mutation is already dominant in a mid-sized city.
What jumps out is that this is now three new versions with this mutation, emerging now.
Twice can be coincidence. Three times is enemy action. So, presumably, either there’s a common origin for these strains in some way that seems implausible, or this mutation is suddenly very likely to emerge.
I don’t know yet what to make of this development. The evolution is sufficiently fast and the timing sufficiently wrong that the vaccines can’t have anything to do with it, especially since it looks like they still work. It could be some combination of many more cases plus luck, which is kind of a coincidence, yet I want to be suspicious of such explanations.
But What Do We Do Now?

As opposed to, well, deciding to instead do the opposite:
Two Dose, One Dose, Who Knows, You Knows
One piece of great news this past week was the Biden administration announcing they were shifting to at least the weak form of First Doses First, and it’s happening. We will release all our vaccine doses now, and count on future supply to provide any second doses. That’s not a full ‘delay second dose to get more first doses’ policy, but at least it is a ‘a first dose now is better than delaying everything by weeks to be certain the second shot will always be available if there are supply disruptions’ policy.
That both has a big direct impact, and also gives hope that we might see additional helpful policies from the Biden administration.
As Tyler Cowen points out, the most striking thing is that once the new policy was announced, everyone ‘fell in line’ with it and neither of us has seen a single objection, because now the new policy is the default.
He also points out that there was never an expected value case that could be made in defense of the policy of holding back doses. The simple argument for First Doses First is not only compelling, it is overwhelming. If you can make two people 80% protected, or make one person 95% protected, and you want to turn the tide of a pandemic and protect people, that’s that.
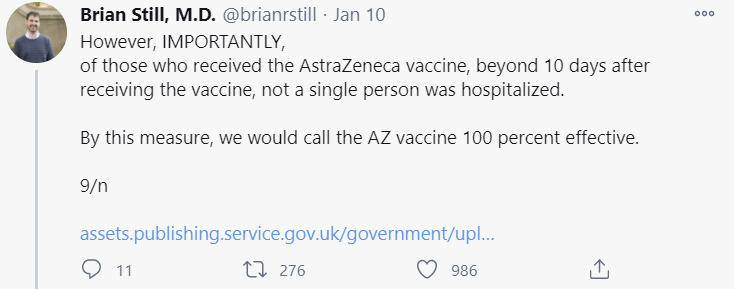
Last week I was linked to the only plausible objection one could raise, which is a claim that the 80% number is not accurate, so that should be addressed:

Is that so, Dr. Peter Marks of the FDA? Excuse me while I pull out the “hot damn, look at this chart” response from the data:
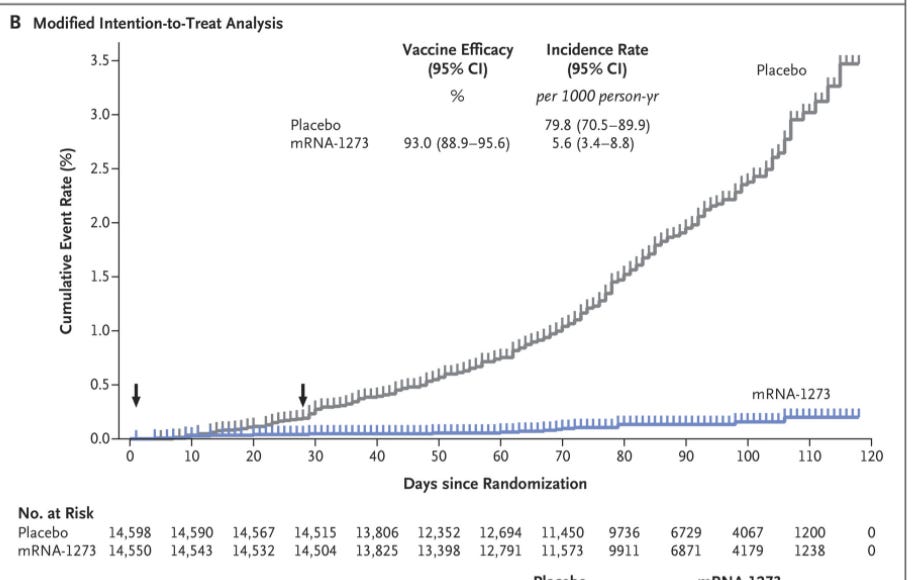
Let’s zoom in a bit:
So... does that look like it’s less than 80% effective between day 10 and day 28?
