

Covid 12/3: Land of Confusion

Last week I warned that we would have unusually high uncertainty for a while thanks to the Thanksgiving holiday. This was both due to unknown events and difficulties in measurement. Reporting and testing would both be delayed by the holiday, and the holiday’s real effect would be difficult to predict.
A week later, we have some information, which confirms that the holiday threw a larger monkey wrench into the reporting and testing systems than I predicted. This makes it that much more difficult to tell what has been happening in terms of infections or deaths. Looking at each day individually becomes necessary to have the best available sense of the overall puzzle, despite the dangers of doing that.
The last two days strongly suggest that Thanksgiving did make things considerably worse. People gathered unsafely, and that bill must now be paid continuously until the pandemic is dealt with. By next week, or even by tomorrow night, we will be able to answer that with more confidence.
That’s the bad news. The good news is that the United Kingdom has already approved the Pfizer vaccine, and it looks likely we will follow their lead a week from today. If logistics hold we can begin vaccinations the next day, and get everyone who wants it vaccinated by June at the latest. It won’t take that many vaccinations for the tide to turn, as it is likely not that far from turning even without them, and may (or may not) have already turned in the Midwest.
The song remains the same. Infection risk is as high as it has ever been, and is rapidly going to peak as the vaccine arrives and lots of people are immune via infections. If there wasn’t an additional set of holidays coming, I’d expect the peak in true infections to be this coming week in many places and within another week of that for the country overall.
Since there are multiple major holidays coming, I instead expect the final peak is most likely to happen in the wake of Christmas and New Year’s Eve. That is a very nasty one-two punch - people gather on Christmas, get infected, gather again right when they get most infectious from Christmas on New Year’s Eve with different groups spending hours drinking together indoors. Quite the final boss for 2020.
Let’s run the numbers.
The Numbers
Last week I predicted a 12.8% positive rate on 11 million tests. Instead we got exactly that 12.8% positive rate but on only 8.8 million tests, as the slowdown was large. Last week was even more of a spike in demand than I realized. Deaths reported did not jump up to the 2,100 I predicted, instead staying roughly static at 1,616. I figured they’d catch up on reporting by Wednesday, and I was completely wrong about that. Whoops. Bad prediction.
For next week, there is again a lot of uncertainty, because we don’t know where we are now. My unconfident prediction is a 14.8% positive rate on 10 million tests, and an average of 2,200 deaths to account for at least some amount of catching up in reporting. But, again, wider than usual error bars all around.
Deaths

DateWESTMIDWESTSOUTHNORTHEASTOct 1-Oct 779711032308400Oct 8-Oct 1478212172366436Oct 15-Oct 2180415912370523Oct 22-Oct 2889517012208612Oct 29-Nov 495619772309613Nov 5-Nov 11108927122535870Nov 12-Nov 181255293428181127Nov 19-Nov 251761416933961714Nov 26-Dec 21628381427421939
That’s not what happened last week. That’s what was reported to have happened last week. There is approximately zero chance that deaths truly declined. They lag by several weeks, so I would disbelieve this decline even if we did not have the Thanksgiving holiday to explain it.
What surprised me is that we have no sign that reporting ‘caught up’ for what happened over the weekend. The last two days are up from the same days a week ago, but only by roughly the corresponding past increase in cases. The missing deaths, for now, are still missing. I overestimated our ability to report, or underestimated how long it would take to clear the backlog, or both.

This chart looks at 7-day rolling averages of deaths, compared to cases 2 or 3 weeks beforehand. The drop at Thanksgiving is clear, after this mostly held steady for three months prior (the CFR here was higher earlier, but I cut the graph off to make it readable).
Positive Tests

DateWESTMIDWESTSOUTHNORTHEASTOct 1-Oct 7567429724311017034042Oct 8-Oct 146828412574411799538918Oct 15-Oct 217557114985113323843325Oct 22-Oct 289498318188115812357420Oct 29-Nov 411268425291716709870166Nov 5-Nov 11157495387071206380108581Nov 12-Nov 18211222452265255637150724Nov 19-Nov 25269230435688294230170595Nov 26-Dec 2256629357102294734185087
The decline in deaths is failure to count the deaths. The decline in positive tests is a failure to run the tests at all. All discussions are on hold until we see percentages and test counts in the next two sections.
Test Counts
DateUSA testsPositive %NY testsPositive %Cumulative PositivesSep 24-Sep 305,833,7575.1%618,3781.1%2.18%Oct 1-Oct 76,009,8455.2%763,9351.3%2.28%Oct 8-Oct 146,322,8655.7%850,2231.1%2.39%Oct 15-Oct 216,439,7816.5%865,8901.2%2.52%Oct 22-Oct 286,933,1567.5%890,1851.4%2.67%Oct 29-Nov 47,245,6008.6%973,7771.6%2.86%Nov 5-Nov 118,285,49510.6%1,059,5592.4%3.13%Nov 12-Nov 188,917,43312.4%1,155,6702.9%3.47%Nov 19-Nov 2510,429,84611.6%1,373,7512.9%3.83%Nov 26-Dec 28,813,39512.8%1,287,0104.0%4.18%
There were still a decent number of tests, but well behind last week’s count. Last week’s tests clearly included a bunch of pre-holiday demand, which was then followed by a holiday slowdown, so some time shifting on both ends. This makes it clear that things overall are not better than two weeks ago, but from this chart the two could plausibly be similar with shifts in different regions.
Then we look at the test percentages.
