

Covid 3/12: New CDC Guidelines Available

This post is a day late although not all that short, as I warned it might be. This is because I have spent the last week visiting the best place on Earth, my true home, which is New York City. I will return again soon, and soon after that I will once again be able to live there. A great moment. I hope to write about the trip, but I need to get this post out quickly, so that won’t make it in this week.
This week had three (other) big discrete things happen. The CDC issued unexpectedly sane guidelines for vaccinated people, and thanks to the day of delay, we also have Biden announcing a date that everyone will be eligible for the vaccine. Finally, on March 7 the Covid Tracking Project stopped collecting data, requiring another phase transition in much of the data and leaving me without a source for detailed positive test rate data that I’m happy about.
We also had a bunch of opening up around the country, despite what is obviously about to happen.
Let’s run the numbers.
The Numbers
Predictions
Last week: 4.2% positive test rate and an average of 1,827 deaths after subtracting the California bump, using Covid Tracking Project’s final week of data.
Last week’s prediction: No prediction due to some combination of ‘somehow I forgot to do this’ and the expected lack of data collection making it difficult to fairly evaluate the prediction. We’ll start again fresh now.
(My (highly unreliable guess you should not trust to match what I would have said) would likely have been to see small declines, to something like 3.9% positive rate and 1,650 deaths, which absolutely does not count for anything as a prediction but does give a sense of vaguely where expectations were a week ago.)
This is the testing trends chart from Johns Hopkins, a plausible new data source.
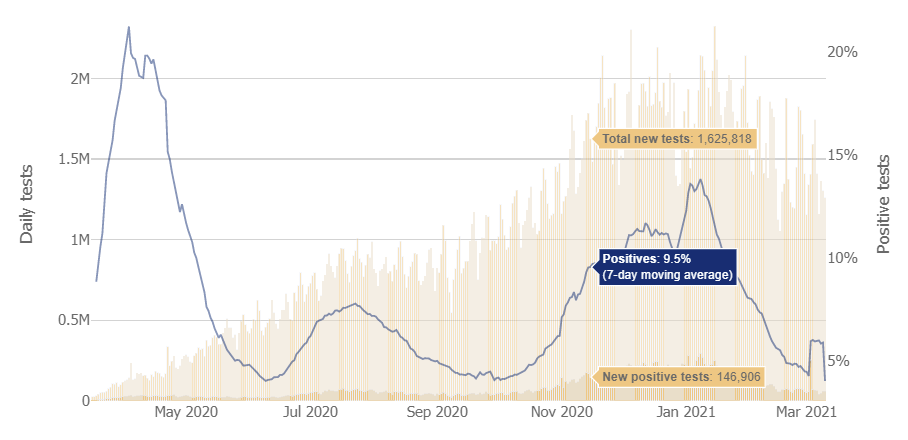
I hate when I want charts and all I get are graphs, and also note that phase jump up and down, and also when you highlight a day it doesn’t tell you what date that is so unless you can work backwards from the final day (and this doesn’t make it that easy to know what the final day is, if it might or might not have updated yet) everything is super fuzzy.
The phase jump here appears in their data in some states and not in others. It’s clearly not ‘real.’ For now, I’m going to presume that the new 4.0% rate at the end is now calibrated however the old numbers were calibrated at the Covid Tracking Project, and ignore the numbers in-between.
Result: Thus, I will conclude that likely the positive test rate did indeed fall slightly, from 4.1% to 4.0%. Deaths fell from 1,867 to 1,374 (!).
Another possibility is the Washington Post, if you’re able to reliably check it on the right day before it updates:

Those are the headline numbers we need in easy to see form, so it makes sense to predict on those in relative terms. Note the 19.5% decline in the number of tests, which indicates that cases falling by 11.3% should be concerning.
Prediction (WaPo numbers): Positivity rate will be 4.2% (unchanged) and deaths will fall by 12%.
Deaths should continue to fall since they lag substantially. Cases could go either way, depending on the impact of the new strains and how people react to reopenings.
The search for a better data source continues. Wikipedia is still good for raw positive test numbers and for deaths.
Alas, the Covid Machine Learning project from Youyang Gu is also wrapping up due to the Covid Tracking Project no longer gathering data. I hope someone gets us a new version with a new data source, but Gu has already gone above and beyond.
Deaths

DateWESTMIDWESTSOUTHNORTHEASTTOTALJan 21-Jan 27628132178151422221871Jan 28-Feb 3552430788071341020083Feb 4-Feb 10493726877165342918218Feb 11-Feb 17383722215239270013997Feb 18-Feb 24365224334782242713294Feb 25-Mar 3383416695610195813071Mar 4-Mar 1025951775371415399623
This is clearly wonderful news and deaths are rapidly on the decline. I worry there’s data artifacts here because the death counts on March 7 and March 8 are so low (e.g. 562 on March 8, and before the 7th the last day under 1000 deaths was November 29). For a while it’s been an increasingly large mystery why deaths haven’t fallen faster, and now they’re falling an amount that reasonably tracks declines in cases. Whew.