Or in chart form:

If we assume that infections after day 10 show up after day 14, we could reasonably look at the “14 Days after dose 1 to dose 2” part of the chart as the relevant one, and the score is... 35-2. That’s actually way more than 80% effective.
The question of duration of that protection is less obvious, but based on experience from prior vaccines, and the protection gained via infection, it seems highly unlikely that we will see big drop-offs within the first few months. There is a reason booster shots are often given a year or more after the first dose. If we do see such drop-offs, as Marginal Revolution points out, we could easily change our policy, and then administer the second dose at that time.
I’d also point out that Dr. Marks says that duration and depth of protection are potentially correlated, which seems very reasonable. But that means that if depth is strong, as it seems here, then we should expect duration to also be strong.
Yes, We Can Agree Andrew Cuomo Is The Worst
Last week, Andrew Cuomo was the worst because (among other things) he took the following steps, which are what you’d do if you wanted doses to end up in the trash:
Severely restricted who could get the vaccine.
Including not allowing vaccinations for 75+ or any other age band.
Gave contradictory and confusing answers about who was or would be eligible for vaccination.
Authorized vaccinations for different groups with no warning, such that county officials (let alone citizens) had no idea what was happening.
Spent his bandwidth threatening anyone who skipped the queue or let someone skip with severe penalties.
He carried those threats out in at least one case, confiscating vaccine doses from New Rochelle that tried to vaccinate its first responders, and fining the town, per DeBlasio.
He then threatened those who didn’t use their full vaccine allocations quickly.
Was actively ignoring pleas from NYC Mayor DeBlasio that he wanted to vaccinate and didn’t have anyone he was allowed to vaccinate.
I didn’t notice in time for last week’s update, but it also became increasingly clear that the #YouHadOneJob of vaccinations, residents of nursing homes, was going, shall we say, Not Great, Bob:
At this point, of course, it is ultimately their fault, they are in New York City, so all they have to do is fill out the proper online forms:

They are lucky they have a website at all. Here in Orange County, no officials had any idea what was going on for days when we asked, and there was no website on which to book. Phone calls were the only option. Lots of phone calls, and waiting lists.
Many of which turn out to be the wrong places. Here’s Erie County getting not all that many calls with no ability to book appointments that way:

The thing is, yes, Andrew Cuomo is absolutely The Worst, but New York isn’t actually doing so badly in terms of shots in arms. We are actually doing slightly above the mean on that metric.
We could, for example, be Virginia (MR). That link walks through exactly how trivial the logistical issues with vaccine distribution (as opposed to manufacturing) would be if anyone cared about solving them.
Which means that other states are doing things that are, on average, even worse than this, in terms of getting shots into arms. As PoliMath notes, New York is full of people looking for bad news. I’d add it also has a governor not only causing much of that news, but striving to make us as aware of much of that news as possible. Think about what kind of disasters you would find elsewhere with the same attention.
Meanwhile, back in New York, the situation is fluid, and in important ways it is vastly improving.
Cuomo did the most important single thing he had to do prior to being told to by the CDC, which was to open up things to Group 1B, which includes everyone over the age of 75. Then things were extended to those over the age of 65.
There are now more than enough arms in which to inject shots, and the most important arms are among those in which shots can be injected. And there’s more clarity on who exactly is eligible in addition to the elderly. And he skipped the Bills game. That’s all great. Credit where credit is due.
The flip side of that is that there are lots of other arms that are also eligible, which are more likely to have success navigating the systems and getting an appointment they can use. So we should expect a lot more stories about the elderly being unable to get appointments, while young people working in administration get slots instead. As you do. But it’s still a vast improvement.