Positive Test Percentages

PercentagesNortheastMidwestSouthWest10/1 to 10/72.61%6.05%6.74%4.23%10/8 to 10/142.57%8.14%7.09%4.75%10/15 to 10/222.95%8.70%7.85%5.36%10/22 to 10/283.68%9.87%8.58%6.46%10/29 to 11/44.28%12.79%8.86%7.04%11/5 to 11/115.56%17.51%9.89%8.31%11/12 to 11/186.99%18.90%11.64%10.66%11/19 to 11/257.00%16.62%10.41%11.75%11/26 to 12/28.38%17.90%12.45%12.79%
We do still see the Midwest test percentage lower than two weeks ago, but only by about a percent, while everyone else is clearly headed back in the wrong direction. It’s clear that the Midwest is trending relatively well, which makes sense given how bad things have been for a while now.
How Bad Was Thanksgiving?
The problem is this chart, which in context is very bad news:
DatePositive Test %Rolling 7-Day Avg12/2/202015.6%12.8%12/1/202016.6%12.6%11/30/202010.8%11.8%11/29/202013.3%11.7%11/28/202010.8%11.4%11/27/202011.4%11.5%11/26/202012.9%11.6%
The last two days are, by a substantial margin, the worst in many months.
I usually avoid day-to-day numbers, but here we see exactly what we feared. Five days after Thanksgiving, the positive test rate soared, and it stayed there the next day. We will soon find out what kind of spike this is, but even if it is a one-time effect from the holiday, there is no reason not to expect that higher rate to be sustained as the newly infected infect others. With people coming home with new infections, we may even get a secondary additional spike, although I’d expect that effect to be small.
The default assumption is that it takes about five days for infections to begin showing up as positive tests. With the slowdown in tests over the weekend there is likely an even bigger backlog than usual, so a lot of results will be lagged further because of that. If people were largely infected on Thursday and some on Wednesday, we expect to see the surge of new cases begin in earnest on Tuesday the 1st.
Thus, the giant jump in positive rate on Tuesday, from a 7-day rolling average of 11.8% all the way up to 16.6%, followed by 15.6% on Wednesday, is such a super scary result. There’s a good chance Thanksgiving increased case counts by something in the range of 30%.
Sometimes looking at a metric tells you about the world. Sometimes looking at a metric, then looking at the world, tells you some things about the world, but tells you more about the metric. Nate Silver points out that Google is showing only a moderate Thanksgiving increase in ‘home visits.’ You see, the mobility score didn’t increase, so nothing to worry about? To me, this highlights that mobility scores and frequency of visits to various location types are data points that can be useful, but that fail to capture the thing about Thanksgiving that we are worried about.
I don’t care about the frequency of travel to any household. I care about large gatherings, especially large intergenerational gatherings that are not typical sets of people, and thus would not have already infected each other. I care if those gatherings involve long periods of time, and activities like extended feasts full of conversation, that are all but designed to encourage virus spread. I care about people travelling long distances and thus shuffling around exposures, and encountering people at airports and otherwise along the way. The numbers cited here tell us nothing about those concerns.
We still have little idea how much impact Thanksgiving had. A few more days from now, we’ll have a better idea. When we get far enough out to find the death curve, that will be even more informative. But the data is a mess and unless we see a huge spike or crater we will never be able to reliably measure the magnitude of the effects. Reluctance to get tested in these situations only makes all of these measurement problems worse. So does the ambiguity in the pre-existing trends, and the impact of pre-Thanksgiving behavioral adjustments. It’s possible that people were safer before Thanksgiving and directly after, and that might mitigate the effect, perhaps even fully. It’s possible that only measurements were distorted. I have a very non-confident Bayesian prior on all this.
How Many Undiagnosed Cases?
This has always been one of the most important known unknowns. The more infections, the less dangerous the disease and the more people are already immune without knowing.
I’ve been working on the assumption that we are detecting one in five or six infections, with room for that to be anywhere from one in three to one in ten. Yesterday I learned (in what will be old news to some of you) that the CDC has issued guidance that says it estimates this at one in twelve, with a range of 7 to 25? The document seems to use August data and was written in September, so more than a bit out of date, but it’s still quite the claim.
We can now rule out the extreme high end because we have 4.18% of the population having a diagnosed case. A 24:1 ratio (1 in 25) would imply everyone had been infected, and we would have seen dramatic effects from herd immunity long before that. Even with an 11:1 ratio, that puts us at ~50% infected, chosen non-randomly. If that doesn’t get us to full herd immunity, it gets us within striking distance.
The report is also guessing R0 at 2.5. That seems impossible as well, at this point. It has to start out higher than that, or things would be solved or at least unambiguously improving by now. Using their high end estimate of R0=4, which is what I’ve been doing for a while, seems close to a lower bound.
Meanwhile Covid-19 projections still estimates a 3.3 ratio.
The CDC range seems clearly too high, and it’s a sign of how I value such inputs that my prior is updating very little on the new information. One in five or six still seems most likely.
Partial herd immunity effects are rapidly becoming more impactful even without the vaccine. As I said above, I expect the final peak to happen at the latest in the wake of Christmas and New Year’s Eve. , which could be a very nasty one-two punch - people gather on Christmas, get infected, gather again on New Year’s Eve with different groups. That’s quite the final boss for 2020.
