

Covid 10/22: Europe in Crisis

America’s Covid-19 situation has clearly entered a third wave. Cases and positive test percentages across the country are rising steadily, and deaths are finally starting to follow suit over the last few days. The scaremongers greatly oversold things, but that doesn’t mean there isn’t a problem, especially in the Midwest. My biggest worry at this point is that this wave could lead to ineffectual but damaging attempts at additional lockdowns. My biggest hope is that this will let us rush the vaccines out there faster and the control systems will kick in within a few weeks, same as they did last time.
Europe’s Covid-19 situation is much, much worse. They controlled things without going for eradication and without establishing proper long term containment strategies. Then they tried to reopen exactly the maximum while keeping containment, which failed. Now they’re paying the price. European case counts are skyrocketing and have passed 100,000 per day. Within a few days they will almost certainly pass America in deaths per day as well. Hopefully my readers over there can provide more insight and good sources to follow, and we can see if this can expand to cover Europe more over the next few weeks and months.
I’m further improving the order in which I post the numbers, and finally starting with the positive test percentages, so we start with the most meaningful non-lagging indicators.
Let's run the numbers.
Positive Test Percentages
PercentagesNortheastMidwestSouthWest8/20 to 8/261.86%5.78%9.93%5.88%8/27 to 9/21.87%6.37%9.38%4.78%9/3 to 9/91.97%6.02%8.48%4.13%9/10 to 9/162.41%5.99%11.35%4.49%9/17 to 9/232.20%5.96%7.13%4.11%9/24 to 9/302.60%6.17%6.18%4.27%10/1 to 10/72.61%6.05%6.74%4.23%10/8 to 10/142.57%8.14%7.09%4.75%10/15 to 10/222.95%8.70%7.85%5.36%

Test Counts
DateUSA testsPositive %NY testsPositive %Cumulative PositivesAug 13-Aug 195,293,5366.2%548,4210.8%1.68%Aug 20-Aug 264,785,0566.0%553,3690.7%1.77%Aug 27-Sep 25,042,1135.5%611,7210.8%1.85%Sep 3-Sep 94,850,2535.3%552,6240.9%1.93%Sep 10-Sep 164,632,0055.8%559,4630.9%2.01%Sep 17-Sep 235,719,3275.2%610,8020.9%2.10%Sep 24-Sep 305,857,0975.1%618,3781.1%2.19%Oct 1-Oct 76,025,6335.2%763,9351.3%2.29%Oct 8-Oct 146,324,8335.8%850,2231.1%2.40%Oct 15-Oct 216,434,9726.4%865,8901.2%2.53%
For the second straight week the positive rate grows by 10%, or about 0.6% in absolute terms, while the test count shows a small increase. This week, that increase was evenly distributed across all four regions.
Positive Test Counts

DateWESTMIDWESTSOUTHNORTHEASTAug 20-Aug 26675456654013232218707Aug 7-Sep 2550007540112741421056Sep 3-Sep 9472737243910640821926Sep 10-Sep 16450507526411581223755Sep 17-Sep 23540258538112773223342Sep 24-Sep 30554969293210630027214Oct 1-Oct 7567429724311017034042Oct 8-Oct 146828412574411799538918Oct 15-Oct 227557114985113323843325
Regionally this is a steady increase across the board with all four increasing by roughly 10%. If we break it down by state, we see bigger contrasts.
In the West region, the coastal states seem to be doing all right, with California, Washington and Oregon all holding steady, and Hawaii still actively improving. Everyone else’s counts are up 50% or more over three weeks, many of them 100% or more. Other than Arizona, all those other states are setting all-time high case counts.
In the Midwest region, Iowa, Oklahoma and Kansas, and to some extent Missouri have this contained for now to only small increases. I’m not sure why Wikipedia puts Oklahoma in the midwest either. We see 90% or bigger three-week jumps in Ohio, Michigan, Indiana and Illinois. Others are somewhere in between.
In the South the scariest numbers are from Kentucky and Tennessee, with the deep south headed in the wrong direction but slower. Florida is up 30% over the three weeks, Texas only 14%.
In the Northeast, Vermont, Connecticut, Rhode Island and New Hampshire are up over 100%. New York, New Jersey and Pennsylvania are up over 50%.
Things are not contained across the board, with only California and Hawaii not seeing increases. The question is where these increases lead, and what they cash out into.