Positive Tests

DateWESTMIDWESTSOUTHNORTHEASTJan 28-Feb 3191,804122,259352,018174,569Feb 4-Feb 10144,90299,451255,256149,063Feb 11-Feb 1797,89473,713185,765125,773Feb 18-Feb 2480,62564,857150,493110,339Feb 25-Mar 366,15158,295151,253115,426Mar 4-Mar 1062,93557,262114,830109,916
This is disappointing news, as is the positive test rate. The decline in the South is impressive, but the other regions are stalling out, and the decline in the South both likely reflects a (slightly) artificially high number last week, and conditions that have since loosened considerably in major areas including Texas. Our march straight down to zero will have to wait.
The next few weeks on this chart will be the moment of truth. If cases don’t pick up by the end of March, they’re likely not going to pick up at all from the current wave of variants, and vaccinations will have enough time to dominate. If cases do pick up, it’s going to be very difficult to pivot quickly.
Vaccinations
(Data here is as of March 12 rather than March 11, so it’s 8 days after last time.)
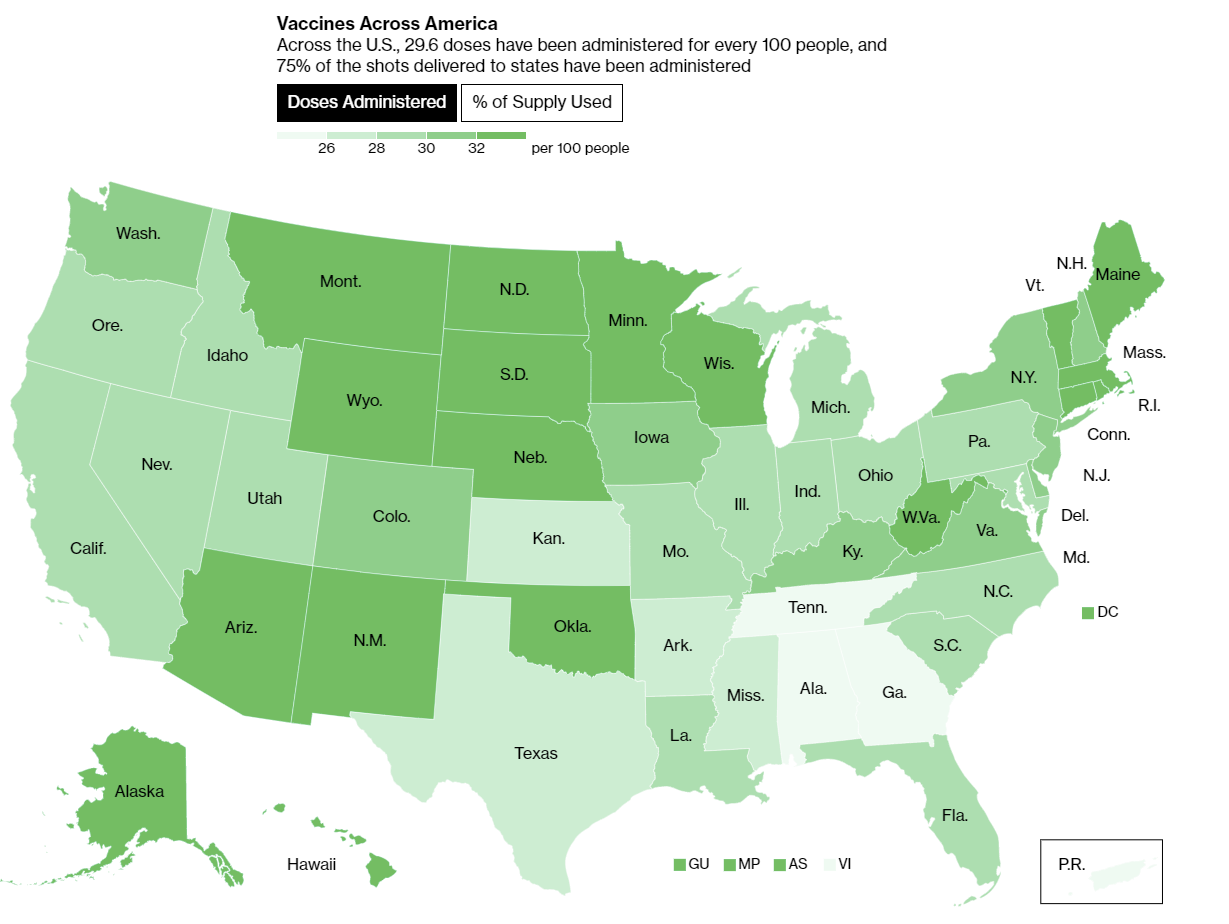
Not only is it clear we can sustain and further increase this pace of vaccinations, we are building up an increasing surplus of vaccine doses, and getting appointments is becoming steadily easier in most places.