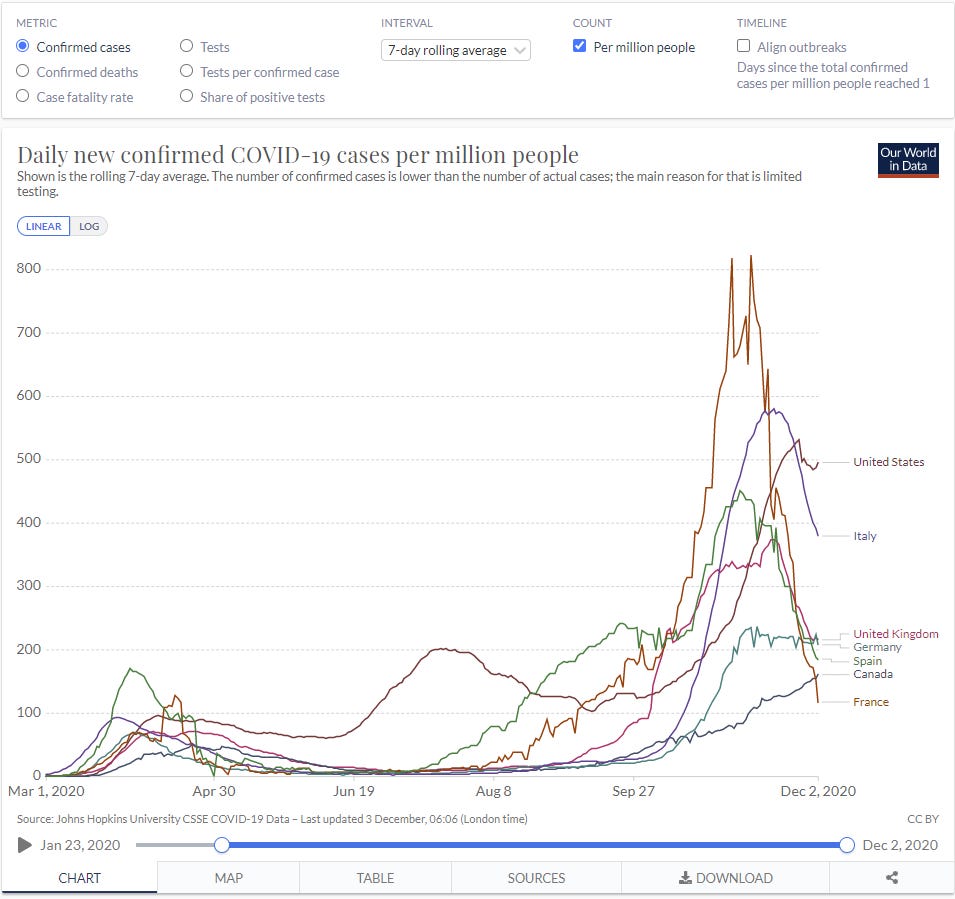
Europe
Confirmed Cases:
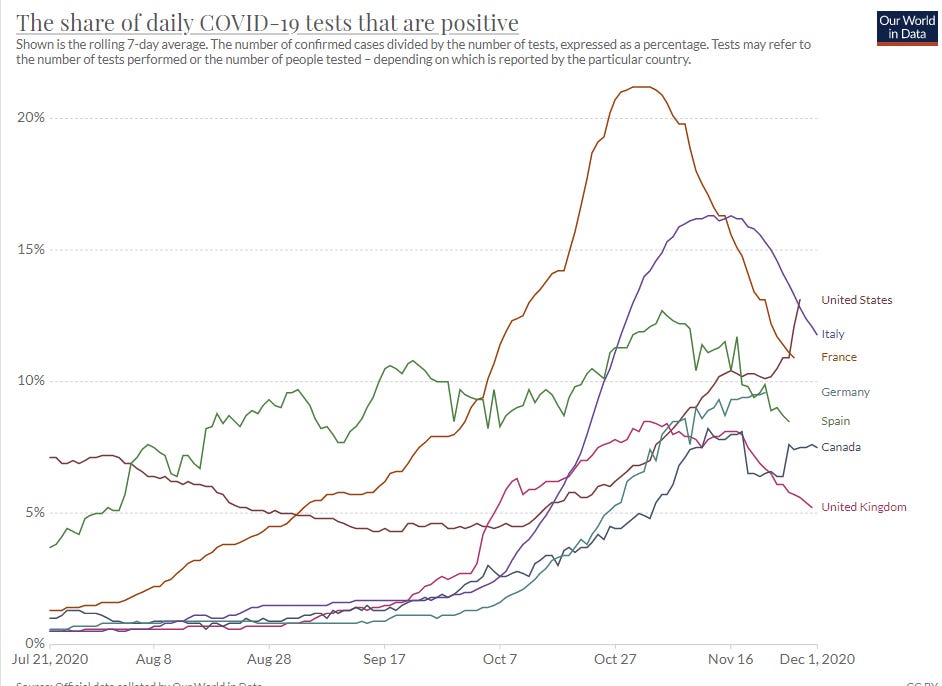
Share of positive tests (starting late July to make this readable)
And deaths:
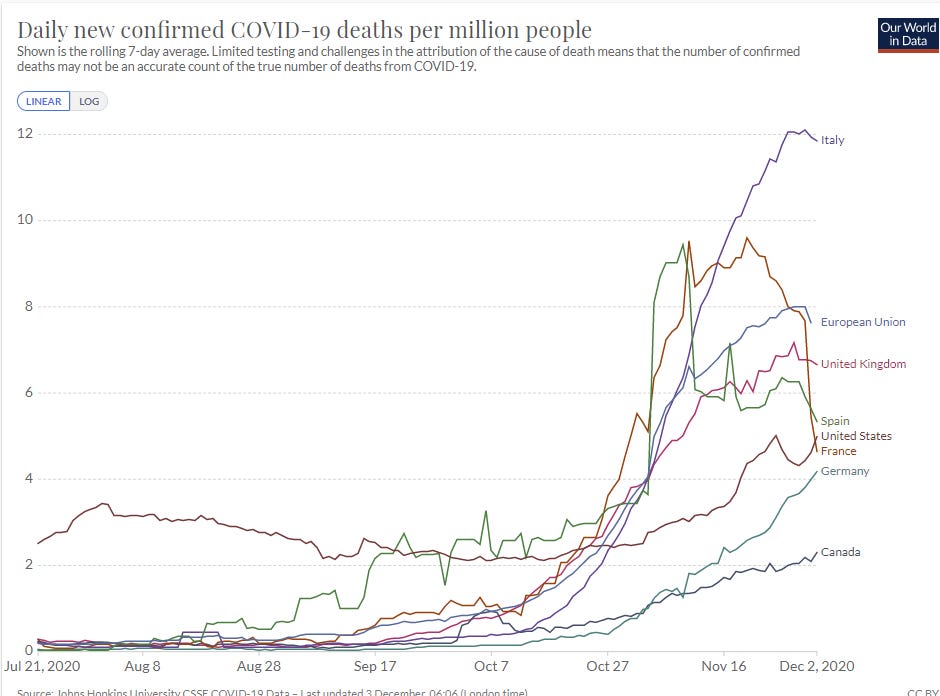
Deaths haven’t had enough time to start dropping in earnest yet except perhaps in France (something strange is likely going on with France’s deaths data here) but the case trends are clear. The European countries that decided to get things under control are rapidly getting things under control. The countries that decided to level things off instead, did that instead. The United States did not do such things, but will soon enough get a similar outcome from a higher level.