Also that it seems we’ve decided that a lot of the state’s focus should be on the “climate crisis” where we will somehow lead the way. Aren’t you, I dunno, kind of busy, sir?
It also seems he’s going after a record that was previously (I can only presume and won’t check) was held until now by former Arkansas Governor Bill Clinton, and which we thought would never be broken:
On a personal level, I can report great success. As a health care worker, my wife called infinite places, got exactly one of them to call her back, and got her shot over the weekend. Armed (partly by me) with the information on how to book, the proper urgency and reasonable skill at using the internet, my elderly parents, both over 75, got their first shots on Monday morning in New York City. This is a great relief all around, even though I will likely be waiting many months for my turn.
Meanwhile, Cuomo has noticed that testing is a thing we could do a lot more often, but rather than use it to solve a pandemic, he’s going to use it to reopen entertainment venues and office buildings:

I suppose there’s only room for one ‘actually stop pandemic’ thing, and the vaccine already called dibs. We have to respect dibs. We’re not barbarians.
If you are in New York, this is the official place to start arranging for an appointment.
Here’s an NYC-specific Twitter thread with a few additional links and thoughts. The author of that thread has offered to help anyone in NYC who needs assistance navigating the system and booking an appointment.
All I Want At This Point is to Sell Out of Covid Vaccine
There are three potential bottlenecks for Covid vaccine distribution. You need shots to put into arms, you need professionals to put those shots into people’s arms, and you need arms in which to put the shots.
The guideline to extend to over 65 has been issued by the CDC.
We fixed the first bottleneck, at least where the CDC’s guidelines are followed. The elderly are eligible now. Wonderful! Time to make an appointment. There’s a problem:
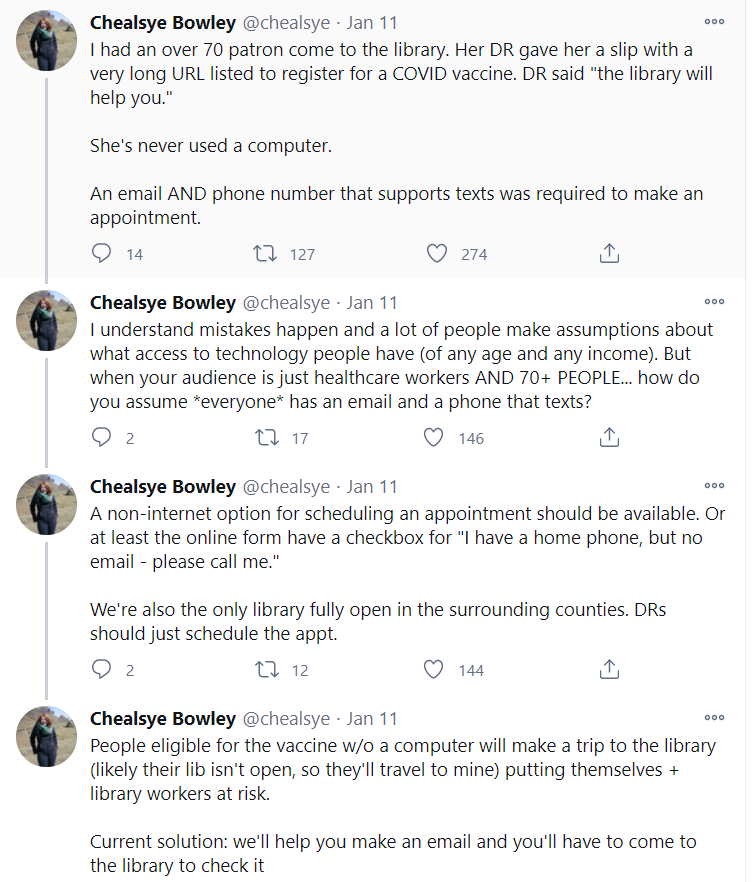
A lot of elderly people are not going to be able to get through this process, and a lot of others are going to get infected on their multiple trips to the library.
