

Covid 10/8: October Surprise

Last week: Covid 10/1: The Long Haul
As part of 2020’s continuing attempt to top itself, President Trump has Covid-19.
It is unclear whether it is more surprising that Trump got Covid-19 now, or that it took this long for him to become infected. It has become very clear that this has been waiting to happen for some time.
The story of Trump getting Covid-19 can be divided into a few different branches.
There’s the story of the timeline. What happened to Trump when, and what did he and the people around him do in response? This is important for the security of our country and for the election, but not necessarily directly impactful for the expected future path of Covid-19.
There’s the story of Trump’s treatment. How sick was he when, with what symptoms, and what treatments did he get? Were those treatments right? How much do they improve his prognosis? Should others get those same treatments? What does it say about his expected future health? We can learn about what Trump can expect, which impacts what the country can expect, and we can learn about medical research and decision making, and what other patients should demand and can expect.
Then there’s the political messaging and impact surrounding all this, and its impact on Covid-19 going forward (as opposed to the impact on the election). This could go in any number of directions. Perhaps Trump getting a serious case of Covid-19 makes his supporters take things more seriously. Perhaps Trump’s messaging that Covid-19 is not serious and we need to learn to live with it makes his supporters irresponsible, and we see large outbreaks. Perhaps nothing matters much, and people do what they would have done anyway.
There’s also who got infected when and how, and what we can infer from this event about how Covid-19 spreads.
Meanwhile, other things didn’t stop happening. Almost none of the people who were infected this week were Donald Trump, and so far none of the people who died were him.
I do my best to avoid politics in these posts, and focus on the pandemic. This week made that extraordinarily difficult. Still, I did my best, and I expect those commenting to do the same.
Before we get to his saga in detail, let’s run the numbers.
Deaths
DateWESTMIDWESTSOUTHNORTHEASTJuly 30-Aug 518317194379365Aug 6-Aug 1217386634554453Aug 13-Aug 1915768504264422Aug 20-Aug 2615037453876375Aug 27-Sep 212457593631334Sep 3-Sep 911417712717329Sep 10-Sep 1611599543199373Sep 17-Sep 2310168932695399Sep 24-Sep 309349902619360Oct 1-Oct 779711032308400

The South and West continue to slowly improve. This week confirms that decisively in both cases, although of course it may not continue.
The Northeast’s problem is widespread but its biggest problem area is New York, which is now rapidly going from bright spot to potential very serious medium-term problem. Even more concerning is the Midwest.
What this definitely is not is anything that points to the popular media talking points that deaths are about to spike and we’re going to lose another 200,000 people by the end of the year.
Positive Test Counts
DateWESTMIDWESTSOUTHNORTHEASTAug 13-Aug 19808876338415699820857Aug 20-Aug 26675456654013232218707Aug 7-Sep 2550007540112741421056Sep 3-Sep 9472737243910640821926Sep 10-Sep 16450507526411581223755Sep 17-Sep 23540258538112773223342Sep 24-Sep 30554969293210630027214Oct 1-Oct 7567429724311017034042

Those are obviously not good numbers, but they are also not especially worse than last week except for the Northeast, and all region numbers except the South reflect increased test counts. Things here seem mostly stable in the other three regions, and they could end up going in either direction from here - even the Northeast positive test percentage barely budged.
Positive Test Percentages

PercentagesNortheastMidwestSouthWest8/6 to 8/132.30%5.67%14.67%6.98%8/13 to 8/202.06%5.62%9.41%6.47%8/20 to 8/261.86%5.78%9.93%5.88%8/27 to 9/21.87%6.37%9.38%4.78%9/3 to 9/91.97%6.02%8.48%4.13%9/10 to 9/162.41%5.99%11.35%4.49%9/17 to 9/232.20%5.96%7.13%4.11%9/24 to 9/302.60%6.17%6.18%4.27%10/1 to 10/72.61%6.05%6.74%4.23%
The South’s percentage here jumps back up. That could be a trend, but it’s likely mostly reversion after the big drop over the last two weeks. The other regions are static on positive test percentages, which are the best forward-looking metric. They do need to be adjusted for increased testing, so the trend is indeed negative, but it’s a small effect at this time.
Test Counts
DateUSA testsPositive %NY testsPositive %Cumulative PositivesAug 6-Aug 125,121,0117.3%506,5240.9%1.58%Aug 13-Aug 195,293,5366.2%548,4210.8%1.68%Aug 20-Aug 264,785,0566.0%553,3690.7%1.77%Aug 27-Sep 25,042,1135.5%611,7210.8%1.85%Sep 3-Sep 94,850,2535.3%552,6240.9%1.93%Sep 10-Sep 164,632,0055.8%559,4630.9%2.01%Sep 17-Sep 235,719,3275.2%610,8020.9%2.10%Sep 24-Sep 305,857,0975.1%618,3781.1%2.19%Oct 1-Oct 76,016,6335.2%763,9351.3%2.29%
New York is rapidly heading in the wrong direction. The rest of the country’s numbers aren’t changing much. If there’s a third wave heading our way, the numbers don’t show any evidence of that.
The biggest media sources continue to attempt to panic us by pointing out raw positive test counts. This is absurd. We have had most of a year to get this straight. Maybe when winter comes people will stay indoors too much with others and things will get very bad. Maybe people will all stay home more and things will actually get better. Trump’s antics could help, or hurt. And so on.
We don’t know what’s coming. And yes, some areas, in this case New York and the Midwest, are trending in the wrong direction at this time. But to warn of an inevitable additional 200,000 deaths within the year, like it’s part of the timeline and only masks can save the future, is deeply dishonest and irresponsible at this time.
The Presidential Timeline
A lot of things happened. This is my current understanding of the timeline. If my understanding improves within a day or two, I will edit this. After that, I won’t, and I’ll update everyone next week as needed.