All I Want For Christmas Are A Covid Vaccine and a PS5, But They Underpriced Them, And Now They’re All Sold Out
The stage is set. The applications are in. The United Airlines charter planes full of dry ice are standing by. All that remains is for regulatory authorities to give emergency approval and allow distribution.
What does it take to get a Covid-19 vaccine approved these days?
The United States says, at a minimum, it takes the regularly scheduled meeting on December 10. There are upsetting rustlings that this actually means sometime after December 10, but anticipation still seems to mostly be that distribution can probably begin December 11, about three weeks after the Emergency Use Application was sent in, a period during which tens of thousands will have died of Covid-19 in the United States.
The United Kingdom is having none of this nonsense. They approved the Pfizer vaccine on Wednesday, and will be distributing it next week.
The European Medicines Agency, the presumably unionized European equivalent, thinks the F.D.A. is acting with unnecessary haste. The best case scenario is the end of the year:
“Assuming everything is positive - and we have to look at the data to be sure - but best case, we could have a scientific opinion by the end of the year,” EMA Executive Director Emer Cooke told the Irish Independent newspaper in an interview.
“These have been developed very quickly, which is very promising from a scientific perspective, but it means there is a lot of attention on the results and we have to make sure we evaluate those as efficiently as we can without compromising our usual scientific standards.”
Another update here via MR suggests evaluation will be done by January 12.
The implicit statement here is that things are moving fast and they are against things moving fast because fast is symbolic of irresponsible and slowing things down makes you a Very Serious Person, so they are going to slow things down to fix that. The explicit statement is merely that they need time to fully examine the data, which implies logically that either they are much slower than the F.D.A. or United Kingdom at doing that and don’t trust those sources, or that those places are not fully examining the data.
The Japanese are going to take even longer. You see, vaccines normally take longer to develop, and we did this one fast, and that’s highly suspicious. Extreme caution is needed. You’d better do trials specifically in Japan if you want to convince the Japanese. Despite that, they’ve decided to buy 120 million doses by mid-2021, so presumably they have a plan to run those tests by then. And given they don’t have a pandemic problem right now and are used to wearing masks anyway, letting other countries take the vaccine first makes good sense. So it kinda makes sense even if the justifications are terrible.
The good news, of course, is that there are a limited number of doses, and as I discuss later geographically concentrating vaccinations is a good idea, so all we have to do is have someone approve the vaccine. Then they can use all the early doses until others also approve.
For America and especially Europe, the timeline comes back to the question of what ‘fully examine the data’ means. What are these people looking for that takes a month to analyze after the data comes in?
If Pfizer came out a week ago and said, ‘in secret we have developed this vaccine for the past eight months, and we present to you a new miracle of modern medicine, BEHOLD!’ I would totally understand it taking a month to examine the data. That’s not how this works. That’s not how any of this works. They’ve been in constant communication with regulatory agencies, their study designs were already approved, and the data from the trials boils down to essentially two things: Who got infected with Covid-19 with what severity, and what adverse side effects were observed.
The news on efficacy is well in excess of expert expectations, essentially a best case scenario. So if plans were approved in the first place, it takes almost no time to say ‘yep, looks like the efficacy data is very good.’ Certainly this isn’t what is taking weeks.
That means that if we are examining the data we are looking at safety data for adverse effects. But once again, there were not any major adverse effects. There is a nasty short-term effect when you get the vaccine, but they know that already and have had months to evaluate that. So yes, you have to look carefully to confirm the whole ‘yep, looks like safety data is very good’ angle, but how long does looking carefully take when there’s nothing to see?
Also worth noting is that Moderna’s application came in several weeks after Pfizer’s, its data was available several weeks after Pfizer’s, and it looks like both will be considered simultaneously. It’s hard to then argue that Pfizer’s application couldn’t have been handled any faster. It looks more like the FDA at best did not want to hold multiple meetings. The counterargument to that is that the two vaccines are very similar, and thus the work can be combined, but that has its own implications.
I do realize that three weeks turnaround is, all things considered, extraordinarily good, even a month is good, but that’s a condemnation of standard procedure, not an excuse.
The missing mood is an emergency. The missing action is planning ahead and making conditional decisions in advance the way I would when playing a game with a time limit. You don’t know what is going to happen next, but there are only so many options, so you consider each of them and plan a response. You have a procedure that lets everyone involved stay on a reasonable schedule and maintain sanity and all that, and keeps an orderly priority queue and avoids favoritism and all the politicization and corruption that usually leads to. Under normal conditions great and all, considering the practical alternatives, but maybe there are times to throw all that out the window?