How is all that going to go?
We can start with how it’s gone so far:
Let’s check the predictions over at Hypermind, where the numbers haven’t moved much this past week:
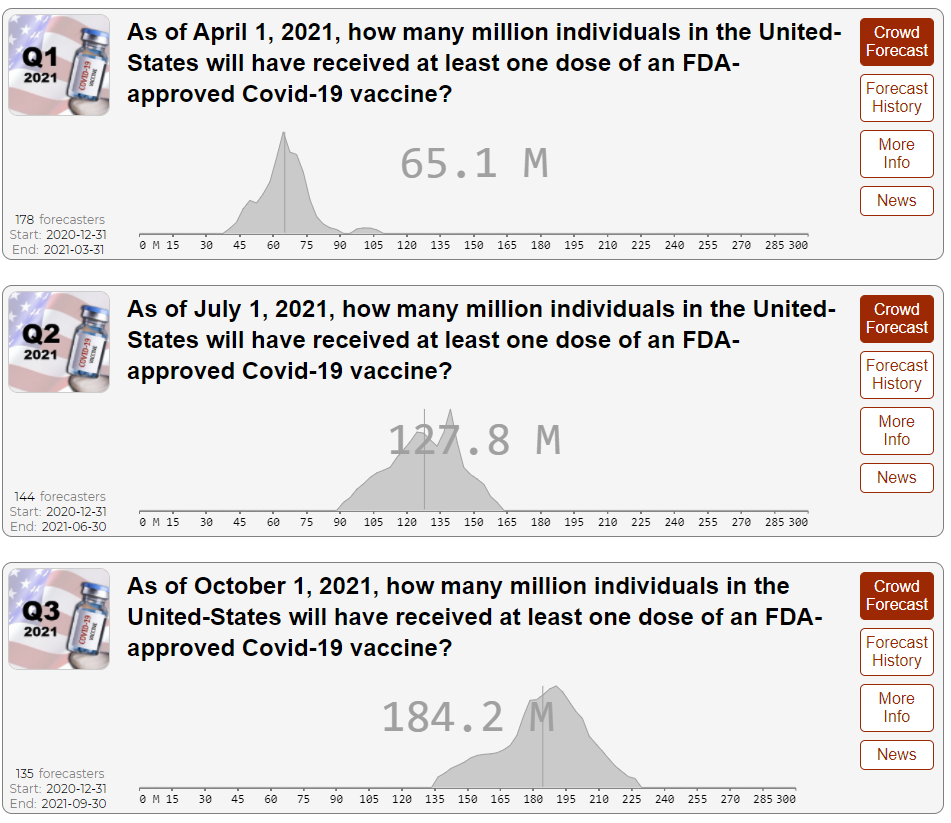
This is more optimistic than my naive Covid modeling. I had about 38 million vaccinated by April 1, 81 million by July 1, 131 million by October 1, so they’re also predicting roughly linear progress but have it happening a little over 50% faster.
I hope these predictions are right, or better yet pessimistic. The difference in those guesses is a really big deal. If we take my model’s guess and boost vaccinations an additional 50%, and the additional infectiousness of the new strain is only 50%, we plausibly (mostly) stop the fourth wave, despite the new strain currently being ahead of my previous guess for that. I’ve added knobs in the spreadsheet to vary both numbers.
Under the optimistic scenario, this increased vaccination pace would be the difference between ending with 40% or 50% of the population having had Covid-19 when it’s all over, with about 24% having already been infected. So this would prevent over a third of all future infections. Speed matters more than anything.
There are 209 million Americans over the age of 18. Given how many don’t want to be vaccinated, these predictions above imply that by April 1 you can likely get the vaccine as long as you care about finding it, and by July 1 you can get the vaccine provided you want it at all, as there would be enough vaccinations to cover every adult who wants one at all.
What about the Good Judgment Project?

That’s distributed doses rather than vaccinations, but by then I presume those numbers will be similar. This market seems overconfident in the timing, even if the median of early May is reasonable. In general, I find Good Judgment prediction markets to be overconfident.