Deaths
DateWESTMIDWESTSOUTHNORTHEASTAug 20-Aug 2615037453876375Aug 27-Sep 212457593631334Sep 3-Sep 911417712717329Sep 10-Sep 1611599543199373Sep 17-Sep 2310168932695399Sep 24-Sep 309349902619360Oct 1-Oct 779711032308400Oct 8-Oct 1478212172366436Oct 15-Oct 2180415912370523

When infections increase, deaths start going up about three weeks later. There was already clearly trouble in the Midwest, but it has accelerated quite a bit, to the extent that it seems plausible that we are starting to see the beginnings of hospital overload - there is a field hospital open, I believe in Wisconsin, already. The overall death counts did not start rising again until Monday the 19th, but since then the trend seems clear.
We are finally starting to see increased deaths. It is late October with 10 weeks to go in the year, so getting to 400,000 deaths by year’s end still seems all but impossible, but that was always an arbitrary scare tactic number rather than an attempt to model anything real.
Overall, it seems likely that we will continue to see roughly 10% week over week increases in case counts, which will result in similar rises in deaths, until something changes. The Midwest has it worse, and there is some risk of overwhelmed hospitals there, which would make things worse still, although it’s hard to get a good read on how much worse.
Covid Tracking Project’s Visualization
I prefer my own graphs, but the project’s graphs certainly help tell the story. Here’s what they had through yesterday:
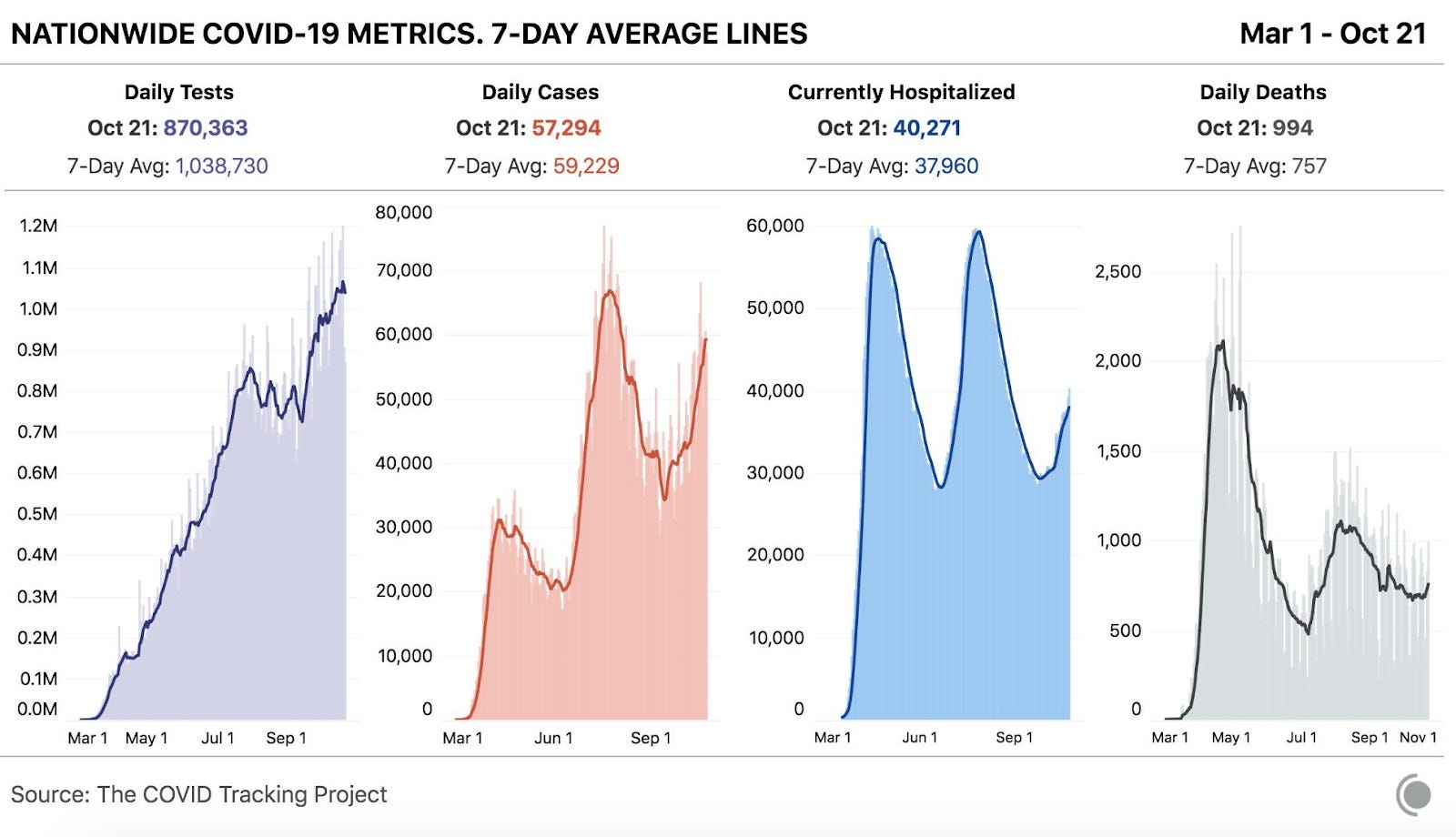
Tests mostly look like a linear increase over time. Daily cases have two peaks and a new third peak starting, with the second peak double the first. Hospitalizations in the first and second waves are roughly equal, partly because in the first wave they were turning people away, with the third wave starting to show. Then deaths peak in the second wave at half of the first wave, and are just slightly starting to show.