We had (and continue to have) a ton of unforced errors along the way that caused (and continue to cause) massive delays, but we are on a clear path to vaccinations on demand for every adult within a few months, and yesterday Biden made that official (WaPo). Every state has been directed to make the vaccines available to everyone over the age of 18 no later than May 1, and Alaska has already gone first and opened up vaccinations to all adults.
Biden delivered the announcement and the rest of his speech well, highlighting that while not everyone will be able to get vaccinated on May 1 or that soon after May 1, at least everyone can get in line on May 1, and emphasizing the need for basic safety measures for now. Needless to say, there was no discussion of cost/benefit, or why we did something very different from this earlier.
Meanwhile, Biden continues to double down on underpromising to maximize the chances of being able to claim overdelivery on all fronts. Meeting one’s 100-day vaccination goal in 60 days without anything unexpected happening that much impacted the pace is more of a sign that you set a very low bar than it is a sign that you went above and beyond.
It is also important to note that we have a strange two-tiered prioritization system. If you are actually high priority, mostly via being elderly, you can get a vaccine appointment (in at least many places) at pharmacies without competing against people who checked a box saying they once smoked a few cigarettes. If you are technically eligible, you can use one of the less convenient, harder to book vaccination sites, or go overnight for Johnson & Johnson.
Compared to most plausible alternatives, this is all actually pretty great. We’re not allocating by price in dollars, but we’re allocating by price at least a little. Rather than be obsessed with exactly what order people get shots in, we make it (relatively) easy to get a shot, and get it safely, if you’re at high risk, and charge a fee in annoyance to those not at as high a risk who want a relatively early shot. So those who are actually high-risk in a less legible way, or who highly value the shot, can mostly get one, and those who are mostly indifferent can wait while others pave the way. Best of all, the annoyance of going to a worse vaccination site is a built-in cost rather than a wasteful tax, so it’s even efficient. Bravo, I suppose.
That doesn’t mean the system doesn’t sometimes fail people when they need it most. It absolutely does:
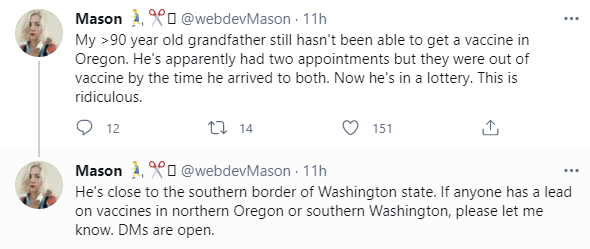
I do think that particular case is mostly extraordinarily poor luck, but it still happens. Presumably in this particular case help is already on the way, but likely still worth DMing her if you have a lead.
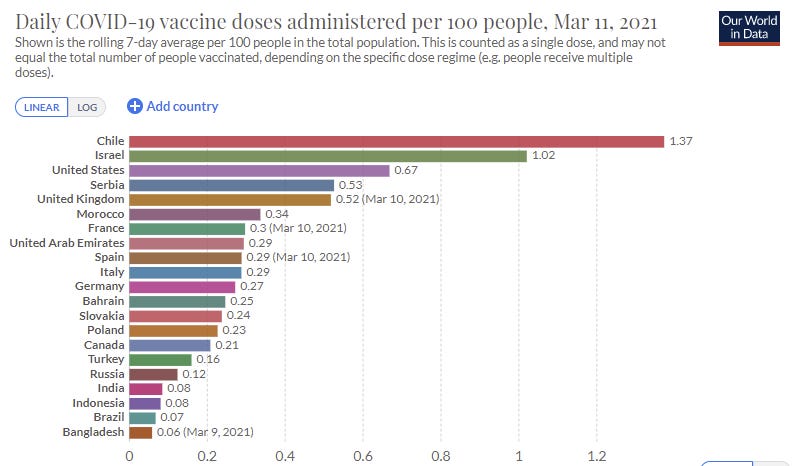
Then again, remember it could always be worse, if we grade on a curve we’re killing it here in the good old USA:
Europe
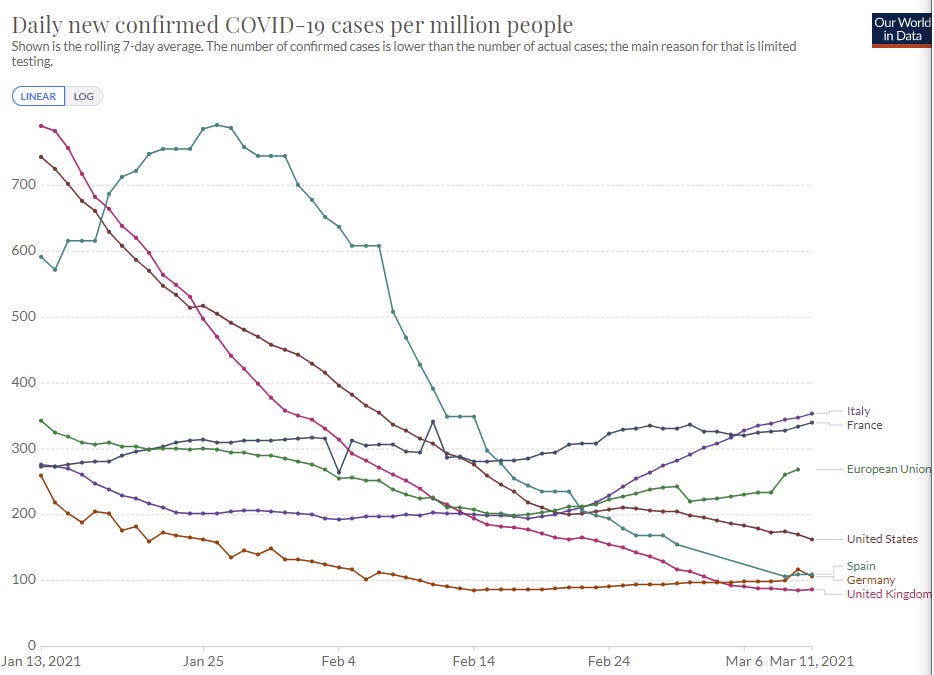
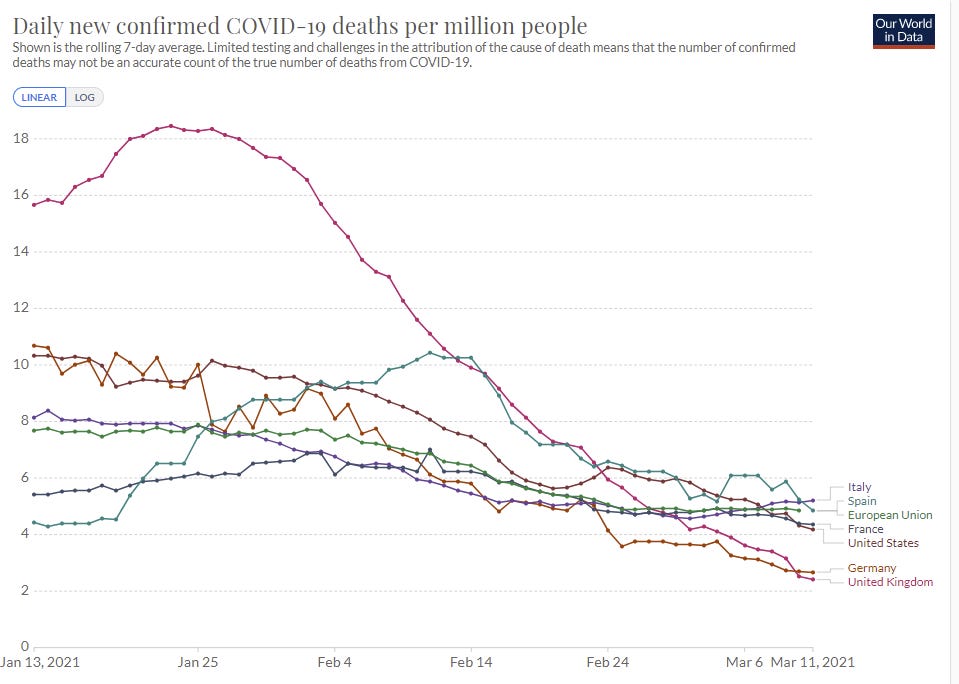
European lockdown strategies continue to have stabilized things for now but not to have improved matters much, and there are signs things are slowly getting worse rather than better. The vaccine efforts are a huge fiasco across the European Union, and should be seen as a challenge to the heart of the entire European project.
