

Covid 2/11: As Expected

Nothing both unexpected and important happened this week, other than that we might be on the verge of at least partially solving obesity.
There’s plenty else to talk about, but everything was on trend. That doesn’t mean my predictions were perfect or the speed of trends didn’t give us a few surprises, nor does it mean I could have written this post a week ago. It does mean that long term expectations haven’t much changed.
Vaccine efforts continue to be far too slow to improve, but to still improve slowly, including both distribution and approval. All current numbers continue to steadily decline, as they should until the new strains threaten to reverse that, which should still be a few weeks away.
While we can hope for unexpected good news, the more realistic and modest hope is that the lack of major news continues but things continue to steadily improve, and vaccine access improves dramatically in March after the approval of Johnson & Johnson combined with accelerating production across the board.
The Covid Tracking Project will be ending soon, and I still don’t have an great alternative source I love, so if you do have one (either for downloading data, for grabbing good data manually slash copy/pasting into a spreadsheet, or both) please suggest it in the comments.
In the meantime, let’s run the numbers.
The Numbers
Predictions
Last week: 7.7% positive rate on 12.7 million tests, and an average of 3,041 deaths per day.
Prediction for this week: 6.9% positive rate and an average of 2,750 deaths. Current trends should continue, with minimal impact yet from new strains, changed policies or increased vaccinations.
Results: 6.4% positive rate and an average of 2,968 deaths.
The 6.4% number isn’t shocking and was definitely in my range of plausible outcomes, but it’s pretty great. It’s even better than it looks, because our test counts are in rapid decline as well, from 12.2 million to 11.3 million, which presumably reflects lower demand. Things are improving rapidly, if not rapidly enough to stall the rise of the English strain, but things could plausibly be 25% better week-over-week, and that’s going to buy us time to improve further. This is reason to be hopeful.
The 2,968 deaths are highly disappointing, as that’s only a few percent less than last week. The 14-day-delayed-from-diagnosis-to-deaths rolling 7-day CFR went up from 1.29% to 1.57%, but on the other hand the 21-day-delayed-from-diagnosis-to-deaths rolling 7-day CFR went down from 1.34% to a new low of 1.25% (technically the low was 1.23% yesterday).
When looking at regional totals, I noticed that Indiana added 1,507 deaths this week that happened previously, as the result of an audit.
When you take those away, that drops the average death rate down to 2,752 deaths per day. Bullseye.
Prediction: 5.7% positive rate and an average of 2,450 deaths. Things should still continue to improve.
Deaths

DateWESTMIDWESTSOUTHNORTHEASTTOTALDec 10-Dec 16327853244376354116519Dec 17-Dec 23382651585131377217887Dec 24-Dec 30336336684171364014842Dec 31-Jan 6455341275019416217861Jan 7-Jan 13628039637383475222378Jan 14-Jan 20524933867207437020212Jan 21-Jan 27628132178151422221871Jan 28-Feb 3552430788071341020083Feb 4-Feb 10493741947165342919725
That’s a very large uptick in the Midwest, so the question is what is going on there. There certainly was never a corresponding jump in positive tests. Looking at the details, the explanation is that more than all of it comes from February 4 in Indiana, with 1,518 deaths. The Covid Tracking Project explains that these additional deaths come from a historical audit, so they’re not from last week at all. For this week’s update I’ll leave them in place, but will be editing the extra 1,507 past deaths out of the weekly charts going forward. At that point, things look normal.
Positive Tests

DateWESTMIDWESTSOUTHNORTHEASTDec 31-Jan 6428,407251,443494,090267,350Jan 7-Jan 13474,002262,520531,046306,604Jan 14-Jan 20360,874185,412452,092250,439Jan 21-Jan 27260,180158,737386,725219,817Jan 28-Feb 3191,804122,259352,018174,569Feb 4-Feb 10144,90299,451255,256149,063
Excellent progress. Not enough to overcome the new strain, but still very good, and even better accelerating improvement.
Test Counts
DateUSA testsPositive %NY testsPositive %Cumulative PositivesDec 17-Dec 2313,363,17211.1%1,440,7705.1%5.60%Dec 24-Dec 3011,300,92411.2%1,303,2866.0%5.98%Dec 31-Jan 611,649,64013.3%1,365,4737.3%6.45%Jan 7-Jan 1313,911,52912.2%1,697,0346.6%6.97%Jan 14-Jan 2014,005,7209.7%1,721,4405.9%7.39%Jan 21-Jan 2712,801,2718.8%1,679,3995.3%7.73%Jan 28-Feb 312,257,1237.7%1,557,5504.6%8.02%Feb 4-Feb 1011,376,5416.4%1,289,6034.2%8.25%
Vaccinations

Last week there were signs the growth in vaccination rate might be stalling out. Fortunately that has not happened, and supply continues to increase at a good clip.
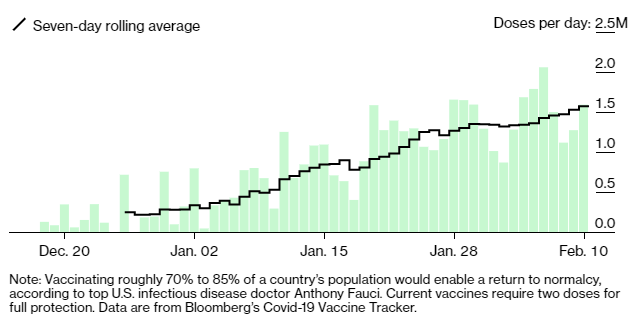
The current pace is not fast enough by any means, but if we can continue to grow at 20% week over week with the Pfizer and Moderna vaccines alone, it won’t be long before we get where we need to be.
It doesn’t feel like things are accelerating, because eligibility was expanded sufficiently that there are no appointments anywhere and no one has any supply, but that will change. As with many growing phenomena, more of the action takes place later in time than it would seem to people who have been paying attention for a while.
Globally things are mostly similar to last week, with Chile putting on a strong showing.