That progression tells the story of a disease becoming steadily less scary, only partly offset by improved testing and hospital capacity. Cases double, hospitalizations stable, deaths down by half. Things are definitely headed in the direction of more infections, but it’s not clear that will increase deaths by that much.
Why a Third Wave?
What’s causing this wave? What changed? I’ve written in recent weeks about various possible factors, which I am guessing are having a combined effect. In order of my guess of their importance, the issues are: People adjusting their risk tolerance as they notice Covid-19 has become less deadly, general fatigue with social distancing and other prevention efforts, colleges and related activities (much more about colleges here than primary or secondary schools but some effect across the board), rhetoric from leadership to ignore the virus, colder weather (minimal impact from this so far in many places, but the Midwest might be different). Testing has gone up, but we’ve adjusted for that and it isn’t going up that fast.
I see people as mostly making the reasonable and rational decision that the cost of marginal prevention is rising, while the costs of catching Covid-19 are falling, with some unreasonable signaling and tribal loyalty thrown in. It makes sense, when the disease gets less deadly, for the effective equilibrium of the control system to increase the number of cases to compensate, and it also makes sense that such adjustments are slow to course correct and therefore would overshoot.
Combine that with small structural additional changes, and the control system keeping case counts steady has broken down, at least for now. It will probably reassert itself on its own given time, as people make individual decisions to limit their risk.
Will there be another set of lockdowns if the corrections don’t come quickly? That is the big question now.
Why So Few Deaths?
Once again, a question that comes up every week. Now a story about how there’s even two official studies, so it’s real. Studies show! They find that 7.6% of patients hospitalized for Covid-19 die, versus 25.6% at the start of the pandemic.
A quote from the story, talking about an early Covid-19 case: “It’s not that we didn’t know what we were doing. We absolutely knew what we were doing. It was just there were unknowns there.” So we absolutely knew what we were doing, except that we didn’t know what we were doing. Which is fine! There was no way to know. Alas, our blame and credit assignment mechanisms don’t work that way, so we get quotes like the above.
Story notes that treatments have been systematized and improved, but is actually quite good pointing out that it isn’t clear this is what caused the change. The people who are infected tend to be younger and healthier. So, the story asks, which of these caused the improvement? Because that’s how the media has to frame a story, to see who deserves the credit and blame. The studies see death rates going down even when correcting for patient types, so they conclude that credit is indeed due.
There’s also this potential cause of a drop in death rates per hospitalization:
And Mateen says that his data strongly suggest that keeping hospitals below their maximum capacity also helps to increase survival rates. When cases surge and hospitals fill up, "staff are stretched, mistakes are made, it's no one's fault — it's that the system isn't built to operate near 100%," he says.
Or one could point out that when you don’t have room for healthier people, your death rate will be higher. At one point in the story, a doctor says that ‘many things’ caused the improvement, but he’s talking only about many improvements in what doctors do, because all credit must go to doctors.
No mention of mask wearing or other precautions decreasing viral loads, or even people coming in earlier because testing is easier and they know what to suspect and don’t think the testing site is a death trap. Or possible selection for people more susceptible to getting infected by the virus for unmeasured reasons also being more likely to die from it. Certainly no mention of possible virus mutation.