It is worth noting they were deeply overly optimistic about how much distribution we would get in December and January, as were essentially everyone as far as I could tell, and it seems to have taken them far too long to realize their mistake.
Meanwhile, proper epistemic procedures are in place at MIRI:
I like Nate’s side of this bet and think Anna’s 2/3 estimate is a little bit low, given how much I expect Eliezer and Nate to make an effort. They should usually be (in effect) very near the front of the no-priority line.
Vaccine Allocation By Politics and Power
Headlines that tell the story and don’t require a click: Who can get the COVID vaccine in Florida? Hint: It helps if you have donated to a hospital.
There’s an extra advantage to 24-hour vaccinations, as they give an efficient way for people who aren’t allowed to pay money to bid on getting the vaccine. Who cares about it most? Offer some highly inconvenient appointments and see who shows up:
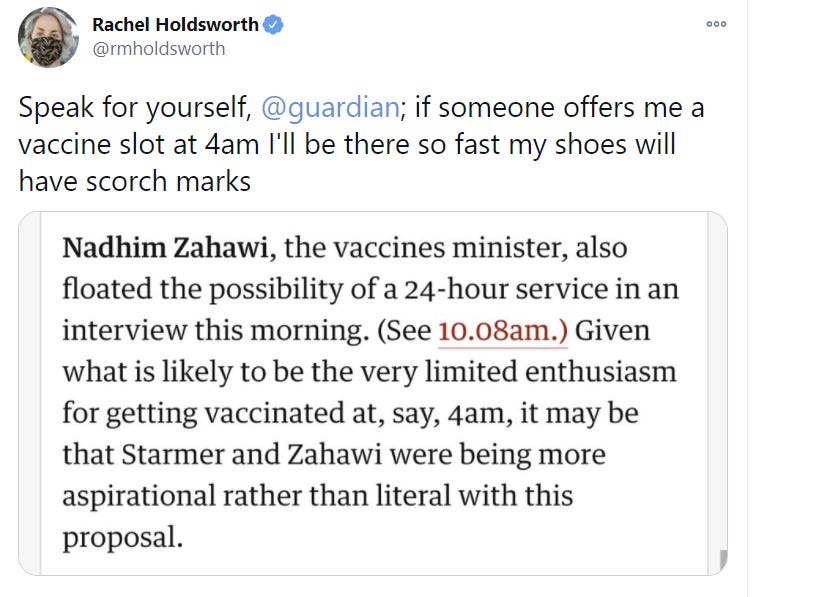
Believe me, I would happily show up any time, day or night. We’re about to find out if I’m alone in that, which I am very confident that I am not:

The list is growing. We also have the Washington Heights Armory.
Not listed is the best mega vaccination site, Citi Field, home of the newly owned-by-someone-who-cares-about-winning New York Mets, which will start on January 25.