Europe

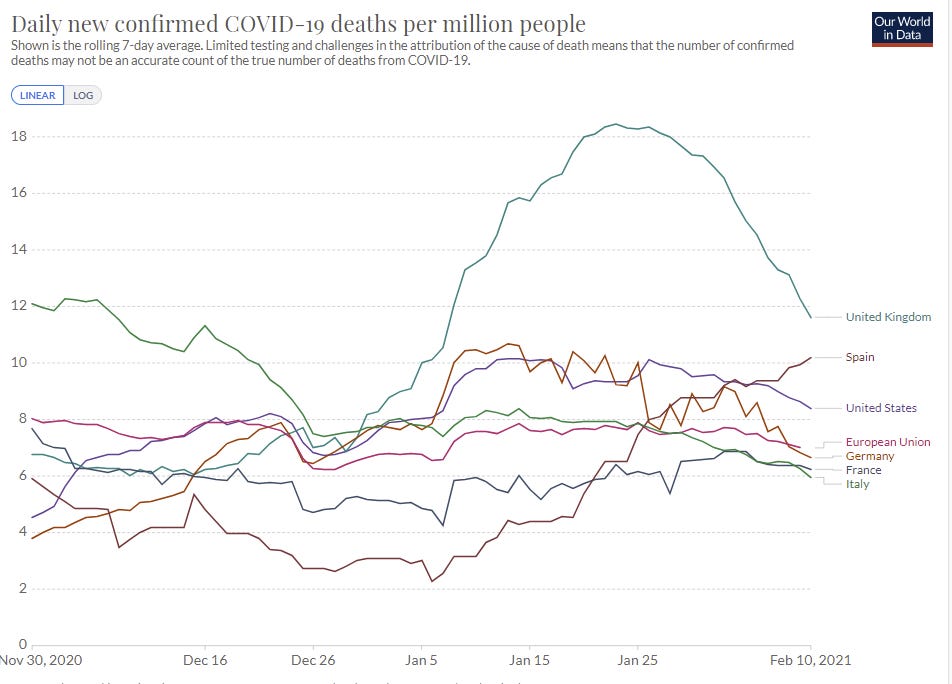
It is clear that the United Kingdom has contained the English strain through its countermeasures. The countermeasures in place elsewhere do not appear to be sufficient to do that, but the existence proof of the option is definitive. Things are generally improving everywhere, with Spain improving especially rapidly. As always, there are other countries with things going on but I post the same list each week to remain consistent and avoid cherry picking, with the USA on here as a comparison point.
Covid Machine Learning Project
Eric Topel interview with Machine Learning Project sole creator Youyang Gu.
Waiting on the English Strain
Some good news this week (science link):

Max says this is obviously very bad news, but whether something is good or bad news depends on your prior expectations.
If you previously had your head in the sand and were trying to pretend that the English Strain wasn’t more infectious, this is indeed very bad news.
If, however, you previously had accepted that the English strain was more infectious, and the question was how much more infectious, then news of the answer could be good or bad. In this case, it’s good.
This is an estimated 37% increase in infectiousness of the new strain versus the overall mix of strains. My initial version got this calculation wrong and forgot that there's already a lot of the new strain in Denmark, which pushes this into the 40s. Even that small difference is big, although other official estimates are still over 50%. Compared to 50%, even 45% is effectively much better. The difference is enough to give us somewhat of a puncher’s chance of things not being so bad, both buying us time and reducing how bad it is when the time comes.
This is roughly consistent with Kai’s framing of the data today, as well, depending on beliefs about the serial interval.
This is a common pattern. For a while in March of 2020, the stock market was reliably moving in the wrong direction on news. They’d see that things were shutting down and update that things were worse than they thought, whereas from my perspective things shutting down meant things were better than I thought, because I already knew that they should shut down and now they were at least both aware of the situation and thus actually shutting down. Which was good news.
So on that note, is this data point good news or bad news?
Vaccine Efficacy
This is an attempted Bayesian analysis of various vaccines and their likely efficacy against various severities of disease and against various strains. I say attempted because it seems like these take relatively generic prior distributions, and don’t adjust them much based on our understanding from other data points, including data from other vaccines. The result is that these distributions are likely underconfident, and in some cases biased, but it’s still a worthwhile exercise.
Waiting on Johnson & Johnson
The good news is that Johnson & Johnson has applied for emergency use authorization, and they are going to get it. There’s going to be a sprint to review the data in which every second will be used! Which started right after the official application, because you can’t review data that hasn’t been submitted in a completed application, that’s physically impossible, what are you even talking about.
The bad news is that it’s going to take three weeks to get to the meeting, likely with additional time after the meeting before we can distribute the vaccine, but hey:

Last week I went over how we know the Johnson & Johnson vaccine is safe and effective, and there are millions of doses waiting to be distributed, and there’s no good reason we can’t start that process yesterday.
I do realize that there is a difference between, as Scott Alexander discusses, the FDA’s need to be legible and reliable, and follow proper procedures, versus my ability to apply Bayesian reasoning.
That doesn’t mean this needs to happen three weeks after application, and attempts to justify that timeline are obvious nonsense.
Mostly, it’s a call and response. You say ‘why are we letting people die for no reason?’ and they say ‘Thalidomide!’ and ‘people won’t trust it.’
So basically, one time someone had a drug that wasn’t safe. We didn’t approve that drug because our existing review process made it look unsafe, so in response to that we created a more involved and more onerous process, as opposed to noticing that the previous process actually worked in this case exactly as designed. Then we use this as a fully general excuse to freak everyone out about everything that hasn’t gone through this process, and then use that freak out (that, to the extent it exists which it mostly doesn’t, is directly the result of such warnings) as our reason to force everything through the process. Neat trick.
Oh, and did I mention that the ‘safety data’ that requires three weeks to review is, and I quote it in its entirety, ‘nothing serious happened to anyone at all, and no one was struck by lightning.’ Either J&J has created a safe vaccine, or J&J is committing a fraud that will be caught and get everyone involved arrested within three weeks, or they’re committing a fraud so effectively that the review won’t catch the fraud and won’t help. Those are the only possibilities. If the data isn’t fraudulent then the drug is safe, period.
It’s one thing to have Asymmetric Justice. I get that the FDA has to act as if damage from permission is orders of magnitude more important than damage from lack of permission, despite how awful that is for people’s lives, but how many orders of magnitude are we talking, and once you pick a number can you then show your work?
Do we already know the vaccine is going to be approved? Well, not quite, but...