And of course, standard warnings about long Covid and hospitals filling up and how it’s still important to do ‘everything possible’ to prevent infection.
On the plus side, warning about 400k deaths by end of year here has become 300k deaths by February, which is a warning that could plausibly actually happen. Credit where credit is due.
My best guess order of importance on less deaths per real (not detected) infection is: Younger pool of infected, healthier pool of infected, available hospital capacity, lower viral loads, better treatments, not doing existing harmful treatments, better detection, more susceptible people getting infected first. The wild card is virus mutation, which might be no effect or might be number two or three on the list.
What Is Happening In Europe?
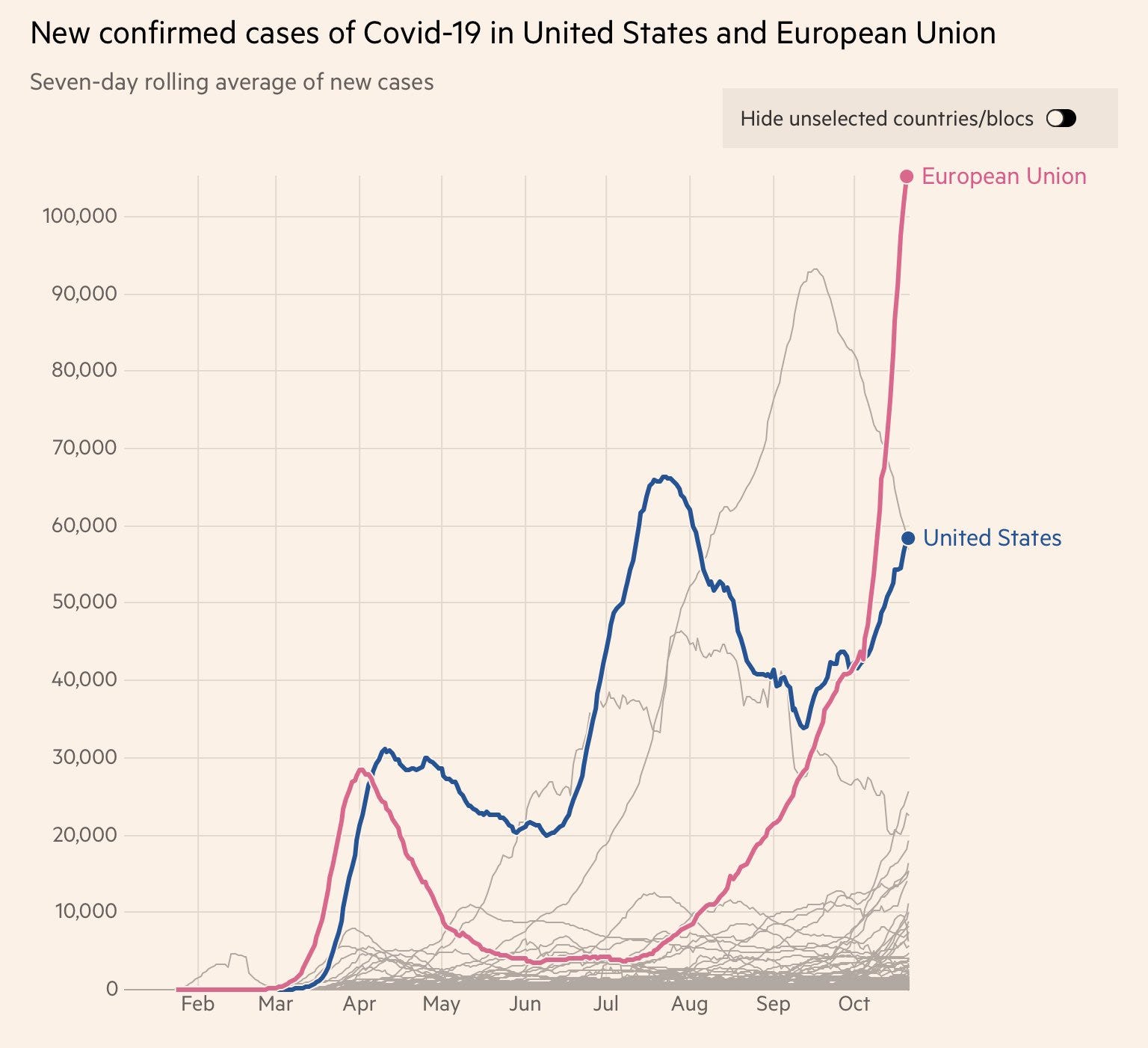
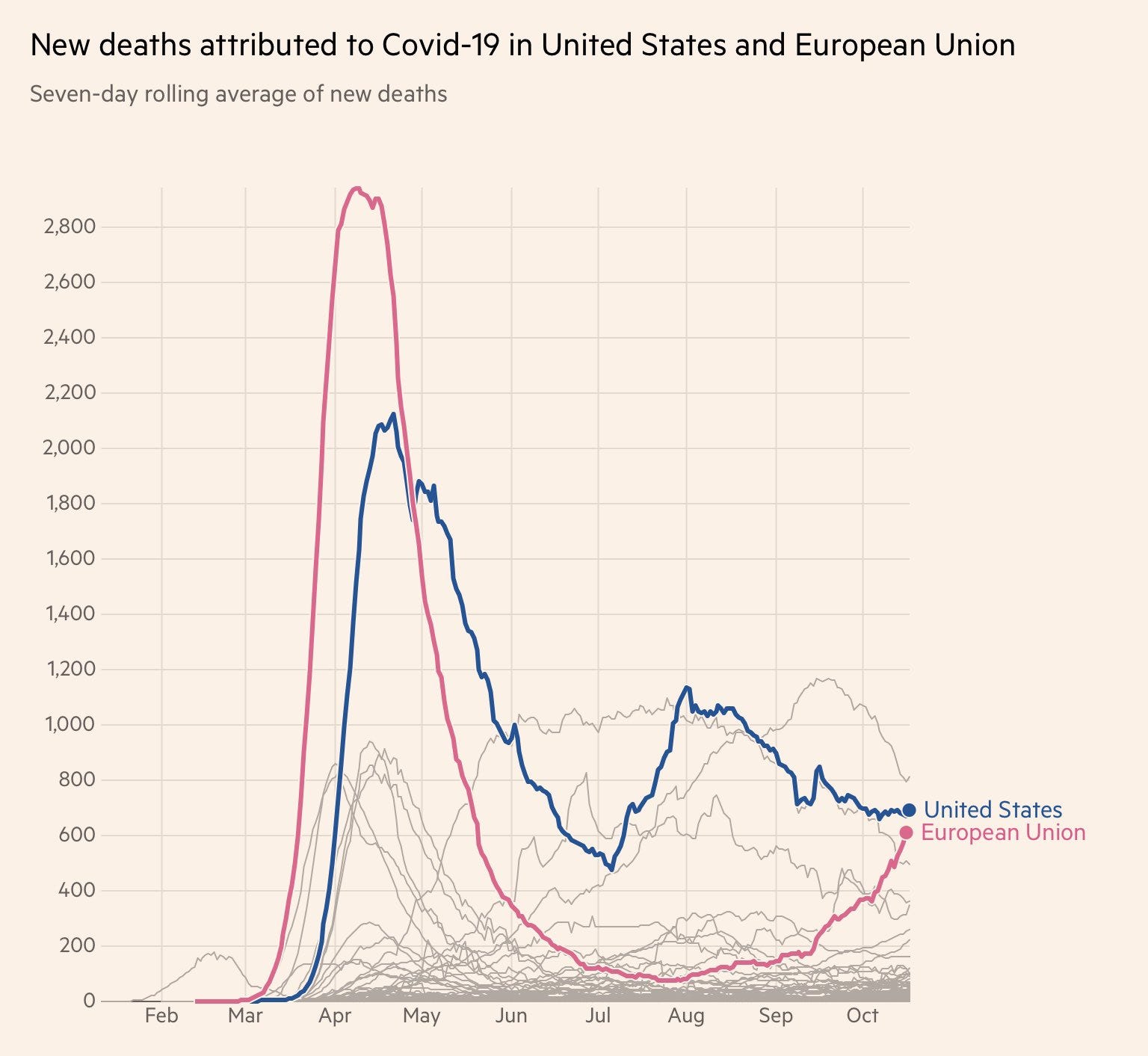
That is a far scarier set of graphs than anything we see in America. In America, we’ve had multiple waves, but from the low point of cases in June we only peaked about 350% of that, deaths only a little more than doubled. The graph never went full hockey stick.