The English Strain
Oh no. New strain versus old fatality numbers from this preprint:
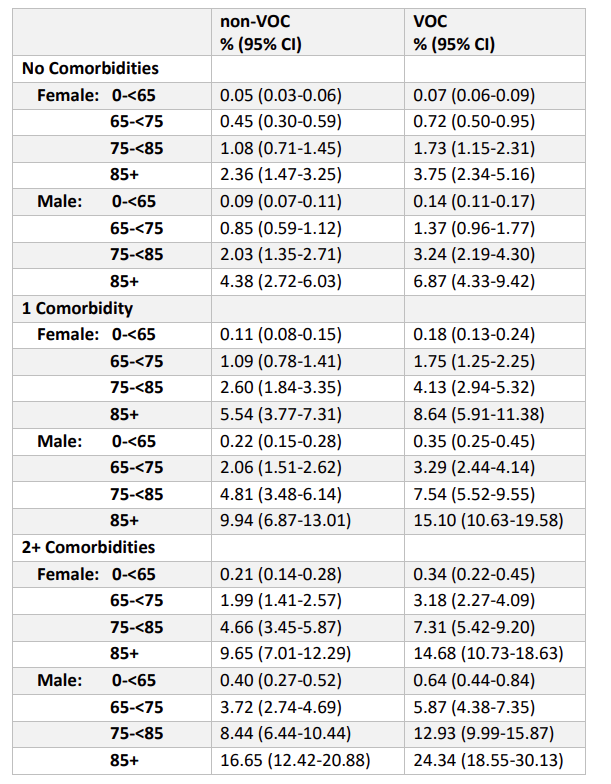
The moment will soon be here, and case numbers are already substantially higher than they would be otherwise.
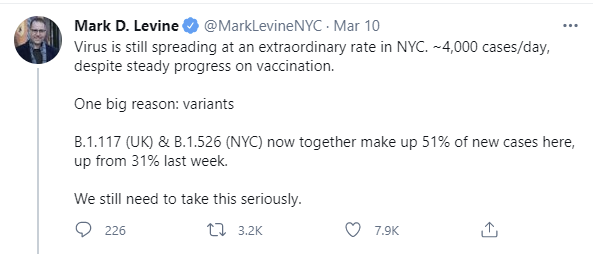
The moment of truth is fast approaching. Within a few weeks, new variants will be a majority of new Covid cases in the United States. Very soon after that, they will account for most cases.
It is clear that the number of people with the variants is continuing to rise, as the overall number of infected people is only falling slowly. It would be very surprising if the number of cases doesn’t rise before it starts dropping again - we are indeed almost certainly at least somewhat f***ed, and the resulting death rate will reflect the higher death rate from the English strain.
The question is how bad things will get. There are naively plausible mathematical models where we are rapidly vaccinating enough people to make up for the shift to the new strains. For example, there are these CDC projections which even underestimated the rate of vaccinations:

The problem with that model is that it fails to include a control system, and the control system is going to spend a while making things worse rather than better.
Open Sesame
You can say things like this all you want, but all it will likely do is backfire because it will be seen as a completely unrealistic and unreasonable demand:

That’s pretty unreasonable! When those who always make demands in a direction make completely unreasonable demands - no loosening of restrictions of any kind for a very long time - the response is to go ‘yeah, that’s public health experts for you’ and that’s that.
That’s what happened.
Not to be outdone or even matched, here’s Texas:
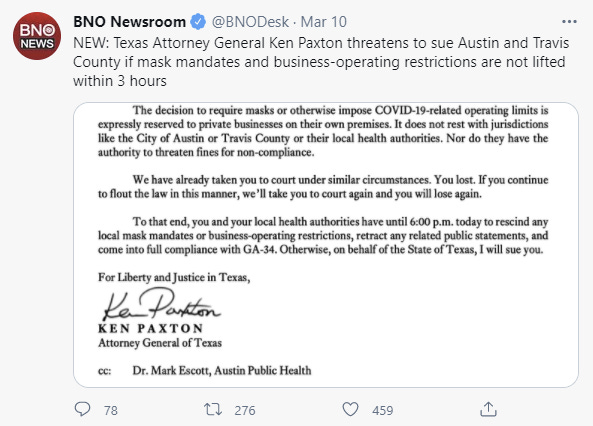
Everywhere, we see states lifting restrictions in response to the progress we’ve made. All the vaccinated people that will start acting reasonably, especially now that the CDC has offered guidelines, will likely weaken the ability to enforce norms on the unvaccinated. We’ve already seen our rate of progress dramatically slowed before the impact of a number of rules being loosened, and it’s not clear that those loosenings can be easily reversed, or if they can be reversed before things get back to alarming measured (and thus delayed) levels first, and then are implemented with a delay.
If public health advocates had wanted a different result, they could have offered a reasonable policy backed by object-level logic. I’d suggest something like this: The new strains are taking over. We have to survive one last spike due to the new strains. If a month or more from now, cases are falling and are at or below current levels, you can start loosening restrictions then. That gives people hope and is clearly reasonable, while covering the issues we need to actually worry about. Yes, they might prefer waiting longer than that, but it aint gonna happen.
In Soviet America, Vaccines Still Work But Can You?
What can you safely do if you are vaccinated?
For a long time, Very Serious People have told us that the answer is exactly the same as what unvaccinated people can safely do, all but saying “If I were you I’d lock my doors and windows and never ever ever ever leave my house again.”