Hang on, question incoming! Well, I’ll be damned, that’s not a 99 at all...
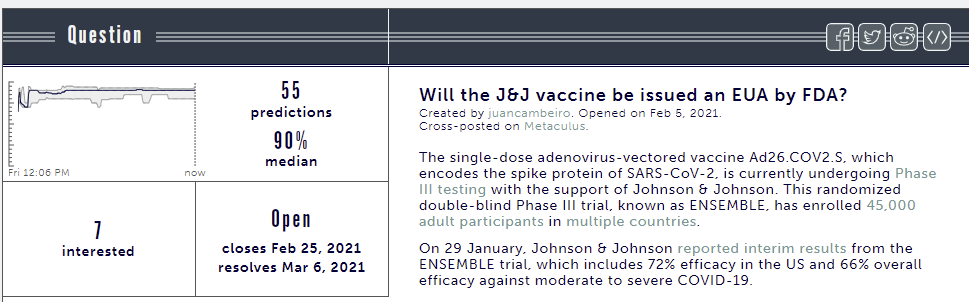
The question is actually kind of weird and terrible - if they move the meeting or issue the EUA before the meeting it resolves to ambiguous and is cancelled, so the question it’s asking is ‘conditional on having the meeting without approval do they then issue the EUA within 7 days’ and that’s not the thing we actually want to know. We want to know if the EUA will eventually be issued one way or another, whereas this question is actually mostly measuring whether they drag their feet so long it takes more than a week while they hash out the exact minimum age and procedural guidelines, or something.
Also, I broke down and joined Metaculus for this question because 90% seemed crazy low, and this is not how odds work this is not how odds work at all:
But then I checked another question, and hey, you know what gets one even more internet points than good odds?