Europe seems to have gone full hockey stick. Infections were contained for two months under 5,000 a day, and have quickly shot past us to over 100,000 a day. Deaths were stable under 100, and already crossed 600 despite several weeks of lag and that graph being several days older than the first one - at least one doubling from here is already baked in. These graphs are really scary. If left unchecked this would presumably collapse the European hospital systems in many countries within a few weeks.
I have not been tracking things in Europe enough to understand why this is happening there, but understanding it seems important to the puzzle. Something must have happened. I do wish I’d been watching Europe more from the beginning, but what’s done is done.
My best theory (and please keep in mind I’m speculating here) is that the Europeans didn’t have a strong enough control system of individual action any longer, due to their trust in authority and technocracy and the message that they had ‘won’, so there were no checks once the balance tipped too far and the dam broke.
When things were improving or stable, things slowly returned closer to normal. Rather than finish the job, the Europeans declared victory and left home. Things steadily started getting better slower, then got stable, then started getting worse faster and faster, they opened their universities without proper precautions, and they thought they’d won and were in good hands so no one did anything about it that wasn’t several steps behind. Just like in March. They assumed the responsible people in charge were taking care of it, except that there aren’t responsible people in charge except by comparison to America. Just like in March. Alas, reality does not grade on such curves.
What is very clear is that we are not “two weeks behind Europe.” Europe is likely headed into uncharted territory and moving much faster than we are. It’s going to get worse before it gets better, probably quickly.
Of course, no one on any side in America is pointing out this is happening. One side doesn’t want to admit that Covid-19 is getting worse and is a problem. The other side doesn’t want to admit that the people they admire as the responsible adults are somehow handling things worse than we are, or that by controlling things better earlier they may have set themselves up for a disaster now.
In all seriousness, check your country and region carefully, but if you are in Europe, you need to prepare for a new lockdown. One may well be imposed upon you soon, and you may want to go into one on your own even if it isn’t imposed upon you. Stock up on essentials, take care of any business you need to before things get even worse, and mentally prepare to hunker down.
My readers in Europe, can you shed more light on things? I don’t have good sources in my regular feeds, so insight and links are appreciated, especially good Twitter sources to follow and good websites to get statistics and other information. What’s the best European site that’s similar to the Covid Tracking Project?
Remdesivir
Does remdesivir help save lives, or does it only shorten recovery periods?
Science magazine reports that remdesivir and interferon fall flat in WHO’s megastudy of COVID-19 treatments, the preprint is here. As Tyler Cowen notes, the timing of the drugs is crucial to ensuring their effectiveness, and it seems like these studies are likely administering the drugs relatively late. Gilead’s response letter throws a general ‘you can’t mix all this random stuff together’ objection based on variation in what the hospitals did to get the WHO’s study done, and links to the good-looking one in the New England Journal of Medicine, which shows big mortality improvement.
The WHO’s study is bigger than Gilead’s, but both are plenty big enough, so there’s probably different things going on in the different studies. Those who know more about the science here that I’ve talked to mostly think that remdesivir early is a good drug but later on is not good, so my default hypothesis is that the WHO study was a mix of early and late administration. Note that that could still effectively make it a bad drug on a population level, if we’re not smart enough to use it when it is good and not when it is bad.
It seems clear that treatment of Covid-19 in general has greatly improved. This is an example of how it’s hard to know how much of that is due to any particular change.
What we do know about Remdesivir is it seems to be better administered early, and it shortens recovery time, and it won’t make you more likely to die. Even if it doesn’t make you less likely to die, that’s still enough to use it, unless it is crowding out other things, but there likely comes some point where it’s too late, and it’s not clear where that point would be.
F.D.A, Let Astrazeneca Resume Their Vaccine Trial
We’d like to resume it, and we’ve resumed the trials in England and Brazil. With those resumptions, thousands have been immunized without adverse effects, leaving only the initial issue that seems to have been in two patients, only one with clinical relevance. Which means even if it’s much much more common than it has been in the trial, it should in no way slow down anything.
Yet thanks to our F.D.A. (delenda est!) our trial remains halted. With America’s distrust of foreign data, who knows how long this might delay things. Those dastardly Europeans even use different file formats! Which it seems may have led to a month of delay before the data could be properly converted. Presumably because there are various regulations, so one does not simply convert such sensitive data.
A year ago, I’d have had a hard time imagining that America would cripple its entire economy rather than accept an alternative file format to explain away one or two adverse events in a several-thousand person clinical trial. Now it doesn’t even surprise me that much. I guess it does still surprise me a little.