Maryland’s headline choices, prior to the new CDC guidance, where teachers were to go before those aged 65-74, and 8% of the population is in front of those over 75:
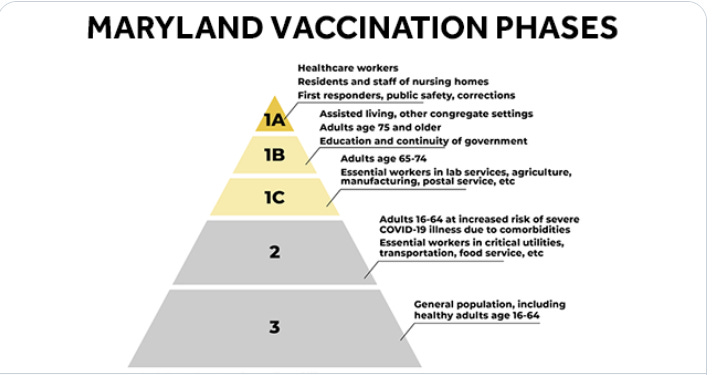
Or to be as clear as possible on what was going on as of January 11, prior to the new guidance:
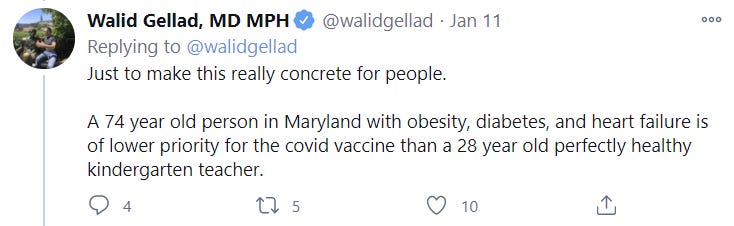
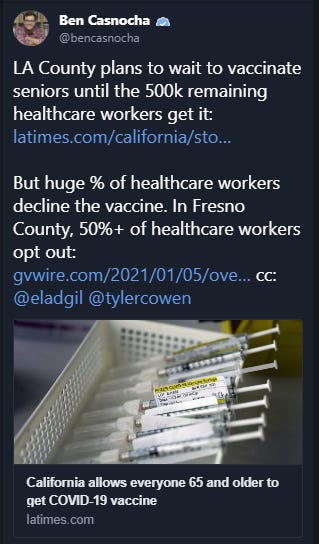
Meanwhile, the latest from Los Angeles (2nd link from post), where we keep getting signs that things are being handled especially destructively:
Do Not Throw Away Vaccine Doses: Somehow a Section Title
I am mostly doing a solid job of not getting angry about how things are going. I make an exception for when people literally throw out doses of vaccines.
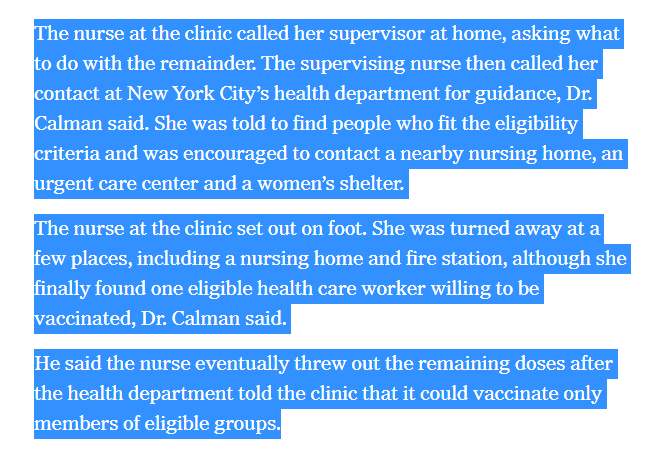
Fortunately, also in Cuomo’s New York, some people realize it’s not the incentives, it’s you and decide not to do that. Obviously vaccinating a 26-year-old healthy reporter is not ideal, but it’s infinitely better than throwing the dose out.
In the former control group, Sweden is throwing out the extra vaccine doses in Pfizer vials, because we might dislike the FDA but at least we don’t have to deal with the European Medicines Agency, who are totally Delenda Est Club members:
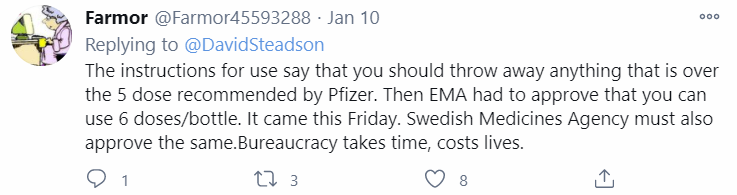
But good news, they could soon give the go ahead to stop throwing away vaccine doses.
England by contrast has moved on to doing distribution via pharmacies. Brexit has had some very high costs and was not pitched to the people remotely honestly, but getting away from European Union regulatory bodies while one has the chance should not be underestimated.
Also, there are some things you should definitely not do if doses are about to expire, because they’re technically dangerous, and against the rules, and set bad examples, and reasons, and they’re so bad I’m not even going to say what they are, but in any case please definitely do not do them.
Buy More Vaccine? You Can Do That?