Everything’s made up and the points don’t matter. No, I didn’t lock in that second prediction, and I believe I’m probably done with metaculus. I can’t even. Change my mind.
On the actual J&J vaccine, I don’t know what more there is to say. As with Moderna and Pfizer, they’ve already done the actual approval process and confirmed that it’s going to get approved before they applied, and now we’re delaying in order to make it clear we are Very Serious People who Follow Proper Procedure and are not In Bed With Industry and Putting People At Risk or Destroying Trust in Vaccines by going ‘too fast.’ Or something like that.
We have now done this three times. It’s one thing to have the first vaccine application point out that there’s weeks of lost time. It’s another thing to not have fixed the problem months later.
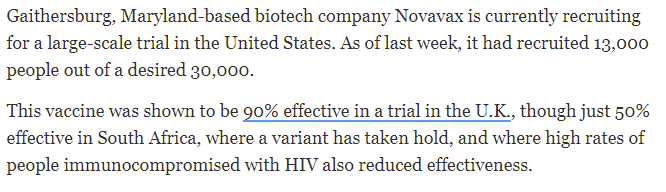
Waiting on Novavax
From the USA article on Johnson & Johnson, we learn exactly what is holding up Novavax, and the problem is a straightforward case of Not Clinically Trialed Here:
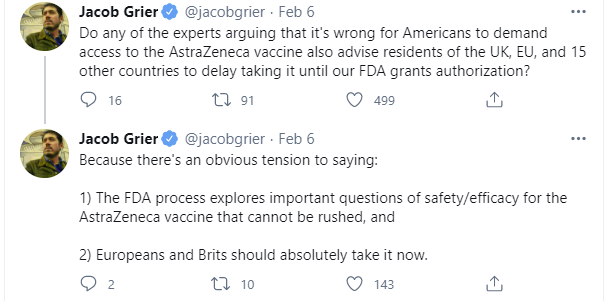
Waiting on AstraZeneca
If Novavax needs an American trial, I guess we have our answer on AstraZeneca.
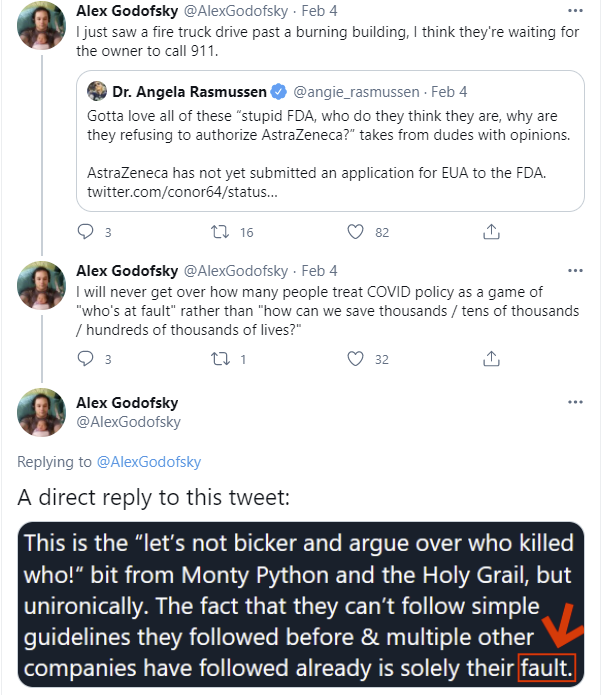
This cuts to the heart of how unserious, perverse and malicious non-approval is at this point:
Not counting implicit arguments from full-on anti-vax people, I have yet to see one single person argue that we should undo the approval of AstraZeneca in the UK or EU.
Nor did I see a single call for stopping the use of the AstraZeneca vaccine in South Africa. That’s presumably because this would be a really stupid move. There was a small and therefore underpowered study of the AZ vaccine against the South African strain, which is easy to misinterpret since it couldn’t conclude anything definitively due to lacking sufficient power. The AZ vaccine still clearly provides some protection against infection by the South African strain, and likely greater protection against severe disease, and it’s safe, so what’s the downside to continuing to give it out?
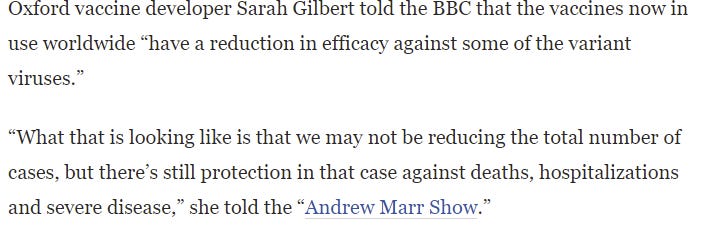
Certainly if the choice is between ‘some reduction in deaths, hospitalizations and severe disease’ and ‘no thanks, we prefer the full quantity of deaths, hospitalizations and severe disease’ this choice should be clear enough.
You would, of course, be wrong about that. South Africa did stop the use of the AZ vaccine (WaPo), and again, I have not heard any experts point out how suicidal that decision is, although shifting future vaccine purchases to other vaccines did make sense.
This follows the pattern that ‘expert opinion’ on what to do is primarily defending following elite decision making. I’ve been underestimating this effect, but the pattern is increasingly clear. If the properly respectful elites with the power (e.g. basically anyone powerful except the Orange Man) decide not to do X yet, the ‘experts’ will talk about how we must follow proper procedures before doing X or else risk catastrophe, or how X is damaging or unethical or something. Once the properly respectful elites decide to do X, whether or not they followed the procedures the ‘experts’ were defending earlier, the ‘experts’ might briefly decry the skipped procedure, but they will immediately pivot to defending X. There’s presumably some value of X sufficiently awful that the ‘experts’ wouldn’t do this, but we’ve yet to prove that by example.
So we have the same vaccine sitting in storage unused in Baltimore, while failure to secure and deliver enough of that same vaccine for current use is a continent-wide scandal in Europe.
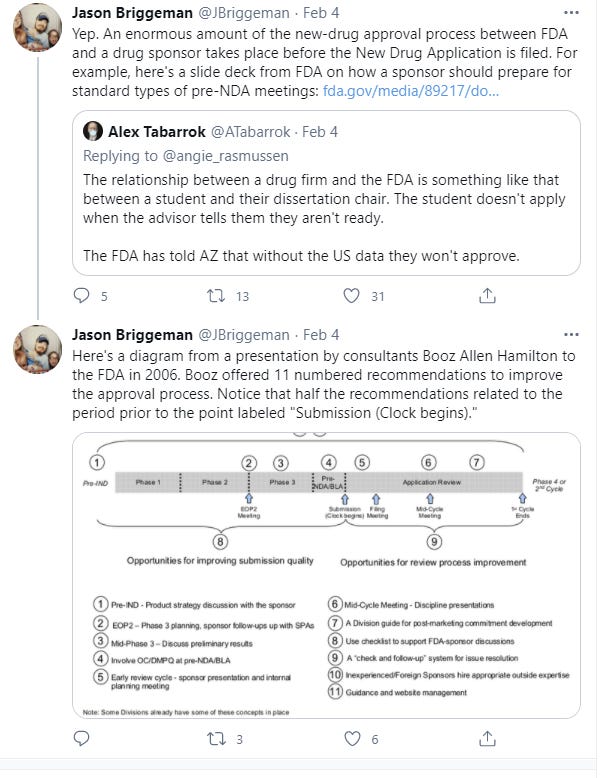
And in case it wasn’t sufficiently clear last time, the reason AstraZeneca didn’t apply is that they’ve been told not to and that they’d be turned down. That’s how the process works, you’re in constant communication and only apply when you have what is necessary.
Or, with the attitude the situation deserves:
Waiting on Demand Shortfall
First we had a shortage of eligible arms into which to put shots, resulting in lots of needless delay. We were so obsessed with prioritization and what was fair that we threw doses away while letting others sit on shelves.
Then we got to the current phase of the vaccine rollout, where there is an abundance of arms and not enough shots to put in those arms. Now we are thankfully using all our doses, but with a train wreck of a prioritization scheme that places lots of people at minimal risk (e.g. anyone with a BMI of 30 in many places) in competition against seniors for shots, while destroying the legitimacy of the prioritization system. It’s worse than nothing, but far better than too much, and the focus rightfully has shifted to finding more doses faster, increasing production, cutting vaccine doses where we can and approving new vaccines quickly.
The question is how much and when to worry about the transition to the third phase, when we have enough vaccine and the limiting factor becomes people’s willingness to get vaccinated.
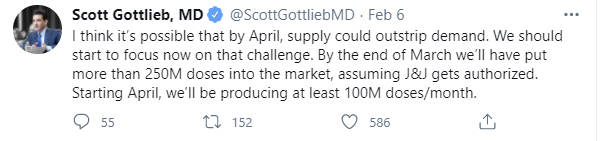
Possible is not the strongest word, but the other part of this statement is claiming relatively high confidence. The key question is whether the 250M doses target is real and how much of that is one-shot J&J doses. If we hit that mark, then our chances to get everyone in the ‘eager to get it’ group done by April look reasonably good.
Peter Hotez, in the linked thread, has been hearing the other half of the news reports, and also echoes the same range I have for how long we have before the new strains take over:

We can and should do our best to move the needle but the most important practical question in so many of our lives is which of these two reports is right. Will we have sufficient doses for ‘the eager’ in April, or will it be waiting until at least June?
Shall we check in with the Good Judgement Project?
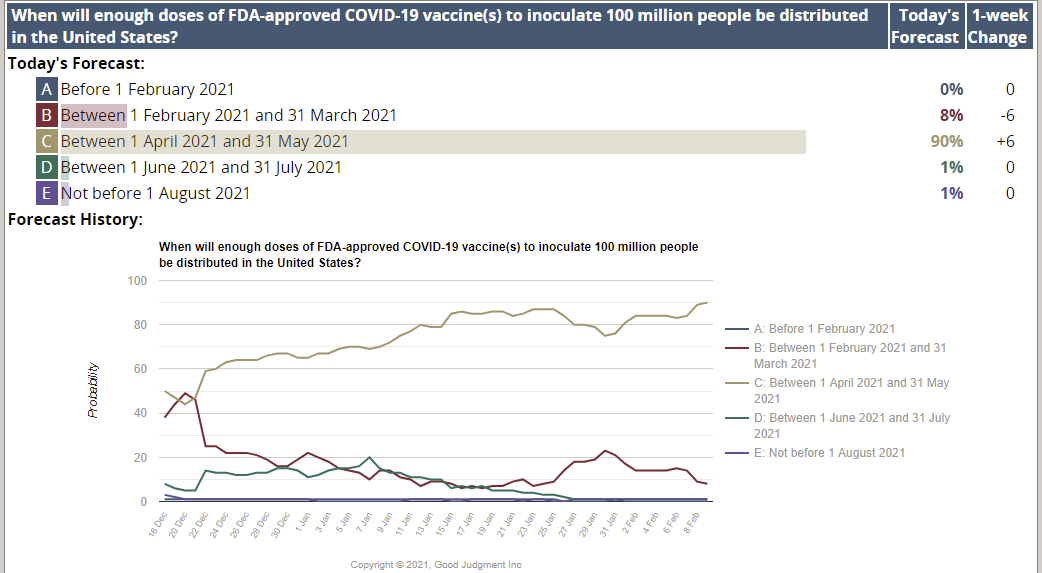
There continues to be very high confidence that the necessary doses will be distributed by the end of May. As usual, they are overconfident and C is nothing like 90%, but the level of confidence still speaks volumes - Scott Gottlieb is making an explicit prediction of outcome B, and Peter Hotez is soft expecting option D.
Doing quick math, if Scott’s other half of the equation is right and there’s only ‘deep’ demand for 50-75 million vaccinations, then compare that to our current pace of 1.5mm+ doses per day, or 750k people vaccinated per day with 44 million shots already administered. Getting to 150 million shots from here would only be two months (mid-April) even if we didn’t accelerate from here. So it seems like the end of infinite demand, and the shift to a potential demand shortfall, is likely rather near.
You know what isn’t helping with that?