Then, yesterday, a patient in their trial died.

Shares of Atrazeneca were down 1%.
Did I mention that the patient was In the control group? No? Whoops. Also, whew random chance.
One easy way to know is that the study wasn’t halted. If the death had been in the treatment group, the study would have been halted. So we knew the death was in the control group from the above picture alone, without having to wait for the confirmation.
Because the only way to test thousands of people for months is if none of them have any serious health problems whatsoever, despite the obvious high improbability of none of them having serious problems of one sort or another. And certainly none of them can die, despite there being thousands of people in the study with a life expectancy less than one hundred, and well, you do the math.
Meanwhile, the Chinese continue doing widespread vaccination, and their test results reportedly look good as far as they go, but doesn’t seem like much information, and also I said we should trust England’s data but this is China so let’s not go nuts.
Also meanwhile in completely insane “medical ethics,” Pfizer says if it wins emergency use authorization for its vaccine, it will immediately vaccinate the placebo group in its trials. We wouldn’t want to risk gathering additional information, so we should prioritize those placebo patients with our limited supply of the new vaccine, it seems.
Close Contact
CDC has finally updated its guidance on the definition of a close contact. Now 15 cumulative minutes within 24 hours counts, rather than only 15 minutes in a row. This seems like an utterly obviously correct adjustment, so it’s certainly welcome.
Alas, this is presumably the end of The Covid Shuffle, where kids got up every 14 minutes and changed seats so they would not technically become ‘close contacts’ with each other. Which did almost nothing to prevent the virus, of course, but did give the kids some well needed breaks and maybe even a little physical exercise. It’s also such a good Bavarian Fire Drill. It’s important to take victories where one finds them.
In case it needs saying here, there is no sharp distinction between close contact and non-close contact, and there is no minimum amount of time exposure to a person to catch the virus.
And no, Washington Post, this does not ‘make mask-wearing even more important for preventing disease.’ Our major newspapers can’t figure out the distinction between what prevents the virus and what is in written guidelines, or realize that the written guidelines don’t determine how the virus spreads. Wet ground continues to cause rain, film at 11.
In Other News
Good news, everyone! The San Francisco playgrounds are opening with only 1 adult per kid, 30--minute limit, crying kids need to be removed. After only seven months. What a glorious day.
NPR attempts to actually model parts of the physical world regarding infection. Nothing terribly useful, but still warms my heart.
If you wanted a Breathable Bacon Mask then good news, there is one available. Seems like a poor flavor choice to lead with, as a little bacon goes a long way. Still happy to see someone trying as there has been a decided lack of mask innovation. This is something the market should be there for, as we don’t need the masks to meet any standards so I don’t think there’s an important regulatory barrier? And everyone wants to look cool and feel more comfortable, so there’s gotta be a huge market.
It turns out that when you spend a lot of time and money, both fixed costs and marginal costs, to develop lifesaving monoclonal antibody treatments, the next thing corporations typically do is charge a lot of money for them. Seems legit.
Metastudy concludes that if you have ‘mild-to-moderate’ Covid-19 (an adjective that my brain still thinks only applies to people in American ads for brand name prescription drugs telling you to talk to your doctor about them) are highly unlikely to be infectious after 10 days, which we knew already. But if you have ‘severe-to-critical’ illness, which I didn’t think existed by that name even in ads for drugs, virus may be shed for longer. Which makes sense as far as it goes, so if it’s bad then presumably you should isolate until you test negative.
We expect Tier 2 British couples not in a bubble to refrain from sex. This is totally a reasonable thing to expect, will absolutely make a real difference as long as everyone keeps calm and carries on, and we’re definitely not in a young adult dystopian novel.
When school experiences get both unsafe and otherwise radically worse, in ways that destroy much of what is valuable about them, and still charge the same tuition, we are shocked to report that enrollment is down! 16% nationwide, and 22% in community colleges. And that’s terrible.
New York advises against non-essential travel to anywhere outside New York, including New Jersey, Connecticut and Pennsylvania. That means New Yorkers will only have to quarantine after visiting the other 40 states on their travel advisory list. Congratulations for now to California, New Hampshire, Vermont, Massachusetts, Maine and Hawaii. In a few weeks that will probably be only California and Hawaii. I wonder if they’ll change the quarantine criteria when New York itself starts meeting them about two weeks from now?
In June, Trump put two political appointees into the CDC with no officially assigned roles, it seems with the express goal of preventing the flow information out of the agency. Which isn’t really news at this point, but figured I’d include it anyway.