I’m primarily not being sarcastic here, I’m actually still boggled can someone please explain what the hell is up with this:

I ask, because if Michigan is asking permission that implies that with permission they would be able to buy doses (from the factory, which is in Michigan) which implies there are doses still for sale that no one has bought.
Which seems utterly insane, but so does the idea that the Feds would be giving Michigan part of their allocation in this spot, which is the only other explanation I can come up with? But that does not seem like something the Feds would ever agree to do.
So I notice I am extremely confused, and hope someone can help me out on this one.
Also, it certainly does seem like the main bottleneck for solving the entire global pandemic much faster was indeed very small amounts of money combined I presume with regulatory barriers:
If true, and we’d been willing to spend approximately zero additional dollars, we’d already have all the doses we need. If true, we could still do it and have the rest of the world covered within the year.
Not doing this last year was... I mean I don’t even have the words:
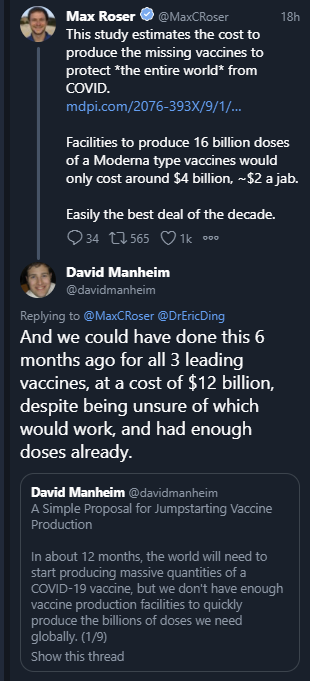
If this is all remotely true, then this was separately within the budget of dozens of countries and at least a hundred private individuals, many of whom are primarily philanthropists. None of them made a serious attempt to do this or even consider doing this (at least that we know about), is a very important fact to fit into your model of the world.
Approve Safe and Effective Vaccines: Somehow Also a Section Title
Your weekly reminder from Marginal Revolution that we should approve the AstraZeneca vaccine. No, really, we should approve it and I would happily accept it myself (link from screenshot):
Ensuring this happened would be my first order of business if I was the new President.
The second order of business would be approving Johnson & Johnson’s vaccine.
That’s right, the best news of the week is that this section title can be officially plural now, because we can welcome Johnson & Johnson’s one shot vaccine to the list. So we’re now waiting on multiple approvals.
Technically, we don’t know that it works. What we do know is it generates a robust antibody response. We won’t know the phase three results until later in this month, but if anyone thinks those results won’t be good enough to justify approving the vaccine, I will happily book your wager.
We have the information we actually need:

We won’t know exactly how well it works yet, but we know it’s safe and we know it’s a lot better than nothing, so all waiting does is kill people and prolong the pandemic.
Alas, we also got very bad logistical news from Johnson & Johnson. They will likely only be able to deliver a few million doses (only one needed per person) by the end of February, if results prove good and their application for emergency use authorization is approved. All help is welcome, and we should take it now and give them every incentive to move faster, but we were hoping for a lot more.
How Bad is it Out There Right Now?
It’s not great.
I was asked a few weeks back about the dangers of getting infected while getting your vaccine. This is a real worry, and is also the ultimate way to waste a vaccine dose and expose exactly the people we most want to protect. It was suggested that if things get bad enough during the fourth wave, that getting vaccinated might be so risky as to not be worthwhile.
I responded that while such infections will happen, it seemed super unlikely that getting the vaccine wouldn’t be worthwhile. Then you read descriptions like this one from England, via Stuart Ritchie, which I recommend reading in full, and it makes you wonder. There’s no question that what they are doing there is going to get a lot of people infected.
You Should Know This Already
We worked for weeks on a detailed set of prioritizations and procedures and regulations and approvals, and Israel just... gave out the vaccine to everyone as quickly as possible.