Some Time Before All This
The head of White House Security, Crede Bailey, becomes ill with Covid-19. He remains in the hospital on October 7. Possible original source of outbreak.
Friday, September 25
Trump attends fundraiser with Ronna McDaniel, who later will test positive.
Saturday, September 26
Donald Trump hosts a deeply irresponsible Rose Garden ceremony at the White House in celebration of his Supreme Court nominee, Amy Barrett. This includes an outdoor ceremony with lots of prominent Republicans packed in tightly, including the President’s family and inner circle. Photos are from link above.


There was also an indoor ceremony, largely without masks.

(Source)
Later, after Trump’s diagnosis, this would be one of the ‘White House photos of the week’ (source):

Since both events had many of the same people and took place on the same day, it’s difficult to say where infection took place without careful contact tracing, which the White House is not doing. Both events were deeply irresponsible. They involved old and vulnerable people, didn’t wear masks, and had extended close contacts. We even have video of outright hugs. These are not people who are taking the virus seriously on a personal level.
Here’s a chart looking at the seating versus who would later test positive:
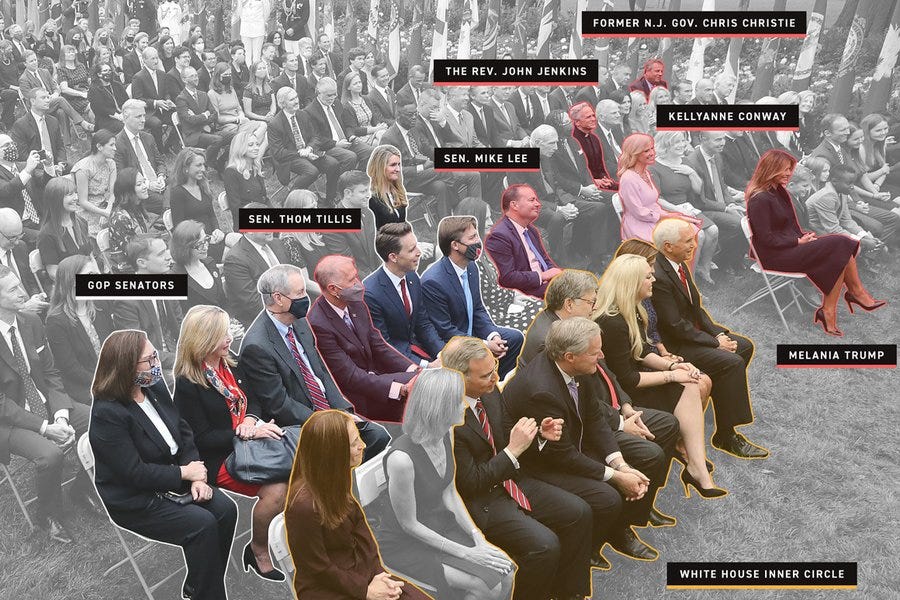
(source)
Tuesday, September 29
Trump and Biden hold the first Presidential Debate. Trump shows up sufficiently late that his on-site Covid-19 test cannot be conducted, and it is skipped. During the debate, among other things, Trump mocks Biden for wearing masks. Trump and Biden’s podiums were 12 feet, 8 inches apart. Members of Trump’s party did not observe mask protocols, even when offered masks by the staff. The bulk of Trump’s Debate Prep team will later test positive.
Thursday, October 1
In the morning, Hope Hicks, who has been travelling extensively with the President, tests positive for Covid-19. Only a small group are told at first.
The President does not quarantine, nor do others who have been exposed to Hicks.
President proceeds to travel to an indoor unmasked fundraising event in New Jersey, without getting a test.
The President, at some point (I’m not clear on exactly when in this order) tells his chief of staff to not reveal their positive test result.
After the fundraiser, the President gets a positive result from a rapid test.
The President calls into Hannity, and does not mention his positive result.
The President gets a second positive result.
Late that night, the President announces he and Melania Trump have tested positive and will quarantine at the White House.
Friday, October 2
The president’s condition worsens.
The president is taken to Walter Reed hospital via helicopter.
The president’s oxygen level drops into the mid-high 80s, and he is given supplemental oxygen. He is given oxygen a total of twice that we know about.
(His doctor said, in response to whether it dropped below 90, that it did not drop into the low 80s, so we can assume it did drop into the 80s but probably not the low 80s.)
The president is given an experimental antibody cocktail widely expected to be safe and effective, but which has not been approved for general use.
The president is also given Vitamin D, Zinc, Melatonin and remdesivir. He is not given HCQ.
The president’s doctor lies about his condition, which he will later claim is to keep the patient’s spirits up.
Everyone says the next few days will be crucial.
Kellyanne Conway tests positive for Covid-19. Others will continue to test positive and I won’t note most of them, but there are a bunch of such people and the list keeps growing.
Biden tests negative, and will continue to test negative. He sends Trump his thoughts and prayers. He resumes campaigning, but pulls negative ads and turns his Twitter feed into generic bland statements even more than before.
Saturday, October 3
Information about the President’s condition continues to be unreliable at best. Doctors assure he is getting better, for whatever that is worth, throughout the day.
The President’s doctor refers to “72 hours into treatment,” which if accurate (this timeline assumes it is not accurate) would place his first positive test on Wednesday rather than Thursday, and placed Trump’s first treatment of antibodies on Thursday morning. Presumably this wasn’t accurate, but I have no idea why he said it.
President releases ‘proof of health/life’ style pictures and videos to reassure public, including signing a blank sheet of paper. A video is later shown to be edited to remove a cough.
President claims to be engaged in ‘document review’ and be eager to return to White House.
President’s lack of Twitter activity worries many (no really).