I could not be more contemptuous and sick of the ‘nothing changes when you get vaccinated’ position. Or even this nonsensical ‘we don’t know’ position. I took a graduate level course in epistemology where it was called into question what it means to know that some proposition P is true, and whether we can actually know anything at all, and that’s all quite interesting as philosophy, but for practical purposes yes we damn well know this stuff.
How bad is it? It’s pretty bad:
My guess continues to be that this hesitation will fade with time. Wait for the people who actively want the vaccine to get it, and then everyone who can’t do their job without a vaccine to get the vaccine, and then we’ll have many months of tens of millions of people as clear evidence that the vaccines work, and a lot more people will follow. Thus, I’d be inclined to mostly wait on the public service campaigns until then, when people will be able to act if convinced and we’ll have an easier time convincing them.
I also notice that there is a large part of me that thinks, once it’s easily and widely available, you know what? Straight up, just f*** ‘em if they don’t want the vaccine.
Suppose it is June 15, and there are open same-day appointments outside of work hours at half the pharmacies in America. The good stuff, too. Anyone who wants a free shot of Moderna or Pfizer can get a free shot, no questions asked.
Remember, we seem to have vaccines that are almost 100% effective against death and severe disease, and everyone’s had the chance to get vaccinated, and can change their mind at any time.
Why not simply go back to normal? If the other half of America doesn’t want the vaccine, all right, fine. Some of them can keep hiding in their houses for another year if it suits them. Others can walk around vulnerable and shake everyone’s hand. This large part of me really, really doesn’t care. Still do the PSAs and all that, sure, but it’s their lives on the line. Either we’ll still contain the pandemic anyway, or the ones who are out there unvaccinated taking big risks will infect each other, and that will burn itself out, and then either way we can all move on with our lives.
I don’t endorse that position on reflection or anything, but it seems important to have the courage to note that it is there.
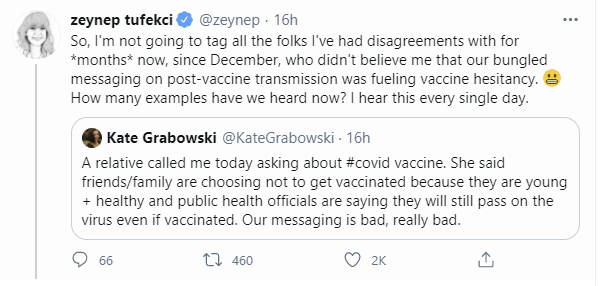
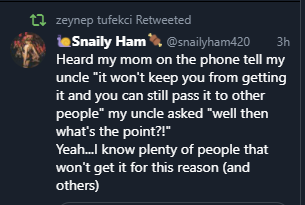
In particular, the whole ‘we’ve told people that the vaccine won’t stop them from getting Covid or from passing Covid to others or let them resume their normal lives, so why the hell should we expect them to take it?’ counter-argument is getting stronger every time Zeynep retweets another example, and her list is getting long.
Vaccine Allocation By Politics And Power
New York joins the club letting those who technically have a ‘comorbidity’ of a BMI of 30 get vaccine priority while seniors continue to be unable to book appointments. How the wheel turns. Looks like the list at least excludes smokers.
Americans are really fat. How fat are they? What say you, Wikipedia?
The National Center for Health Statistics estimates that, for 2015–2016 in the U.S., 39.8% of adults aged 20 and over were obese (including 7.6% with severe obesity). Luckily in my first reading I'd mixed up which statistics are referring to BMI of 25 vs. 30 (they use the same words in different places to refer to both, but still totally my fault), and it's only that 39.8% that are eligible in this fashion via the BMI threshold, if everyone is scrupulously honest and doesn't game the system in any way.
Right away, the main mailing list I am on had one person note that he was four pounds short of qualifying, and a plan was quickly formed (I believe and hope in jest but these days who can know) to eat some carbs and put on a little water weight to get over the top. There seems to be a lot of somewhat serious talk about putting on a few pounds to hit the cutoff point.
Of course, a better strategy is to just lie, it’s not like anyone is going to weigh you. This isn’t a boxing match.
I wonder how much long term damage this is going to do to people’s health by demotivating healthy lifestyle choices, the same way I worried earlier about the impact on smoking rates. I don’t think these impacts will be worse than the health effects of the pandemic, but if you think that kind of damage is impossible here, you have not done the math.
Meanwhile, in Georgia, health officials saw that a clinic was vaccinating teachers believing them to be essential workers, who the state then decided were not yet eligible under local rules because they are not ‘essential workers,’ and responded to this cartoon villainy by raiding the medical center, confiscating the vaccine supply and promising not to deliver any more doses for six months.
Meanwhile, in Boston, priorities are straight:
Meanwhile, in Harris County, a doctor gave out rapidly expiring doses, was fired for it and is now being prosecuted. Can’t link to the story because NYT but it’s easy to find if you want details.
While others get the vaccine because they run a microbrewery, which is classified as ‘essential manufacturing’.
You can’t undo eligibility that’s been granted. I mean, sure, you can, but it’s pretty terrible. What’s done is done. We’d be better off without eligibility rules at all, and relying on people to use their judgement and their willingness to invest time in the process as allocation methods (despite the ability to do this being anti-correlated with actual need to get the vaccine, both in terms of exposure and vulnerability), since we are unwilling to use price.
For example, if you want to test how much people want to get vaccinated, you might give them eight different ways to book an appointment in the same county, and see who is willing to try all of them.
When people do start trying to use your systems, what happens?
Occasionally someone gets this part right, and we’re actively surprised:
You Should Know This Already (Inessential Reminders)
If protests do anything at all, there should be pro-vaccine protests.
The WHO is suddenly enamored with the ‘frozen food’ hypothesis for the origin of Covid-19, which would claim that the virus didn’t even originate in China, and I will leave interpreting what is happening there as a (very easy) exercise for the reader.
If you’ve already had Covid-19, the second dose is likely not helpful to you. The first dose will have been enough. The second dose also knocks a lot of people on their ass for a day, so if it isn’t helpful one would actively want to avoid it for one’s own sake, plus it gives that dose to someone else who still needs it.
Immunity from old strains, study says, does still help against new strains.
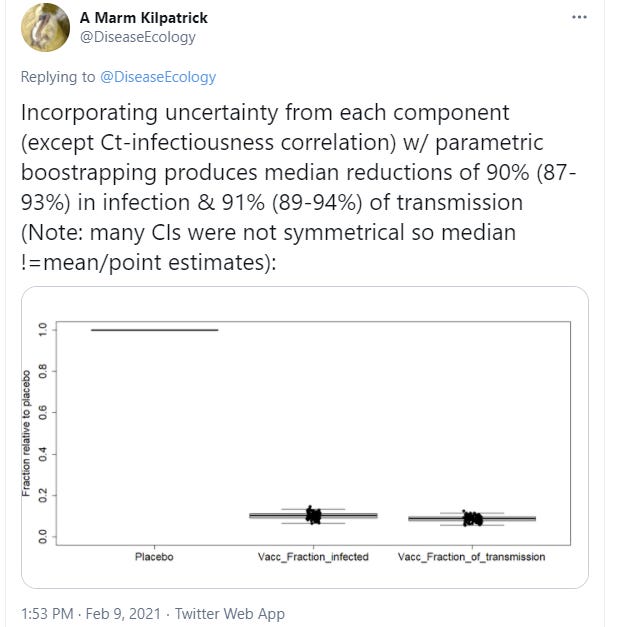
Pfizer vaccine continues to post great results, in this case low viral loads.
There was a comment about Scott’s article and my response to it that said that vaccines like Johnson & Johnson’s are always one dose, so my saying that it was good they didn’t test a second dose was evidence that I was incompetent and shouldn’t get anywhere near the CDC. That example looks rather interesting now a few days later, as they begin a two-dose trial of the Johnson & Johnson vaccine.
Exactly how good? In the way that counts the most for you, about 100% effective:

The best way to improve productivity and efficiency is to do the thing, in this case Pfizer using their experience to double production. Which they could have done last year. It occurs to me that if we had offered to pay $100 per dose for mRNA vaccines all of last year and then tossed them into the trash after testing their composition rather than even bother storing them we’d be done with this pandemic by now.
An article writing up people’s efforts to create tools to help with booking vaccine appointments.
The UK vaccine rollout is considered a success, and by the standards of other results, it is indeed a success. This interview explains how they did it, which was essentially ‘make deals with companies and pay them money in exchange for doses of vaccines.’ They still did much less than a sufficient amount of that across the board, and it doesn’t seem like anyone involved grokked anything like the full speed premium or the need to overspend, but they at least threw some effort in the right directions.
How do we know politics has returned to normal? “News stories” like this one on Fox News, complaining that Biden was travelling by plane despite CDC warnings not to travel. That’s how you keep life, liberty and property relatively safe while the legislature is in session.
As much as I go after the FDA, at least they did approve the most effective vaccines, whereas in India Pfiizer has now withdrawn its application because of the need for ‘additional information.’
The army has now completed the process to issue the Combat Cloth Face Mask. The process worked as designed and only took one year, at the low cost of $45 per cloth mask. The army is congratulating itself on the “expedited timeline.”
Cases are declining across the world, here’s an analysis of why that comes down to behavioral changes combined with ~30% of people being immune due to prior infection and that allowing us to turn the corner. He points out that temperatures of various places don’t much correlate with current trends. Of course, as the new strains take over, this progress will by default be lost and reversed, and current levels overall remain quite bad.
If you don’t believe that the bulk of infections come from people who are choosing to take a lot of risk, that needs to be squared with people constantly taking lots of risk and announcing they’re taking lots of risk, like this 62 year old proudly shaking hands with whoever is willing.
Department of it can always get worse: Any month no one is vaccinated sure sounds like an inauspicious month to me:

Still combined with remarkable amount of can-do spirit (article):
Ministry of Truth
There used to be a robust consensus that the right to free speech, both in law and in practice, from threats both public and private, was one of our core values. I would argue it was the core value. There is now an increasing consensus against the right to free speech. This has progressed from the rapidly expanding umbrella of ‘hate’ speech (regardless of its truth value), to speech in support of the political outgroup or against ingroup causes that the Powers That Be have decided to proclaim as false or dangerous.
Increasingly it also applies to health claims that are in conflict with Officially Recognized Sources of truth. Like the WHO, FDA and CDC.
Professional retaliation for speech in some cases has extended to merely having joined (likely to reserve a preferred username) social networks that have arisen as alternatives to this censorship, even the person in question ever having posted anything at all on such networks. Why would you have access to a way to say something, if you didn’t have something to say?
We face increasing levels of Kolmogorov Complexity, and are told to say that thunder proceeds lightning. More and more true facts are only stated privately in whispers, or implicitly and esoterically within other statements.
I write these posts on WordPress and they are reposted on LessWrong, which has strong norms around front page posts, but a very strong commitment to not censor personal blog posts, and which provides a robust backup in case someone tries to get my content taken down. Ideally I’d fully self-host as well but I haven’t put in the work. We live in times when even outlining my model of the physical world of a pandemic makes it feel necessary to see the entirety of my technology stack and where pressure might be brought to bear. A few years ago such considerations wouldn’t have occured to me at all.
It has been my belief for a while that if I was posting my full content on Twitter, Facebook or YouTube, that it is likely my content would have been taken down and censored.
It is not a helpful policy to take down information for not lining up with the official government position. That is not how one inspires confidence and trust, or identifies error and discovers truth. There’s also the small matter that the official positions frequently reverse themselves.
Now it seems Facebook is expanding this policy...
The public approves and wonders why shutting down bad speech took so long:

Here is Zeynep explicitly violating Facebook’s official policy by stating true facts:

If a regular person says vaccines don’t provide immunity, they’ll be censored. If a newspaper writes that we don’t know that vaccines provide true immunity and therefore everyone needs to keep social distancing and mask wearing forever even when everyone involved is fully vaccinated, that’s the mark of a Very Serious Person, and also the recommendation of the CDC.
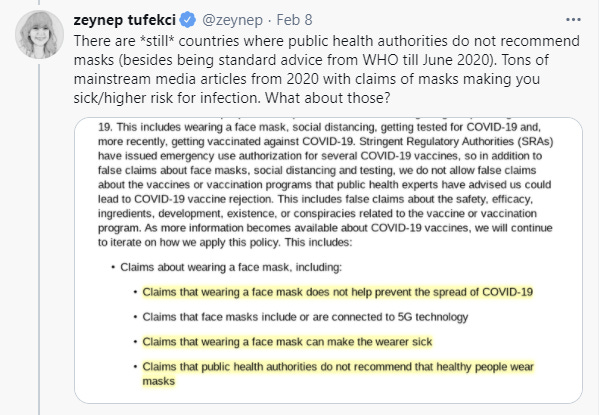
Shall we follow Zeynep’s example, and violate this policy a bit more by making more true statements about the physical world? Let’s take a closer look at the policy and see what else we can find.
There were a lot of opportunities to violate this policy with true statements, so I’ll limit myself to two (a previous version had a third which I had misread).

The group of young children can potentially be infectious to others, but are effectively immune and cannot die from COVID-19.
The specific treatment of getting vaccinated or having previously been infected then recovering results in immunity.
These aren’t trivial gotchas. Both of these cases seem somewhat important.

The original source of Covid-19 infection was not human-to-human transmission. It is generally believed to have been caused by consumption of an infected bat from a Chinese wet market in Wuhan, but there are alternate theories as well, including the WHO’s would-hilarious-if-it-wasn’t-real new ‘frozen food’ hypothesis, and also those who claim it escaped from a lab (which is another claim explicitly prohibited by Facebook). I’ve chosen to consider such questions of origin out of scope for these posts, but we know for sure it wasn’t human-to-human transmission.
On the flip side, love this exchange:
And also I wonder if they’ll be enforcing this one against a lot of journalists and “experts”:
I’m glad to hear that it’s now official that the vaccines are effective in preventing Covid-19, and I’m confused why Very Serious People keep telling everyone otherwise while also wondering how to get more people to want to take the vaccines. Life is so weird.
It seems that all this is being directed by the WHO:
It is well-known that I am Against Facebook but these concerns have nothing to do with my existing core objections to Facebook, other than taking ‘Facebook decides what I see and don’t see, is manipulating me for its own profit and I can’t count on seeing anything or having anything I say be seen’ to an entirely new level.
Since I am only on Facebook purely to exchange contact information for communication elsewhere, plus the occasional messenger conversation that can’t be avoided, I don’t have a read on the effective level of enforcement of these rules, or whether such enforcement is being done in a reasonable fashion. I do know that I continuously see reports of suspended or even terminated Facebook and Twitter accounts with no explanation or one that makes little sense, and no practical ability to appeal the decisions.
I do think that being kicked off Facebook will often be a blessing in disguise, but that doesn’t make it right. If you value your Facebook account, please reconsider that position, but meanwhile guard and bite your keyboard’s tongue.
I am thankful that I am in a position where I need not worry about retaliation, for the same reasons I am in a position to devote time to writing this. Most others are not so fortunate.
To anyone who says ‘this isn’t the government doing it so it doesn’t violate free speech’ or ‘there are plenty of other places to go all you have to do to have a platform is Create a Full Alternative Stack (including your alternative to AWS, if not yet an ISP), think about the practical implications of that. Does anything even need to be said?
In Other News
Video (3 minutes) on how to properly fold a surgical mask.
In case it wasn’t clear yet, Zeynep Tufekci is doing great Covid-19 work, and I’m finally following directly after far too long via the Twitter feed here. There’s also a substack here.
Zeynep reports that the University of Berkeley has banned outdoor exercise. How do they think that is going to go? Do you think students are going to obey your restrictions in ways that make them take less risk? Do you think they’re going to cooperate with your contact tracing?
Israeli hospital claims it might have a cure for Covid-19, dubbed EXO-CD24. They’re saying it helped 29 out of 30 patients in serious condition. I have no idea how promising things are at this point, but figured I’d pass it along. They are coming out of Phase I and applying to begin Phase II.
A key part of the story of 2020 has been that life under social distancing is diminished life, people’s lives and livelihoods are hanging by a thread, and things are generally quite bad. The most concrete illustration of this was supposed to be a higher suicide rate, which seemed like it had to be true. Except, there’s a claim that suicide wasn’t up last year, despite being up generally in recent years?
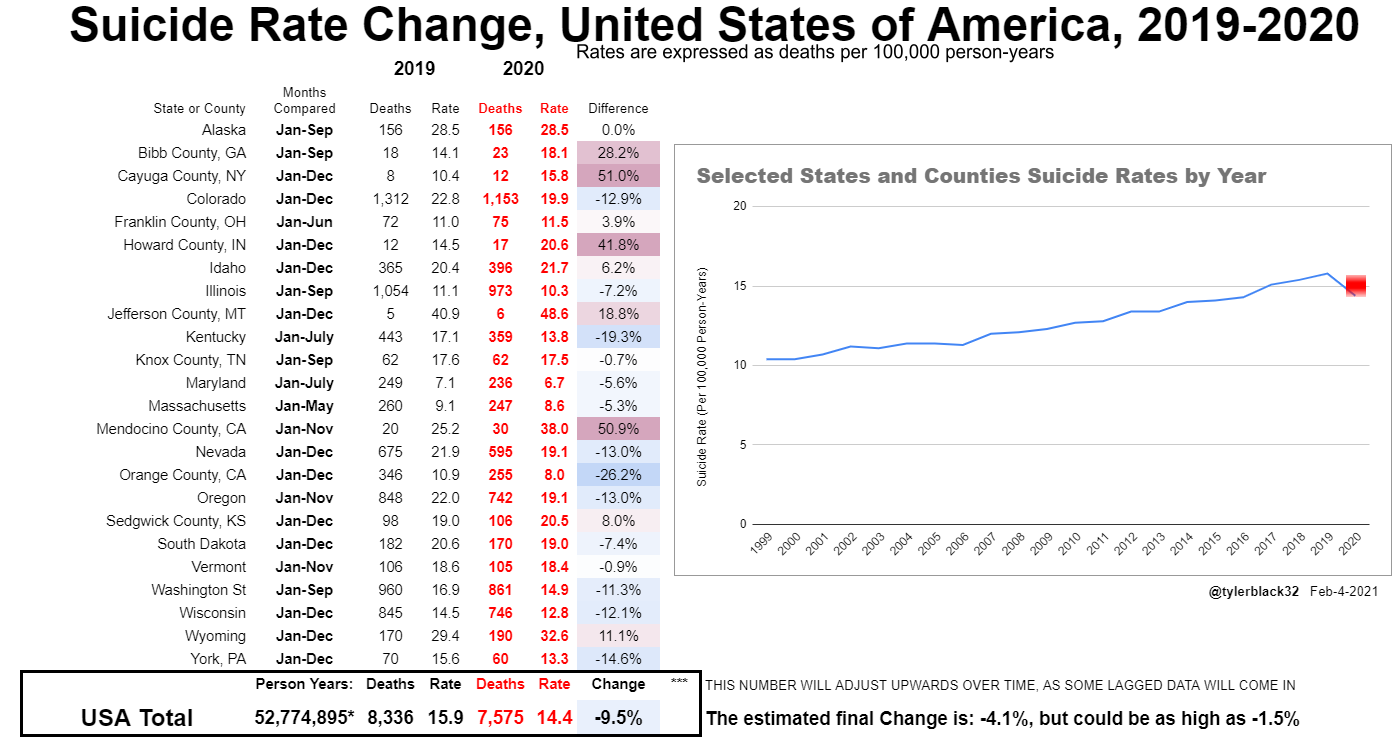
This shows a clear steady increase over the last two decades that is pretty alarming and didn’t get the attention it deserved, but a decline last year of 9.5%.