We sat around worrying about ‘wasting money’ buying too many doses, and now we don’t have enough, and Israel just... paid two to three times the “market price” to make sure it had enough doses. They also committed to sharing data to help make the deals go through. The rest of the thread has lots more info on how Israel pulled this off. And again, it’s all... they went ahead and did the thing. There was no shutting up and doing the impossible, both because nothing involved was remotely impossible, and also because what would be truly impossible is getting Israelis to shut up.
Alex Tabarrok reminds us that we should be doing preliminary testing now on vaccines for potential future pandemics.
John Cochrane righteously rants about our failure to approve AstraZeneca. He’s right but no need to click.
Alex also reminds us (in a repost) that experiments make people uneasy and suggests reasons. My understanding continues to be that the experiment result is largely about The Copenhagen Interpretation of Ethics and Asymmetric Justice, as one who experiments is now responsible for all potential harms and all potential lost benefits, as well as all potential or realized inequalities, and for trading off any and all sacred values, while getting none of the credit for anything since the choices were randomized.
Do not click on this because it is a case of Something is Wrong on the Internet, but I needed an example of the sort of insane scaremongering guidance that is being given to many people that they should remain paranoid even after being fully vaccinated. And thus say things like this:

This is obvious nonsense. If it is reasonable for you to consider doing full quarantines after getting fully vaccinated, I can only deduce that you are either immune deficient or have a dead man’s trigger that launches nuclear missiles.
At some point we have to call such sentiment what it is, which is that it is opposed to and incompatible with life. One should also look at all similar recommendations made in other circumstances in light of its inability to adjust to circumstances. You should be skeptical of cries of “Wolf!” from people who keep saying “Wolf!” no matter how obviously there is no wolf.
You Should Know This Already in the sense that this screenshot has a 1 where there should have been a 0:
Reminder that this Covid tracker exists for NYC.
Fans were not socially distancing after the National Championship game.
In Other News
From the CNBC Johnson & Johnson article linked above, we also see this tidbit worth noticing and applauding, because incentives matter, and they matter more than you think even after knowing this fact:

Wired covers the micro-covid project at length.
The University of Wisconsin used rapid testing and managed to catch 80 percent of cases with symptoms and 41 percent of asymptomatic cases. The article chooses a somewhat different framing.
A question that needs to be asked, if you have good additional info not in the thread please share:
Another source of weekly Covid updates is Tom Frieden. I’d skip it, but figured I’d note it exists. There’s a lot to like here, but it didn’t teach me anything new, and it reflects the moralizing explanation of Covid spread. There’s some ‘luck’ from super spreaders but otherwise it’s all about whether you did enough sacrificing, or you didn’t do it right or didn’t do it for long enough, and the goal of writing such updates is to scare people into bigger sacrifices.
I have no idea why Dr. Moncef Slaoui, the head of Operation Warp Speed, was asked to resign and transition things over to someone else. Seems like if someone does their one job this effectively you’d want to keep them around.
After being confined in a room for hours with a number of Republican congressmen on Wednesday, January 6, you know, because of reasons, Congresswoman Jayapal tested positive for Covid-19, and is now in quarantine. She reports: “The duration in the room was multiple hours and several Republicans not only cruelly refused to wear a mask but mocked colleagues and staff who offered them one.”
Youyang Gu of the Covid Machine Learning projections notes that there is essentially no correlation among the US states between current infection rates and estimates of existing immunity. One could interpret this as places that are more vulnerable having had more infections, and thus now having more immunity but doing so from a baseline of greater vulnerability. Certainly the correlation between state precautions in the past and state precautions now is positive. If one sets ‘effect of accumulated additional immunity’ equal to ‘effect of the conditions that caused those infections’ then that gives us a model we can test.
Never let a crisis go to waste, medical innovation edition, as mRNA vaccine tech is applied to multiple sclerosis, here’s the paper in Science (login required). Next up: Nipah, HIV and seasonal flu.
It’s still early, but still. Note that lack of speed doesn’t kill as effectively here, but lack of speed still kills here, too.
Also, off topic, to end on a positive note, if anyone wants to never feel cold again, I’m here to report back: The coat is here, it is real, and it is spectacular.