President is given steroid treatment dexamethasone typically believed to only be appropriate in critical and severe Covid-19 cases. In less severe cases, it is on net thought to make things worse. These steroids have side effects that can be severe, including mood swings.
Senator Ron Johnson tests positive for Covid-19 after attending dinner while awaiting his test results, says he ‘did not anticipate testing positive.’
Sunday, October 4
Trump’s doctors continue to claim Trump is rapidly improving and say he could be released as early as tomorrow.
Outside medical experts do not think claims by Trump’s doctors are credible, nor do they think releasing Trump within the next day would be advisable, although they note that White House has a complete medical facility.
Just before market futures open for trading at 6pm, Trump does a drive around in his motorcade to wave to supporters. The motorcade is sealed against chemical attack and effectively a giant hot box, inside which were multiple secret service agents which now must quarantine away from their families for two weeks.
Monday, October 5
Trump has a morning string of all-caps Twitter posts that mention various issues and then end in “VOTE!” This marks the end of his long Twitter absence.
Trump leaves the hospital just after 6:30pm, or 72 hours after admission.
Upon arrival at White House, Trump climbs balcony stairs, removes mask, waves at crowd before proceeding inside.
Tuesday, October 6
Among many other Twitter posts, Trump says this, which is false and going to get people killed, and hopefully massive backfire politically: Flu season is coming up! Many people every year, sometimes over 100,000, and despite the Vaccine, die from the Flu. Are we going to close down our Country? No, we have learned to live with it, just like we are learning to live with Covid, in most populations far less lethal!!!
Trump reaffirms his intention to do a Town Hall Debate on the 15th, somehow.
Multiple members of the military who work around Trump have now tested positive.
Washington, DC reports 105 cases, the most in one day since June.
12:30pm: Trump’s doctor reports Trump has no symptoms and his Oxygen saturation is 95-97%
1:00pm: Top military brass forced to quarantine after exposure.
4:00pm: 123 front-line workers in the Capital complex have now tested positive. Contact tracing continues not to be done. Few without positive tests are in quarantine.
We learn 13 employees at Murray’s Restaurant in Minneapolis quarantined for two weeks because they catered a party attended by the president on 9/30, which is on timeline because of how many others aren’t in quarantine.
After mocking Harris and her team for demanding it and attempting to refuse the request multiple times, Pence and his team agreed to a plexiglass barrier in the next day’s debate. Pence has been in close proximity to many people who have tested positive, but has himself always tested negative.
Wednesday, October 7
Trump’s manager announces his intention to resume working out of the Oval Office, allow staff to come into contact with him because there will be ‘precautions in place that allow for that.’ Hours later, Trump is in the Oval Office ‘being briefed.’
Trump’s doctor says he is symptom free and his blood shows substantial levels of antibodies.
Trump (presumably still on steroids) Tweets that Biden should not be allowed to run and accuses him of treason. In all caps, of course. He’s totally fine. People barely noticed or cared.
Regeneron notes that the antibodies in Trump’s test were likely the ones from the antibody treatment.
Trump camp claims those around Trump are tested daily, but admits that Trump himself was not tested daily.
Pence and Harris debate in Salt Lake City, separated by twelve feet and two very small plexiglass barriers. It is painful to watch and nothing is said. Pence is set upon by a fly, and had a curiously red eye. Perhaps he’ll die. Hopefully and presumably not, though. Pence’s wife does not wear a mask on stage, in violation of debate rules.
Thursday, October 8
Commission on Presidential Debates announces the second debate will remain a town hall debate, but that it will be virtual, with both candidates dialing in and the ‘undecided voters’ themselves in Miami.
In response to this announcement, Trump says he will not participate: “I am not going to waste my time on a virtual debate.”
It is noted that during Trump’s previous visit to the hospital, doctors (who are bound by confidentiality anyway) were required to sign NDAs. We still don’t know why he was there.
In his first phone interview since being infected, Trump blames the ACB announcement event for the outbreak. "Somebody got in and people got infected."
He also says “I think I’m better. I’d love to do a rally, I don’t think I’m contagious at all.”
We continue to not get any answers regarding the date of Trump’s last negative test.
It is Dave Barry’s son’s birthday, and hence the date on which all historical events occur. Happy Birthday, Rob!
Zen and the Art of Glomarization
Trump’s doctor is in a tricky spot. As is his press secretary.
You don’t want to lie. Lying is bad. It’s against your ethics to lie. Plus, if you are caught outright lying, as he was, it ruins what little credibility is left and throws everything into doubt. Thus, you want to strive to avoid outright lying. I do think that the doctors are doing their best not to outright lie too often, as most doctors do.
Or, of course, maybe that’s what they want you to think. They can’t tell the whole truth, because then they’d have to tell the whole truth. They can’t tell only true things, because Trump wouldn’t stand for it, and also there’s no politically good way to tell only true things. There’s even a real security need to make it look like everything is under control, and Trump is not about to hand power over to Pence, because his systems say you never do that.
So what would Trump’s doctor do if he had no choice but to lie? He’d retreat to the next level of plausible deniability. As many times as necessary. First he’d try for the impression he wasn’t lying. When that failed, he’d give the impression he mostly wasn’t lying. When that failed, he’d give the impression he at least cared about lying and wanted to do less of it rather than more. That’s a much better position than people thinking you always lie, all the time, about everything. And it’s true that he gets some reward for maintaining these levels for longer, so that provides some reason to believe there is some real correlation between the truth and what the doctor is saying. There isn’t no reason to believe anything he says. There merely... isn’t a very strong reason.
Trump himself is not in this particular tricky spot, because he’s crossed fully into lying all the time. But there is great value in preserving at least some credible alternative means of communications.
Hence the glomarization problem. Or rather, the problems that result from a complete lack of Glomarization. Without that option, the failure to answer a question says a lot.