Paper and thread on seroprevalence in India.
Biden has not yet appointed an FDA commissioner. The key qualification should be whoever promises to get the vaccines approved quickly, the tests approved quickly, and also things like filling in the vials of vaccine approved quickly. Once again, I suggest Solomon Mowshowitz, or failing that, Scott Gotlieb is always available.
CDC recommendations for how to do things relatively safely, with a remarkable lack of ordering everyone to do nothing forever. I was amused by the following example of accidental honesty, the classic reverse-no-evidence:
I mean, none of this is wrong or anything, on the margin this is good advice where available. Now can we have a talk about what it means when there’s ‘no evidence’ of something, and why one might want to act as if that thing was probably true anyway?
Not Covid but exciting result of new potential weight loss treatment. As usual, I make no claim that this is a legitimate result or that we should expect it to hold up, but this is the sort of problem that could plausibly have a mechanical solution that simply works - weight loss is up there in hardness with steel, diamonds and knowing thyself, but there’s no reason that has to be true. I’ve got the weight loss quest handled, but if there was a solution that also let me eat three meals a day, or even reliably eat two, that would be awesome.
The early signs point to this being legit and super exciting, as Sarah Constantin is one of the people I trust most on such matters:

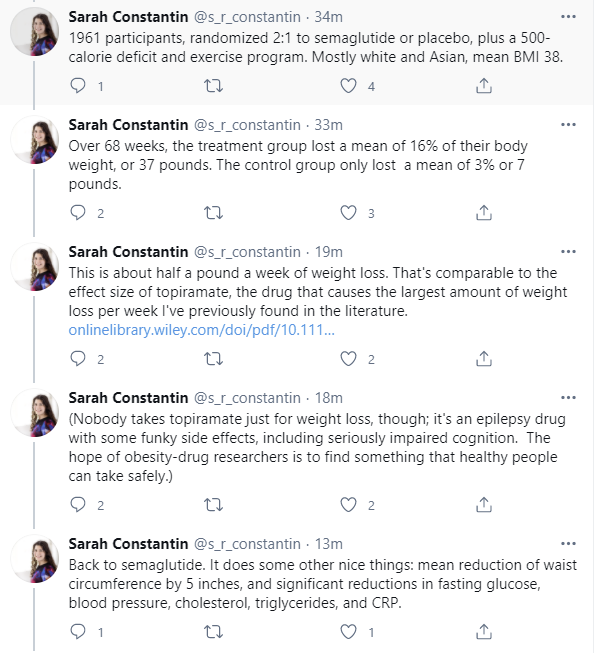
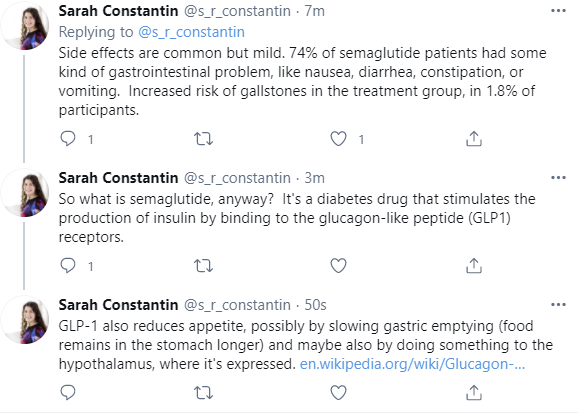
I’d want to do a bunch more consideration before getting such a treatment, but Humanity, Fuck Yeah!