I’m furious at this last small delay because it is so obviously unnecessary and shows how bad things are even when there is unusually strong pushing for fast progress. I don’t actually care about the delay itself all that much, however, because the limiting factor in distribution is manufacturing capacity. The same number of people will be vaccinated in February regardless of any delays in December, provided they don’t extend beyond a few weeks. More people will get sick and die, and more people’s lives and days will be lost or ruined, but compared to the overall stakes this is very small potatoes. Compared, that is, to previous delays.
Did you hear how Moderna made their vaccine in two days without even having a virus sample? So we could have very easily been done months ago if we allowed challenge trials, or even without that if we were allowed to do expected value calculations and run larger experiments faster?
Did you hear how the limiting factor was safety data, but we still were unable to scale Phase II trials enough that their safety data could count as safety data, forcing us to wait out for Phase III safety data?
Did you hear the one about Moderna having a big lead on Pfizer, and being told they had to delay their trials because they had insufficient minority participation (rather than start while working to expand such participation, which is what you would do if you actually cared about helping people, and while Pfizer was not told told to do any of this) leading to Pfizer finishing first?
Meanwhile, a take on why many of the vaccine trials likely underestimate how effective they are, and which seems right to me.
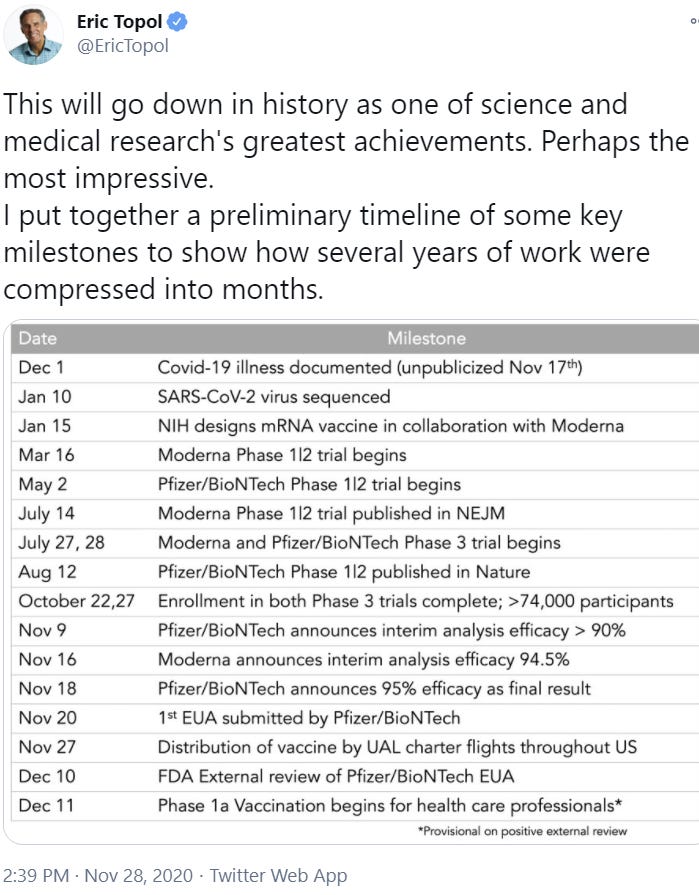
Also in medical research world modeling, here’s some of how mRNA vaccines came to be a thing.
Who Gets the Vaccine First?
We can’t vaccinate until we use politics to decide who gets priority. The CDC is meeting to determine that. To avoid figuring out which areas have greater need, and to avoid any possible accusations of blame via buck passing, but also because apparently Trump and his team can’t be bothered with such trivial questions as logistics, allocation is first going to go to the states by population, but without telling states in advance how much vaccine they will be getting or providing them with funding to distribute the vaccine, and the states are then going to be tasked with deciding on distribution.
(I’m sympathetic to ‘states must maintain balanced budgets that do not make sense during a pandemic, and the federal government should be aiding states a lot in general’ but I am completely unsympathetic to ‘they aren’t providing money specifically for distribution’ because money is fungible.)
Health care workers and the most vulnerable continue to be presumed to be going first in most or all areas, in some combination.
Both of these make good sense. Health care workers expose themselves as part of their job and are out there directly helping. The most vulnerable are much more likely to die if infected.
Putting both of these in the “1a” group to get the vaccine first is going to be tricky. This was the question that needed to be decided, to figure out which of those two groups goes before the other, and as far as I can tell everyone everywhere has passed the buck. There are only enough doses initially for about three million people, by the end of the year perhaps twenty million. There are about twenty million health care workers and about 1.4 million people in nursing homes. So now in each state, we can expect lots of small political battles to determine how much allocation goes to various hospitals and nursing homes, then within each institution to determine who gets vaccinated early versus later. Those with power, status and connections within those institutions will be rewarded.
That population of 1.4 million in nursing homes is, according to the CDC at the source above, responsible for 6% of infections and 39% of deaths. If I were making the decision, I would go there first. If these first 4 million doses can cut deaths by 39% that seems like the best option.
On a side note, obviously going to a nursing home is caused directly by old age and failing health so the statistics are completely unfair, but has anyone considered that these places might be eldritch abominations?