Thus, I am able to put “Trump’s oxygen level in the mid-high 80s” on the timeline above.
Trump’s doctor was asked whether Trump’s oxygen level had fallen below 90. In response, he said it had not fallen into the low 80s. Once it’s clear that he’s willing to discuss oxygen levels at all, it seems obvious that he’s giving the most information his patient has allowed him to share. His patient’s goal is to look strong, so he will share any information that Trump believes makes Trump look strong, and not share any information Trump thinks makes Trump look weak.
Thus, I conclude that every good news statement is, at best, the strongest technically true statement of that same type. Trump’s levels were just barely above the ‘low 80s.’
The same goes for every action Trump takes. If something would make Trump think that he’s made himself look healthy, he’d do it. If not, he won’t. So this was the strongest signal he and his team had the ability to send, including both the President’s health and the skills required for execution.
If Trump hasn’t called into any shows, it means he’s not confident he can do so without coughing. If he could, he’d do it.
If Trump doesn’t Tweet, it’s because for whatever reason he can’t. Thus, he couldn’t for a while, then he could. Once he could, he did.
If Trump doesn’t put out videos or photos, that means that the best photos or videos would have been worse than nothing, which is very bad news indeed - and thus, makes that news even worse. That’s why you almost always expect to see some photos and videos, no matter how bad it is getting.
As of when I’m writing this, Trump looks to be recovering and stable, and able to sit around watching news and sending angry Tweets, which is much of what he did to campaign in 2016. So that’s what he’s doing. Trump will, by this logic, feel he is under extreme pressure to resume meetings and rallies - because if he doesn’t, in his mind that means to others that he can’t. Never mind that he’s infectious.
The biggest unknown is: When was the President’s last negative test?
And here, we are faced with the Unexpected Hanging Paradox.
Assuming Trump’s claims are accurate and his doctor misspoke to put his first positive test on Wednesday, Trump’s first positive test was Thursday, taken in response to the positive test from Hope Hicks. There was a highly unacceptable delay between those two events, and Trump should have quarantined even with a negative result, but let’s ignore that for now.
If Trump’s last negative test was on Thursday morning prior to (or simultaneous with, which would make some logistical sense in terms of a testing system) Hicks testing positive, then great. That’s the best possible answer. But obviously they would have told us that if it was true, so it isn’t true. It’s safe to assume there was no negative test on Thursday.
But now that we all know there wasn’t a negative test on Thursday, the best case scenario for Trump is that he tested negative on Wednesday. Thus, if he did do so, he would be well served to say so. And he hasn’t done so for several days. So it seems highly improbable Trump tested negative on Wednesday.
That also potentially helps explain his doctor’s statement. If Trump’s doctor was thinking that he hadn’t had a test at all on Wednesday, he might be treating Trump as if he was probably positive then because of a Baysian prior that follows from how bad things got how fast. Actually makes sense. So it seems very likely Trump wasn’t tested Wednesday. Unless he tested positive and is hiding that fact, which of course explains the doctor’s statement even better. We certainly can’t rule that out.
Which in turn means two things.
First, either Trump tested positive on Wednesday, which would be really super duper bad for him if it got out and got verified since he went to events after that and didn’t tell anyone for days including Biden, or Trump being tested daily is a lie.
Second, Trump did not have a negative test after the debate with Biden.
Everyone who says “Trump catching Covid-19 means testing is not the answer” should note that not only did Trump totally disregard all the rules regarding behavior, with everyone around him failing to distance and few of them wearing masks, he also didn’t get daily tests. You can’t despair over the value of testing if it wasn’t tried.
That moves the question to Tuesday. If his last negative test was on Tuesday, would he reveal that?
That’s less clear.
What saves Trump from the full Unexpected Hanging Paradox is that there is an extra advantage to not answering. If you don’t answer, no one can know for sure, no one can use as ‘fact’, the answer. Sure, they can be rather confident what the answer is, but that’s not the same thing.
Thus, even if the test was on Tuesday, and we know it almost certainly couldn’t have been later than that via the logic above, it still might not make sense to reveal that information, even though it is the best possible scenario. If you don’t say anything, then no one can say “Aha! You admit that you weren’t doing the daily testing you said you were!” They can claim it anyway, of course, but there’s nothing like a confession. And Trump world is not typically inclined to admit any kind of mistake or wrong-doing, for exactly this reason.
Thus, I don’t think we know whether the test was on Tuesday, or if it was earlier. It might even be much earlier.
Perhaps Trump wasn’t being tested much at all, on theory that if he’s never tested, he’s never positive, and catching Covid-19 makes him look weak. Whereas if he never gets tested, often he won’t have symptoms or won’t have symptoms he can’t hide. That would certainly explain why he showed up to the debate late enough to skip the Covid-19 test, and it fits his personality and other actions.
Alternatively, maybe he’s doing every two days, or when they feel like it, or something, but it’s still not something they’d admit.
I do think the refusal to say is some evidence in favor of the date being earlier than Tuesday, but I think it’s weak evidence. Whatever your prior was before, that should mostly still be your prior, because he usually wouldn’t say anything either way.
A similar phenomenon explains refusal to contact trace.
If you contact trace, you find out who spread the virus to who, and what actions they took doing so. Right now, we know people in Trump’s circle did wildly irresponsible things and some of those things probably turned into at least one super-spreading event. But we don’t know who exactly was responsible, and we don’t know what the event was.
Any event and person we could concretely identify would be far more blameworthy. Thus, it’s better to not know the details. Even if the details are 90th percentile not-so-bad, that’s still worse than not knowing, in terms of blame allocation. There are even different factions looking to blame one for different actions.