This was neither a realistic ask nor a way to get people excited about getting vaccinated. It’s the same problem as telling states they can never open, except even more obviously untenable. Weeks went by, and the CDC issued no guidance on what vaccinated people could do. Thus, this was the situation as late as March 5:
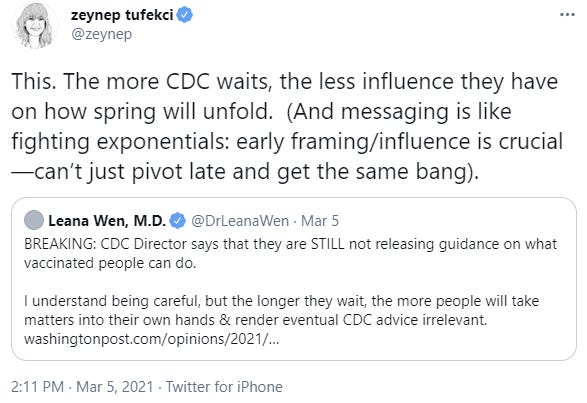
Then, finally, we got guidelines! Real ones that made a non-zero amount of sense! Nice.
That doesn’t mean we got there for the right reasons, and I definitely agree with this take.
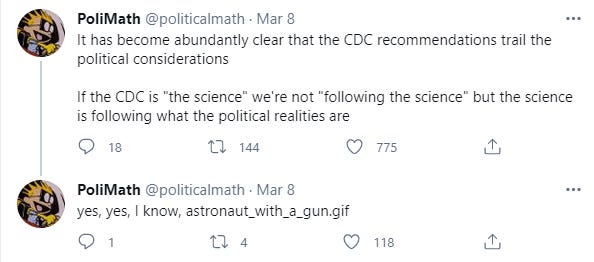
And also, while we’re on PoliMath, this take as well, even more strongly:
Then again, if they did the other thing they would never be following the science, they’d be (Following Science™)™, which is what they do most of the time and what leads to telling everyone that they should build their lives around minimal symbolic improvements in protection against infectious diseases rather than living life. I’d much rather this follow the political realities if it can be combined, as it was here, with an attempt to get the priority order of interventions into a reasonable state. Also, if you are
(Following Science™)™ and make impossible demands, even the politicians ignore you, as we’re seeing with the reopenings.
As a reminder, the key for us to remember is that the political considerations center around blame avoidance on a two week time horizon, so if we want to get sensible policy, what we need to do is create sufficient expectation of back propagation of consequences that blame can be inflicted for bad decisions (or lack of good decisions) within that two week window. Then we’ve got something.
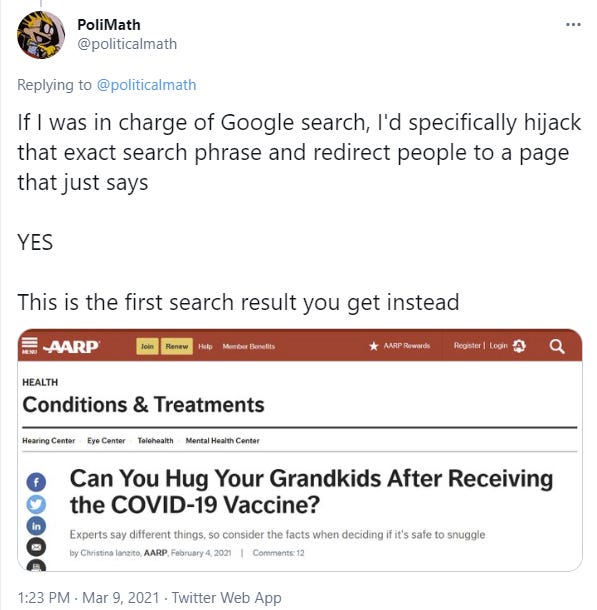
Due to the intensity of the current blame avoidance and conform-to-authority pressures, people who would usually have treated CDC guidelines as an upper bound beyond which you get diagnosed with obsessive-compulsive disorder are now taking them literally, for example:
Yeah, that’s slightly unfair because homes have some self-limiting dynamics and offices can get very large with lots of people, but the ones who are thinking that only authorities can determine who does and does not have dark transmission magic are the problem here. Or rather, the dynamics training and forcing people into the posture that they must look to the relevant authorities for currently believed locations of dark transmission magic one would be blameworthy for not avoiding.
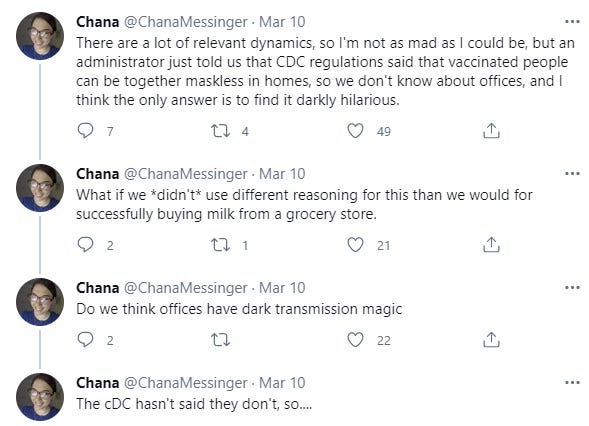
Also Robin Hanson points out that the authorities continue to treat people who have previously been infected as if they aren’t immune and this in no way counts, presumably because “no evidence.”