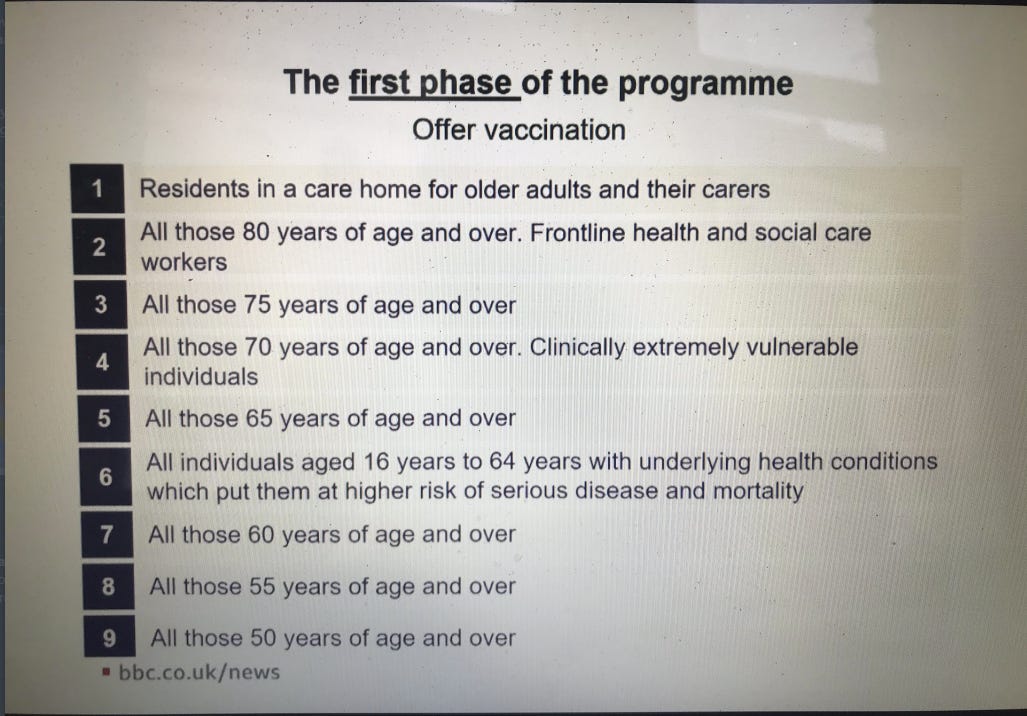
Here is what the United Kingdom will be doing, which seems reasonable enough although it excludes a lot of essential workers for longer than I’d have thought wise (source):
It has been pointed out that distributing the vaccine evenly among all locations is actually the worst possible choice. Vaccination has network effects. If you vaccinate enough people in one location, then everyone there can go back to normal. The vaccinated hospital or nursing home can then operate much better, or even an entire region.
If you vaccinate only some people in every location, no one who isn’t vaccinated can go back to normal at all, and even those who get the vaccine can’t fully go back to normal. There’s no normal around them to return to, and while the pandemic rages on, 95% effective is not 100% effective. This is fractally true as well: If I get vaccinated but my wife does not or vice versa, that has its advantages, but mostly far less than half the advantage of vaccinating both of us. Thus, proceeding in a random order by location would be better than an equal distribution, assuming the right sub-categories still got appropriate prioritization. That argument makes me think there might be an allocation even better than allocation by price. The downside is that any prioritization process like this is vulnerable to politics and corruption, which equal distribution prevents.
I find the questions both interesting and relevant, since we all need to know when to expect our chance to be vaccinated and know when we could plausibly claim priority. Can my parents, definitely at high risk due to age and comorbidities, get protected early? Can my wife, who is a psychiatrist, do so, and if so what about me? Are any of those claims justified? I do not know.
Then of course, there’s the question of the already infected and therefore already immune. In a remotely sane world, when Covid-19 tests are scarce, the first thing you do is give people antibody tests to confirm they need the vaccine, or at a minimum you could... ask people who have already had the Covid-19 not to get vaccinated? Even if insisting on this is not possible, of course, I would implore anyone who is immune to not try and get vaccinated until there is adequate supply. I don’t even know why they would want to.
Another question is, are they going to effectively force those who get an allocation to take the vaccine instead of giving those doses to people who actively want them? I am content to wait until after essential workers and the most vulnerable, so long as I get it before all the people who don’t actively want the vaccine.
A warp speed official claims that ‘100% of Americans that want the vaccine will have had the vaccine by June’ and that seems mostly fine. I’m going to make a push to get it in March or April instead, and I expect to succeed because a lot of people won’t care much and I’ll care a lot.
Meanwhile, there continue to be worries abound about how to convince many people to take the vaccine, especially once they realize the shots often have unpleasant temporary side-effects. Worries about whether people will get a bill for vaccination even if the vaccine itself is free. If you were wondering how the medical system works, the ads I saw at that link were for personal loans, and it looks like yes you will get a bill and then file a bunch of forms to hopefully avoid paying it, because that’s what ‘free’ means.
Convincing the reluctant is something we will have to deal with some time around May or June, and certainly plenty of people will try to free ride, but I am confident our existing systems will mostly pull through here. By then, I’d also expect most people who refuse vaccination to have already been infected anyway, given correlations in behavior.
Sports Go Sports
When the pandemic arrived, sports shut down. We didn’t know how dangerous it would be to play, or how to play relatively safely. Since then, sports have mostly resumed.
The NBA bubble went off without a hitch and showed us better ways to test and keep us safe, which the outside world seems to have mostly ignored. They are moving forward with next season: "The NBA announces, among many key dates, that the Hall of Fame inductions for the Class of 2020 — headlined by Kobe Bryant, Tim Duncan and Kevin Garnett — will take place in mid-May."
MLB had some trouble, especially in the contract negotiations, and had a bunch of infections, some of which the players blatantly ignored, but was able to reschedule the games that it missed as necessary, and we got the boys of summer. The MLB bubble seems to have broken on the final day of the World Series, but in the end it all worked out. I do not think anyone caught Covid-19 from an opponent at a baseball game, but within-team activity was clearly not safe. The danger was in the dugouts.