In such a world, one must value their privacy even when one has done far less wrong than average. One who does things at all is inevitably vulnerable to blackmail or retaliation if one learns about those actions in sufficient detail. When one has done more than average, and is actually the worst, one must be that much more paranoid. Luckily for such awful people, the paranoia of others helps protect you somewhat, justifying your refusal to reveal or learn information. It’s a war against not only common knowledge, but all knowledge.
Quarantine For Thee But Not For Me
When is it necessary to quarantine for two weeks?
The guidelines say one should do this whenever one is in close contact with someone who tests positive, even if you yourself continue to test negative.
The definition of ‘close contact’ has always been somewhat nonsensical and elusive, but the principle is clear. If you are exposed, it doesn’t matter what the tests say. Quarantine time.
Thus, when secret service agents take a ride with Trump, time to quarantine. Period.
We talk about social distancing and mask wearing as our primary weapons against the virus. The actual primary weapon has always been quarantine of sick and potentially sick individuals, but it’s so basic we don’t even mention it.
Regular people understand this.
Our top politicians? Not so much.
Trump is obviously the most egregious example. When Hope Hicks tested positive, he was a close contact. He not only did not isolate, he did not even get test results before going to fundraising events without masks. Then, after saying he would quarantine and having to go to the hospital, the first thing he did after leaving the hospital (in what would, if he were not the president, have at least been Against Medical Advice) was take off his mask several feet away from some White House workers so he could wave to the crowd. Republican talking points deny those workers exist, but there are photographs. And it sounds like (hard to tell for sure) Steven Miller spent hours with Trump at the hospital, and now Miller has tested positive.
So that’s pretty terrible.
Mike Pence has many close contacts who have been positive. He should be quarantining many times over. He is not doing that, instead fighting efforts to protect those around him, while continuing to go out there putting others at risk. The CDC cleared him to participate in the debate, but this is clearly in direct violation of their guidelines.
Those guidelines continue to use the ‘within 6 feet for 15 minutes’ rule, which again is such obvious nonsense, which would be fine if it was an upper bound that people took seriously but not literally. Instead, everyone at the top levels, it seems, is taking it literally as a technical hurdle to be fulfilled.
Three senators tested positive, and many have been exposed. How many are exposed we don’t know, because contact tracing hasn’t been done. But it’s clear that all of them plan on going about their business as normal the moment they have a negative test, and many aren’t even waiting for that, because ‘they don’t expect to test negative.’
Nor are any top level Republicans, it seems, wearing masks, or practicing social distancing while indoors.
Then there’s Joe Biden.
Yes, technically Joe Biden is not a ‘close contact’ of Donald Trump. They were 12 feet apart rather than 6 feet.
Indoors. For 90 minutes. Unmasked. With Trump yelling much of this time directly at Biden.
If you have any sense of the physical world, that’s obviously riskier than 15 minutes spent 6 feet away from someone you aren’t actively talking to. It’s much, much riskier.
That doesn’t mean Biden is a favorite to catch the virus in that spot, nor it seems did he catch it.
But it does mean that it was his duty to quarantine, just as basically every Republican politician on the hill should have quarantined. He did have the decency to get regular tests and disclose them, and to wait for the first result. That was good, I guess?
But like them, he didn’t quarantine. That’s not acceptable.
I don’t get why he didn’t. It would be easy to blame it on Trump, who personally exposed him, and then literally sit back at home and watch the dumpster fires burn. The events Biden is going to aren’t that impactful, and risk some sort of gaff or distraction. So it’s all confusing to me. Are the people involved even on the “responsible” side so blinded by basic heuristics that they have lost all ability to model the physical world? Are they so tone-deaf and selfish that they don’t think they need to follow the rules or set a good example?
Signs point to yes.
Plexiglass
Here’s a picture of the vice presidential debate stage:
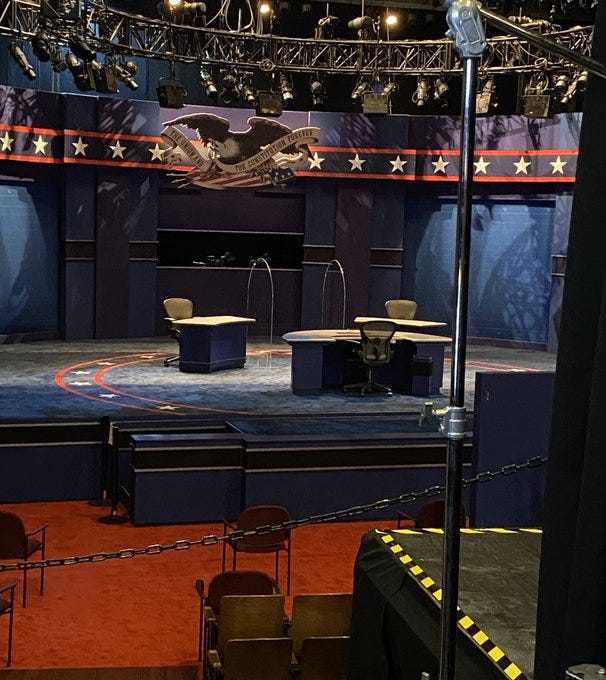
How much will those barriers help?
I think they help a substantial amount, even if they’re pathetically small. There are two barriers between the candidates, so unless air flow gets very strange almost nothing will get directly from one to the other. It also is nice that they’ll be farther apart than Trump and Biden were. Alas, the candidates remain indoors, and also the moderator isn’t protected in either direction, which seems foolish.
And most of all, these barriers are far smaller than I’d like. Grocery store clerks have much, much bigger and more extensive barriers, as they should. Why are we taking any chances on this one?
The general consensus among ‘experts’ seems to be that the barriers won’t do anything because the candidates are twelve feet apart already, so large droplets were already not a problem. This is another example of obvious nonsense. The ‘experts’ are taking ‘more than six feet’ to mean ‘not close’ and reasoning from a simplification heuristic designed to help give people a rule of thumb. Thus, obviously droplets can’t travel twelve feet! That would imply six feet wasn’t safe. As opposed to thinking about the physical world, and realizing that twelve feet is a lot better than six, but a lot worse than twenty-four.