I don’t share his ‘they don’t much care about the infected’ conclusion, or rather I find it imprecise. They mostly don’t care about anyone, so why should the infected be an exception? Also, a lot of this is burning down the village because it isn’t legible. They’re likely thinking a lot of people think they have had it when they didn’t, and they don’t want to open up the can of worms that involves, and they want everyone to get vaccinated and to provide as many incentives towards that as possible, so better to pretend the whole thing doesn’t exist.
CDC Guidelines “Key Points”
Here is the CDC brief on the new guidelines.

So before we move on to the guideline details let’s look at these Key Points. And remember, this is their introductory explanation everyone is praising, for what everyone says are the pretty good, reasonable guidelines.
First one is good.
Then we learn that the vaccines may provide some protection against a variety of strains. However, reduced efficacy has been observed for the B.1.351 strain.
Saying that something may provide some protection is saying almost exactly nothing. It’s saying that we haven’t proven that it doesn’t provide any protection. It’s the kind of language one wants to use if one wants to avoid blame for claiming something worked, while also avoiding blame for not saying something worked, and also give the impression it likely doesn’t work.
So not only does this offer basically no confidence that the vaccines work against B.1.1.7, where we know they flat out fully work, it then says that one should be even more skeptical than the level of “may offer some protection” for this additional strain.
Next, we see that ‘a growing body of evidence suggests’ that fully vaccinated people are ‘less likely to have asymptomatic infection.’ But then it warns us the investigation is ongoing.
So we have something suggestive that they might be less likely, but who knows, these things are tricky, and no suggestion of things like ‘dramatically less’ or ‘prevents almost all’ or anything like that. Are we trying to prevent vaccinations here?
Next we are told that ‘modeling studies’ tell us that masks continue to be important, but that they generously will allow resumption of ‘some low-risk activities.’ I think this could be better summarized as ‘f*** you’ and also it seems modeling can be used to require precautions but a completely different standard of evidence applies to claims of prevention. It’s almost like it’s all about something else entirely.
Then they say ‘Taking steps towards relaxing certain measures for vaccinated persons may help improve Covid-19 vaccine acceptance and uptake.’ No s***, sherlock. Thank you for pointing this out, took you long enough. Also would help if you told people vaccines actually, what’s the word for it, worked.
The next line essentially says “ordinarily we’d tell you to lock your doors and windows and never ever ever leave your house again and actually that’s mostly what our guidelines say elsewhere if you look carefully, but we’ve driven half the population crazy so maybe we can reach a little bit of compromise this one time.” But it wants us to know that if there wasn’t a particular medical issue called ‘social isolation’ they wouldn’t let us meddling kids get away with being in the same room together.
As a side note: The CDC guidelines for gyms call for “consistent and correct mask use.” I have at various times used gyms, but it would never occur to me to use them during a pandemic until after I’d been vaccinated. The whole point of going is to improve your health, and there are plenty of other options. Also, the whole mask issue, which is going to interfere with exercising properly. It’s a small cost in many contexts, but not in this one. If vaccinated people still have to wear masks at the gym no matter the level of distancing, this seems a lot like a soft ban on gyms extended indefinitely. Perhaps we simply can’t hope to enforce a ‘vaccinated people can unmask’ norm in any public space properly, and we can mostly live with gyms being (more than usual levels of) terrible for another few months. The few true gym rats can get home equipment and/or are healthy enough that they can deal with the masks, I suppose.
All right, fine, yes, that’s not the part people are focused on and no one reads such words as if they mean things. I get it. Let’s see the actual guidelines for vaccinated people. The part that actually matters.