The NFL skipped the preseason to ‘keep players safe’ and it seems like not having preseason led to a lot more non-Covid injuries than normal. Also contributing is likely that practices are happening less often and less intensely and efficiently due to precautions. It’s very possible that the ‘let everyone get Covid’ plan would have been safer, as I’d much rather get Covid than face the health risks of playing professional football. Still, it was clear they were determined to play.
The show must go on. No football, no peace.
That’s not to say there haven’t been hiccups. As infections have risen elsewhere, more and more teams and players are coming down with the virus. In previous weeks, teams cancelled games when they had a lot of infections. For whatever reason, Denver was told this weekend that the show had to go on, despite all four of its quarterbacks being ruled out due to contact tracing from their primary quarterback. No masks had been worn.
If you think that represents gross incompetence and they should have held their backup backup backup quarterback in reserve like a designated survivor if they had no fifth option, you’d be right, but they did not think about that at the time. They had the foresight to sign four quarterbacks, where usually there are at most three and the Giants only have two, then made it so a single positive test could take out all four.
The Broncos had to scramble. They tried to sign one of their assistant coaches, two of whom had played quarterback in high school and would know the playbook, but were turned down by the league, presumably due to worries that teams would try to use that loophole in the future to hide reserve players.
As a result, without enough time for an outsider to learn the playbook, Denver had to start Kendall Hinton, someone with zero snaps of practice that was signed to the practice squad a month ago as a wide receiver, and was previously selling sports equipment. Who hadn’t been tackled in years. As their quarterback. While the scoreboard was a disappointment and on reflection laying fifteen on the Saints may have been the wager of the year, there was nothing but praise for Kendall, who was put into an impossible situation. It is important to reward those who give extraordinary efforts and show their character even when the scoreboard would indicate otherwise.
San Francisco has decided to indeed allow no football, banning all contact sports without making an exception for the 49ers. They are not allowed to practice within Santa Clara county limits, and are scrambling for a new place to practice and play. Did I mention that the mayor of San Francisco, who has kept the city in a vice grip all year but who to be fair did not directly shut down the 49ers, London Breed, dined at the French Laundry with seven others the day after the governor did the same?
Meanwhile in college football, it is not going better. With the delays early on from when teams had yet to be shamed into playing the season, Big 10 and Pac 12 teams are losing huge portions of what’s left of their seasons. My team Wisconsin has two resounding wins, one embarrassing loss and three cancelled games, which means they are ineligible for the Big 10 championship game. Two of the top four teams had their coaches test positive this past week. For two straight weeks, more than ten games have been cancelled or postponed due to the virus.
Ohio State has missed multiple games and is in grave danger of missing the playoff due to lack of enough games, and ESPN commentator Kirk Herbstreit was forced to apologize for speculating that archrival Michigan might ‘wave the white flag’ and cancel their game to avoid their inevitable curb stomping (it’s gonna be ugly, folks) and also deny their rival the right to play in the Big 10 championship and probably the playoff. He says he ‘wasn’t playing fair’ but while I love the guy he’s a proud partisan of The Ohio State University so I don’t really know what anyone was expecting, and also I would never condone cancelling a game for such reasons and the honorable Michigan Wolverines would never ever do that, but I really hope this scenario actually happens.
Vanderbilt lost all its kickers and was forced to fall back on open tryouts. This resulted in Sarah Fuller, the goalkeeper of the woman’s soccer team, getting the job. Complete with ‘play like a girl’ inscribed on her helmet, she became the first woman to play in a power five football game, offering up a squib kick that was likely the best thing that happened on the field to Vanderbilt that day, as they lost 41-0 to drop to an 0-8 record.
College basketball got underway this past week. Already a large portion of the marquee games seem to have been moved, cancelled or created to fill newly available holes in teams’ schedules. There were some calls to move the schedule back a few months, but things are moving forward instead. Given how long the season is, it seems fine to cancel games as needed.
The reigning Formula 1 World Champion just tested positive. When a large percentage of all people get a virus, a lot of people in sports will also get that virus.
To my knowledge, there have been many cases across all these sports, but no cases of long Covid, and no deaths. That doesn’t mean there have not been such cases of long Covid, but the common presumption is that those infected will return in a few weeks. So far, in every prominent case or at least every case I am aware of, that has happened.
It has all made life much more bearable under this pandemic, for me and for millions of others. So I left you out of my thank you section last week, but here’s to you, athletes. Here’s to you.
Once More, With Feeling (You Should Know This Already)
Testing works. If you test often enough, as some colleges are doing, you solve the pandemic. We do not currently have the capacity to do this, because regulators have actively prevented us from creating that capacity instead of helping us build that capacity.
If you don’t have tests, you could even periodically screen for loss of smell and pick up 70%-80% of cases that way at a cost of something like a dollar per test. That could end the pandemic on its own, isn’t being done, and this is in the ‘you should know this already’ section. I presume this is a legal thing to do, though, so perhaps some people will read this and do it.
Links only say the same thing, but periodic reminder: Human challenge trials would have saved hundreds of thousands of lives. The failure to use them is a sign of our deep civilizational failures. It is not, however, one of the worst events of human history, because that list includes things like The Great Leap Forward, The Holocaust and the third Star Wars trilogy.
A reminder that we could do what we did for the coronavirus vaccine to do other things too.