Also, if we have this kind of clear consensus that full airborne transmission is the main worry here, why did the CDC only admit that this week? Still, kudos that they finally did it. See the relevant section below.
In general, I’m a big fan of the large plexiglass barriers in grocery stores and other such places. When I went to the store yesterday there were large ones everywhere across the large counter, and it seemed great. We need more and bigger such barriers.
Where Do We Go From Here?
All of that matters. What happens to regular people, and the overall course of the virus, matters far more. If we focus on what matters, as we would be wise to do, we care about what happens to Trump primarily insofar as it impacts the world and our lives.
There are reasons for both optimism and pessimism as the result of the outbreak at the White House.
The optimistic case would point out that this makes Covid-19 impossible to deny or ignore. The President had it, and had to be hospitalized. We can all agree it is real and dangerous. The optimistic case would follow that up by pointing out that it’s easy to point to the precautions not taken by Trump and those around him, the masks not warn, the tests not taken, the distance not maintained - it helps show people that it is up to them to stay safe and keep others safe. And it puts the spotlight on that, and on the cost of failure to do so in terms of risk and of disruption.
The optimistic case would end by saying that now that Trump has been infected, he has an incentive to play up the threat, because that makes him look stronger for having beaten it, and more worthy of our sympathy and support. That would be the smart play.
The pessimistic case would say, that’s all very nice, but this is Donald Trump and those who follow him we’re talking about. Look at how they have chosen to play it. It doesn’t look good.
Those backing Trump now say, if even Trump got the virus, despite all his precautions (none of which he actually took, but never mind that), what hope do the rest of us have? Why bother taking precautions?
Those backing Trump now say, if even someone as old and obese as Trump can lick the virus this easily (never mind all the treatments he got, or that he’s not out of the woods even for the short term and his doctors are lying, or that most patients don’t die) then what are you afraid of? If you’re afraid of Covid-19, it means you’re weak! It means you’re a coward! I’m sure that’s going over great with everyone who lost a relative or dear friend. Which is a lot of people.
Trump says, don’t be afraid of Covid-19. Don’t let it dominate your life. Where ‘dominate your life’ means some combination of ‘infect you and maybe you die’ and ‘cause you to wear a forking mask and forking social distance like a decent human being.’ Trump doesn’t even think that currently being infected should stop him from acting like the virus doesn’t exist, in terms of risking the health of others. Which makes sense. What does he care if others get infected, now that he can’t get infected again? “Maybe I’m immune,” he muses.
Trump-beats-Covid $100 'commemorative coins’ on sale. Memes from congressmen of Trump beating the virus in a wrestling match. Trump with actual nothing left to lose. This will not end well.
At this point, it’s too early to tell, but so far the pessimistic case seems more correct.
How would we know if this is what is happening? This would be a partisan response, and a partisan outcome. Thus, if we see things start getting relatively worse in red states rather than blue states, versus previous trends, especially a sharp turn around a week or two from now, then that’s a sign that this made things substantially worse. The opposite would mean it made things better.
We Could End This With Rapid Tests But We Won’t Because “Medical Ethics”
On a call this week with my father, who used to teach immunology at Columbia University, he asked what he might be able to do to help. My answer was that the most important lever available was rapid tests. Get more approval and more support for more rapid tests, more at home tests, and we can end this thing. Soon.
I’ve been over this ground but a Marginal Revolution link put it unexpectedly cleanly: Benjamin Mazer on Twitter: "I want to talk a bit about medical ethics and widespread asymptomatic antigen screening for COVID. I think it'll help to break down some terminological and philosophical distinctions that are easy to become confused about. Bear with me."
There’s a big ethical dilemma, he notes. On the one hand, we could do the “utilitarian” thing where we run some tests, stop the virus and no one gets sick and dies. Or, on the other hand, this would require people to do things that aren’t in their individual selfish interest, and that’s not ethical. It might give people information they would use to make decisions that wouldn’t be completely clear-cut, and they might even choose wrong, or demand medical care from a doctor after getting an unreliable positive test, and allowing that is definitely not ethical. Even worse, all this would lower the status of doctors and make them feel uncomfortable.
Let’s make this simple. If you think that there’s a safe way for people to voluntarily take actions that results in us defeating Covid-19, at very little expense, and you ban it or advise us not to do it because “ethics,” you are not ethically or morally better than the President. You have no ethics.
That’s in addition to any questions about getting people a vaccine, or getting people better treatments, or gathering better information, or all the other things we know we could do. That we choose not to do. A continuing series, see next section.
(And of course, F.D.A. Delenda Est.)
We Could Give Better Medical Care and Learn More About What Works, But We Won’t Because “Medical Ethics.”
When you actually care more than anything about the prognosis of your patient, and you have the ability to disregard the usual restrictions, the choices you make reveal a lot about what you actually think works to treat patients and make them recover rather than die. There are no frequentists in foxholes.
Everyone agrees that Trump’s medical team and hospital are first rate. There’s worries about ‘VIP treatment’ where he gets too much care, and there’s worries that they’re lying their asses off to the American people because they’ve been caught doing that, and of course Trump is likely a terrible patient in both directions, demanding some VIP treatments while also refusing things like staying in the hospital a reasonable amount of time. But everyone agrees, in terms of capability, great medical care, first rate stuff.
So if they are giving Trump experimental monoclonal antibodies, Tyler Cowen asks the obvious question. Are they positive expected value, or negative expected value? Do they make you more likely to live, or not? If so, and it seems like most informed people think this, why aren’t we using them? If not, why aren’t those who don’t think this saying that?