Trump repeatedly says that 85% of people who wear masks catch Covid-19. How many people does he think wear masks?
Trump was not tested on debate day.
Who Deserves the Credit, And Who Deserves the Blame?
(Nikolai Ivanovich Lobachevsky is his name.)
We Canadians did everything right. Our spin studio followed all the rules! We masked before and after spin class. Everyone knows you can’t catch Covid-19 during a class where we’re all engaged in hard physical exertion. What you can do is catch Covid-19 during the next class from surfaces infected in the previous class, so we make sure to clean all those surfaces within 30 minutes. If we take longer than that, the pizza is free.
We Australians did everything right. Need to maintain the travel restrictions. If we make an exception to get newborns life saving surgery, where does it stop?
Spain was not doing everything right. Their expensive living conditions and small living spaces are to blame for their pandemic! America, with much bigger living spaces than any place in Europe, strangely never gets credit for that, nor does it seem to make much difference. Nor does cost of living seem to correlate with infection severity by city, although population and density do seem to matter where policy decisions mostly didn’t. And the wave hitting Europe now isn’t even concentrated in Spain.
We Americans are not doing everything right. Our schools in New York City began doing mandatory random testing. And that’s terrible, so the CDC decried it as ‘unethical and illegal.’ They also issued additional guidance:
Classrooms and schools “may” temporarily close if there is a coronavirus outbreak, and local health officials “may” test students, teachers and staff, the CDC said, stopping short of urging those actions.
We wouldn’t want to urge such actions, that would be going too far, but I guess we won’t actively stop you from stopping gatherings and doing tests when and where there is a Covid-19 outbreak. Thanks, CDC!
Flight Mask
Looks like it is safe to fly if masks are worn by all, based on this study out of Hong Kong. The numbers involved seem rather definitive. The method seems like a great natural experiment. Everyone is tested on arrival, then quarantined and tested again, so most infections should be caught, and the odds of that seems like they have a very small upper bound.
That is great news for obvious direct reasons. If one needs to fly, it seems reasonable to get on a plane if the rules are enforced.
But the really valuable thing is to take this information and see what other lessons we can draw from it. Masks being sufficient to drive the risk on an airplane down to very low levels seems like a key puzzle piece.
The obvious key question is how airflow works on a commercial flight. Whatever they are doing, it seems to be working. Then we can ask the classic question of flight safety, and see about the pandemic equivalent of making the whole plane out of the same material they put into the black box.
Boeing provides this guide, Airbus is similar:
Cabin air filtration
If the airflow is coming from the ceiling, where it’s gone through heavy filtration, then flows under you and back to the filters, then it makes sense that the risks would be much lower than you would naively expect. You’re effectively outdoors or kind of a super-outdoors. Combine that with silence and mask wearing, and you’ve got a place that’s potentially mostly safe even for several hours.
All Boeing airplanes have systems already in place
to help maintain a healthy cabin environment. These systems filter the air you
breathe and minimize the spread of airborne contaminants.
The volume of cabin air is exchanged every two to
three minutes
HEPA filters similar to those used in hospitals capture more than 99.9% of
viruses and bacteria
Cabin air flows primarily from ceiling to floor in a circular pattern and
leaves through the floor grilles near the same seat row where it enters
It also makes sense that planes would be much safer than they look, because they are! Everyone’s instinct is that flying in the air in a metal box is one of the crazier, scarier and riskier things one can do, whereas (in terms of accidents) actually you’re in far more total danger driving to the airport than you are on the flight, even on an absolute basis rather than per mile. Everything about planes is safer than it has any right to be, because we demand that planes be our safe place and are willing to pay insane amounts to make that happen and also actually make sure we get what we paid for.
There is always the risk of security theater (see the TSA) rather than actual security, but that’s because actually being safe in that case wasn’t enough, we needed to both actually be safe and then Sacrifice to the Gods on top of that to make people willing to fly.
So on reflection, if you told me that the time in the airport was ten times riskier than the flight itself in terms of infection, because they don’t have as good a handle on air flow, I’d pretty much believe you.
This is yet another path to victory. If we were to actually seriously model air flow, we could allow for people to be indoors together in relative safety, which would end this.
As far as I know, air flow in buildings isn’t regulated, so it’s something one could do research and innovation to improve without worrying about it being illegal. Time to get to work, everyone.