In this section because congress is known to be essentially incapable of anything potentially useful: A raging pandemic and a gridlocked Congress could upend President-elect Joe Biden's plan to hire 100,000 public health workers to trace Covid-19's spread, despite widespread agreement it's needed to finally end the crisis. I’m not sure what good contact tracers are at this point, but they will presumably become useful later to wrap things up and keep them that way.
Updates From Events of Last Week
Marginal Revolution on the SCOTUS decision to prevent disproportionally closing houses of worship. Also a reminder from Rabbi Yosef Goldman that “In Jewish law, religious freedom in a global pandemic is the freedom from any other relevant obligation if a life would be risked in its fulfillment. In fact, protecting the lives of the living becomes the obligation.” I can verify that Jewish teaching is that you have a religious obligation to suspend your religious obligations if necessary to keep people safe, so services should indeed have been cancelled voluntarily. Where I disagree with Rabbi Goldman is that I believe that this doesn’t mean that cancelling them by force of arms fails to violate religious freedom. That’s not how freedom works.
Pilot shortage prompts rare flight cancellations at Delta over Thanksgiving break. Delta then transferred the passengers to other flights. Which is good news in the sense that everyone made their flights especially their return flights, and good news in the sense that the planes were previously sufficiently empty that there was plenty of space. It was bad news in the sense that everyone still travelled, and that they now did so in more crowded planes. In a normal Thanksgiving, there are lots of completely full or overbooked flights, and there’s a mad scramble to get everyone home and back again. All hands are on deck. It makes sense that in the new world, Delta would be willing to allow flights to instead be cancelled rather than pay a large premium to prevent this, even if it makes the flights less safe - they are hurting financially, getting extra workers over the holiday can’t be cheap, and they can transfer to their spare capacity if needed. That doesn’t mean that, as someone who by default uses Delta to fly, I will forget that they allowed this when deciding in the future.
McConnell finally puts an end to GOP meetings behind closed doors for lunch three days a week since May, maskless when speaking and eating, and some are more diligent than others in putting masks back on.
Introducing the scented candle complaint index of Covid cases. Seems like good news!
In Other News
Covid: Free Vitamin D pills for 2.5 million vulnerable in England. Excellent move, we should do the same everywhere else and also for the non-vulnerable as well. They almost got it! The way they almost got it was to claim it was about lockdowns preventing people from going outside, and Vitamin D deficiency being bad for non-Covid reasons. They’re not wrong, of course. Vitamin D deficiency is quite bad even in the absence of Covid-19, so this is an overdetermined cheaper-than-free action, especially given England pays for everyone’s health care. Still, even now, they’re saying that “But there is limited evidence that vitamin D protects against or treats Covid-19, although health officials have been asked to go back over the existing research” and also only recommending 400 IU/day, an order of magnitude less than I take.
Still, I’ll take the win. Shovel-ready effective altruist proposal for those with more funding than good ways to spend it: Fund doing this in other countries to the extent excess supply is available.
Speaking of wins, Scott Atlas resigns from the White House, and there was much rejoicing.
Sam Bowman asks rhetorical question mocking lockdown skeptics for not changing their minds after the vaccine was announced, gets replies from lockdown skeptics who changed their minds when a vaccine was announced. You love to see it. It is also worth noting that there are also good reasons to become more skeptical of lockdowns than before, since the virus is now less deadly and the political feasibility of lockdowns seems that much worse.
Yale professor evaluates college Covid-19 dashboards. Website itself is here. I am slightly terrified that my brain thinks offering point totals and a competition is likely the most effective and efficient way to get improvements in those dashboards. Only slightly, mostly I’m used to it. I love that the way they sort it is by athletic conference, so rivalries can be invoked. Go state! Congratulations to Amherst College, this week’s winner with the only A++. Unsurprisingly George Mason gets an A+, and unsurprisingly the Ivy League was far from the worst but did not cover itself in glory.
Blame Canada: Canadians, who have secured more doses of vaccine per person than any other country with eight doses per person or four full inoculations per person, point fingers because they tried to first make a deal with the Chinese. The deal fell through because the Chinese government blocked shipments of the vaccine, so the Candians couldn’t test it. In the particular case of the Chinese, ‘get your own data’ seems like a wise principle. I also think it is great that the Canadians are arguing over whether they did enough to secure vaccine doses, despite securing the most doses per person of any country and way more than are needed, because it was a huge error to get way more than was needed rather than way way way more than was needed. I have zero ethical issues with it because the surplus can and presumably will be resold to other nations when the time comes.
Covid-19 hypocrisy this week: San Francisco Mayor London Breed, Secretary of State Mike Pompeo.
Los Angeles Mayor Eric Garcetti locks down the city tight. All gatherings from more than one household are banned except for outdoor religious activities and protests. No being outside unless you are homeless, or for specified essential reasons. I presume his plan is to keep this up for several months. These are sufficiently strong restrictions that on the margin they are all but guaranteed to backfire even in pure infection terms. You have one of the few cities where it’s reasonable to do things outside, and you send the police after people doing things outside.
Not Covid-19: Our healthcare system is a dumpster fire, a continuing series, storytime regarding pricing edition. Also this. And this, where Canada has been forced to ban mass exports of prescription drugs because our plan to save money was to have Canada force drug makers to sell cheap and then buy from them in Canada and import the drugs back here, and that was threatening to create shortages in Canada.
Not Covid-19 but cool: Deepmind says they’ve solved the protein folding problem. This seems to actually translate to them scoring much higher than the previous high score on a protein folding competition. Which is neat but claims of having ‘solved’ the problem seem premature.
New model suggests that a consistent lockdown policy is better than an oscillating policy. Sharing for those who are curious. My quick reading says that they are completely missing all the interesting questions, because they are not thinking about control systems and how people will respond to various levels of infection, and they are assuming there is a generic lockdown knob that works.