My father the immunologist thinks they are absolutely the best treatment and that if he was in Trump’s position, he would want exactly this treatment regimen. Except like Tyler, he couldn’t get that regimen.
From what I see, it seems highly likely this treatment is worthwhile and should be used when available. Here’s one article summarizing. The data isn’t fully in, but we are Bayesians, in a foxhole, and this is an open and shut case.
There is some good news on this front, as some UK hospitals have reached the same conclusion.
Our problem is people and posts like this. She explains the reasons why giving a likely effective treatment to a sick patient is just awful. You see, if the trial results aren’t in we can’t ‘know’ anything, and also... things might happen. Which would be bad because it would harm the clinical trial, which is the One True Way in which people can know things. Which things would harm the trial? All the things! Let’s go through it.
If it looks like the drug works and is good, that will make it harder to do clinical trials, because who would want to risk being given a placebo!
If it looks like the drug doesn’t work and is bad, that will make it harder to do clinical trials, because the drug looks bad!
Why would anyone join a clinical trial if they might randomly be put in the less good group rather than the more good group?
Thus, we need to keep all information out of everyone’s hands, and their confidence at exactly current levels, so that we can get participants.
This is, of course, obvious nonsense.
If the drug looks good, it’s still expensive and not widely available, so signing up for a 50% chance at it is much better than not signing up for a 0% chance. You’d get lots of volunteers.
Even if the drug doesn’t work, increasing publicity around the drug, and thus the number of patients who know about it to seek it out, plus the fact that the doctors liked it enough to try it on Trump, will also drive many people to the trials. You don’t need that big a percentage of Covid-19 cases, so even if the headline news looks superficially bad, so what?
So I actually think this will only be good for participation. The only reason it could be bad is that we have a systematic campaign against doing things. If you have full Asymmetric Justice, then you are blameworthy for everyone who now doesn’t sign up, and everyone will panic about every potential marginal bad outcome at every level. Whereas everything you improve doesn’t count. Under this same model, doing a clinical trial counts as Doing a Thing, so it’s already highly suspicious. Any objection to it means it’s bad, since you can’t count good things against the bad things. So if you do something blameworthy in its general vague vicinity, that’s really bad for its chances.
(And of course, if you actually want to run these super valuable studies and enroll patients, have we tried... giving people money or other considerations in exchange? No? Doesn’t seem like we care very much about doing this, then.)
When someone says things like ‘you have to think like an epidemiologist’ I wonder what that means. Does it mean ‘you have to think about the bigger picture and overall path of disease’? That’s something I can get behind. Does it mean ‘you have to adopt the rules and “ethics” and status systems and consensus behind the group that calls themselves epidemiologists and are considered Very Serious People’? Then that’s how you end up taking nonsense SEIR models seriously.
Aerosol Transmission Update
Remember a few weeks ago when the CDC accidentally told the truth and had to walk it back?
Good news, everyone. They’ve unwalked it back. CDC revises coronavirus guidance to acknowledge that it spreads through airborne transmission.
So here’s to you, CDC. You’ve acknowledged the utterly obvious. For that, we salute you. Because as I’ve said, here we believe in incentives, and we believe in redemption.
Don’t get me wrong, CDC. You’re still very much in the Delenda Est Club. You worked so hard for your membership, I wouldn’t take it away from you so easily. But you get points this round, and there’s lots more points out there for you to score. It’s never too late.
Here’s an FAQ on Avoiding Aerosol Transmission. I’m still reading through it, and I’m not endorsing everything it says, but it seems at least interesting and thoughtful. It makes the case (which I don’t buy myself) that aerosol is the primary mode of transmission.
In Other News
Former CDC Director sends current director five pages of scathing fire. It’s worth a read.
There was an open letter from some Belgian doctors running around that advocated for lifting all restrictions. Alas, it’s standard anti-lockdown paranoia talking points, including doubting the effectiveness of masks while touting the known effectiveness of HCQ, and so on. This prevents its good points in other areas from getting a hearing that might matter.
Marginal Revolution points us to a new working paper on mask effectiveness in Canada. Headline number is a 25% reduction in new cases over the first few weeks as a result of indoor mask mandates. Given the impact of control systems and also that of compound improvement over time, plus people’s increased voluntary mask-wearing as they learn more, I don’t know how one properly extrapolates that, as they do, to a number of cases per week now. It does seem very clear such mandates are worthwhile, which is the question that matters.
There’s a new antibody test that’s claiming to be cheap, doable at point of care, 90% sensitive and 99% specific. So presumably it will be illegal indefinitely.
New paper confirms challenge trials are highly effective at saving lives of humans. Their analysis suggests a challenge trial would save an expected 8,000 lives. So presumably it will be illegal indefinitely.
The latest attempt to model herd immunity uses only spacial heterogeneity and ignores other differences between people, and still gets the number down from the base assumption of 77% down to 47% from that alone. They then suggest that other differences could drive it down as low as 34%, but with no confidence these other things matter. As usual, once I look at the nuts and bolts, this seems hopelessly conservative.
New York Stories
New York is in some trouble. There are a number of ‘hot spot’ neighborhoods and towns with startlingly positive test rates, including one Orthodox Jewish town worryingly near my current location, Kiryas Joel, that has hit 27%.
First, Cuomo and De Blasio decided to move from state average positive rate to the state positive rate without the hot spots to explain how well things were still going. Then, once it was time to pivot to how bad things were going so they could step in and impose restrictions, they pointed out how much of a crisis it was that the hot spots were so bad. Schools have been closed there. De Blasio tried to close non-essential businesses, but Cuomo wouldn’t let him.
Cuomo managed to use a photo from a previous decade as one of his examples of irresponsible and illegal gatherings in Kiryas Joel, which was most certainly not a good look, but didn’t actually change anything.
There’s no question that some religious communities have decided to live their lives as if there was no virus and not care about the consequences. And in general, that people’s precautions are slowly weakening and things are getting slowly worse across the state.
As they often do, the Very Serious People sound alarm bells and say things like “New York City on the edge of a precipice.” Such statements are meant to give an impression that there is some sort of threshold effect and sudden doom coming, to spur people to Do Something and Be Afraid. It doesn’t actually mean anything.
Looking at such charts, what strikes me is how contained the real problem is within a few areas. The chart goes down to a 3% positive rate, which is much worse than the city’s or state’s rate, but better than the national average. There is interaction between areas, but likely not that much interaction between the highly infected areas and the areas where people have made the commitment to take precautions. Even within a zip code, different parts of the city can be remarkably distinct.
On Wednesday the hot spots looked like this (via Cuomo’s twitter):

That’s quite the broad definition of “hot spot” to extend down to 2.3% positive rates.
It also tells us good news by its absence. There is no zip code in Manhattan, the Bronx, or anywhere in the state outside NYC and two zip codes in Orange Country, where the positive seven day average is over 2.3%.
Nor does that left column look at first glance much worse than the right column - and that turns out to be right. The 7-day average here is 5.8%, whereas yesterday in those same zip codes the average is 5.3%. There’s a selection bias here of course, but that hardly seems like a situation spiraling quickly out of control.
That doesn’t mean things will end well. If the election ended tomorrow, I wouldn’t feel comfortable moving back to the city under current trends. Slowly getting worse still gets quite bad. But I don’t see any sudden cataclysm in our future. Chances are, it will mostly stay contained in the areas that are unable to be or choosing not to be safe.
But what of herd immunity? I’ve been saying for a long time that the herd immunity thresholds are much lower than one would naively expect. You shouldn’t need anything like 60-75% of people to be immune in order to get things under control. So what to make of the areas having resurgences mostly having high amounts of previous infection?

What it looks like is that there is no obvious correlation between antibody test rate and current case load.
That is an argument strongly in favor of the impact of immunity.
Without immunity, you’d expect places that previously had large infections to continue to have large infections. Previously getting infected is strong evidence that those areas were more vulnerable, took fewer precautions, had higher starting reproduction rates (R0). They also used to be infected, and that can persist directly. So for all of that to mostly cancel out means that herd immunity here is about enough, on average, to level that playing field.
The places that have the big outbreaks are clearly those that are doing almost zero social distancing. Religious communities with big families that think weddings and prayer services are more important than some virus. They’re young, their lifestyles aren’t compatible with social isolation and were in fact chosen largely for social cohesion, and this is all part of them executing a strategy that is high in reproductive fitness.
The resulting reproduction numbers before immunity are going to be through the roof. They won’t be slightly higher. This isn’t a 2 vs. 3 vs. 4 thing. We’re talking about people who regularly attend potential super-spreader events that are more risky individually than the sum of everything you (yes, you) have done since March. So for those areas to get herd immunity, we might be talking 80%, 90% or higher rates of immunity necessary for true herd immunity. If anything, what’s odd is that they didn’t get more infections earlier - presumably they did honor the restrictions somewhat for a while.
Back in normal places, it’s going to be far lower. In many places, one can think of the necessary local threshold as negative percent immune, because other countermeasures are more than sufficient to halt spread. They would have beaten this thing by now in Manhattan, or at least many parts of it, if the rest of the city and world didn’t constantly reintroduce the infection.
The scary counterargument is that cases overall across the state are suddenly on a rapid upswing we don’t see in other areas - other areas that weren’t hit as hard early. A logical hypothesis for why this is happening would be that immunity is fading in New York, where many got infected in March, and immunity then only reliably lasts about six months. If anything, the effect is too big for this, because everything is spaced out in time, all effects will be continuous, and things are decaying at an accelerating pace that such theories can’t really explain.
My actual best non-trivial hypothesis is not one I especially like, and it’s that in addition to partial reopenings of some schools, New York has many who just celebrated the High Holidays, and many of them didn’t care at all about social distancing during those ceremonies. Whole communities spending that time indoors, packed in close proximity, and deciding they’d had enough. It matches where many of the biggest outbreaks are, and would explain a sudden rather than gradual rise. Cuomo clearly seems to believe something similar. But there are also a bunch of zip codes where this explanation doesn’t apply, and the resurgence is there throughout much of the Northeast, so this is at best a partial explanation.
The good news is that to the extent that this is the cause, it’s not something that repeats that often, and its effect could be largely contained to the communities in question.
What to make of the interventions?
The crackdown is going... about the way you’d expect.
As usual, assuming you can actually enforce your changes, it comes down to the same question. Do we actually want to win, or are we going to go for herd immunity in the end regardless? That is, in these areas, rather than overall.
If it’s that second one, then we have plenty of hospital capacity, our treatments have improved, and these areas are self-contained enough. We should let them ride things out now, while everyone else is in decent shape, and put ourselves in a better spot going forward.
If it’s that first one, sure, shut down the schools, but you’d better have a reason why you aren’t on this plan until a vaccine arrives. Cause you won’t be able to do that, and you’ll be causing a lot of pain for not much gain, against most of these people’s both stated and actual preferences.
Thus, I don’t think it makes sense to shut down the schools in these spots. I think that’s exactly a way to let the spread continue but stay within the hot zone. Nor should non-essential business close, which would force inhabitants out into other areas to infect the rest of the city. If anything we should do the opposite, and encourage those within such regions to stay in them. I would be tempted, if it were possible which it isn’t, to raise capacity back to 100% to ensure that. It’s not like those in other areas would want to venture in.
Either way, we’ll be here in Warwick for a while, it looks like. Especially considering the conclusions about impact from Trump’s illness.