CDC Guidelines For Fully Vaccinated People
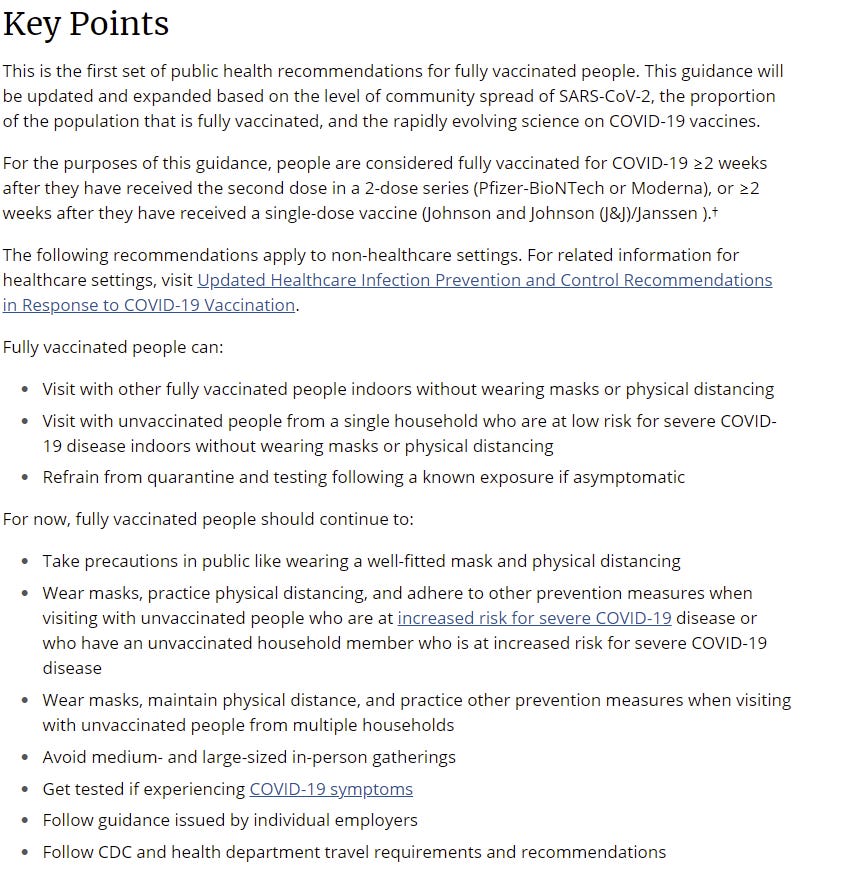
This is the part that matters so let’s see the details.
The first line is that if everyone involved is vaccinated fully, you can do whatever you want, at least for small size gatherings. Good. Excellent. Some common sense. Yes.
The second is the principle that, essentially, a vaccinated person is not a person with regard to gatherings so long as everyone exposed is low-risk.
Thus, you get one household with unvaccinated people, since that’s happening anyway, and if no one is high risk you can add any number of vaccinated people to the mix up to the limit of a ‘small gathering'.’ Good. Excellent. Some common sense. Yes.
That approval assumes a common sense evaluation of what ‘high risk’ and ‘low risk’ mean. It’s one thing to be cautious around the truly vulnerable, it’s another to look at the technical ‘list of high risk conditions.’ The orders of magnitude in no way match. If we treat ‘low-risk’ as basically ‘under the age of 65’ I think this is conservative but at least somewhat sane.
Note that this guideline is contradicted by the guideline that one must wear masks when in the presence of someone whose household includes a high risk member. That’s another degree of separation, and increases the effective annoyance level substantially if it trumps the permissive rule. It makes sense if one appreciates how the risk multiplications work, and you adjust the barrier for ‘high risk’ accordingly.
The third line is that vaccinated people need not quarantine. Again, yes. I could see asking them to act like unvaccinated persons during what would otherwise be a quarantine period, or otherwise use higher precaution levels, but for guideline purposes telling them to ignore it is likely even better. People with common sense will scale back on exposing others anyway if it looks like they took a big risk.
Then there’s the whole ‘you still have to follow every other rule same as everyone else’ clauses. Still getting tested makes sense, although presumably the bar for what counts as symptoms would go up. Following employer guidelines and CDC recommendations is something you gotta say.
Avoiding medium and large size gatherings seems overly broad, depending on what counts as medium versus small. If the concern is that medium gatherings of vaccinated people are actually risky, I think that’s mostly silly. If the concern is that people who aren’t vaccinated will come anyway, or this will normalize larger gatherings and we want to hold off on that, those reasons seem reasonable. Given how vague medium is, I’ll allow it.
Wearing masks when visiting with multiple other households is rather hilarious if you break down what is happening. It’s norm enforcement with a side of punishment. The CDC does not want multiple households of unvaccinated people meeting up, for obvious reasons, and wants to at least ensure mask compliance, so it’s not about to give anyone vaccinated permission to take off their masks in such a room. And I get that. Once anyone at a gathering takes their mask off, there’s a strong tendency for everyone else to take theirs off as well (or to tell them to put it back on). If everyone isn’t in it together, no one wants to be the schmuck going through the annoyance of wearing the mask.
Overall, these guidelines do seem reasonable, as a compromise between what makes physical sense and what preserve necessary norms of behavior, and as a compromise between encouraging vaccination versus letting risk get too out of hand. That doesn’t mean they need to be followed to the letter, but we could have done a lot worse, and this is far better than no guidelines at all, and far better than the previous FUD of ‘act the same as before.’
So yeah, all in all, I’ll take it.
Vaccines Only Work If You Use Them
AstraZeneca remains unapproved.
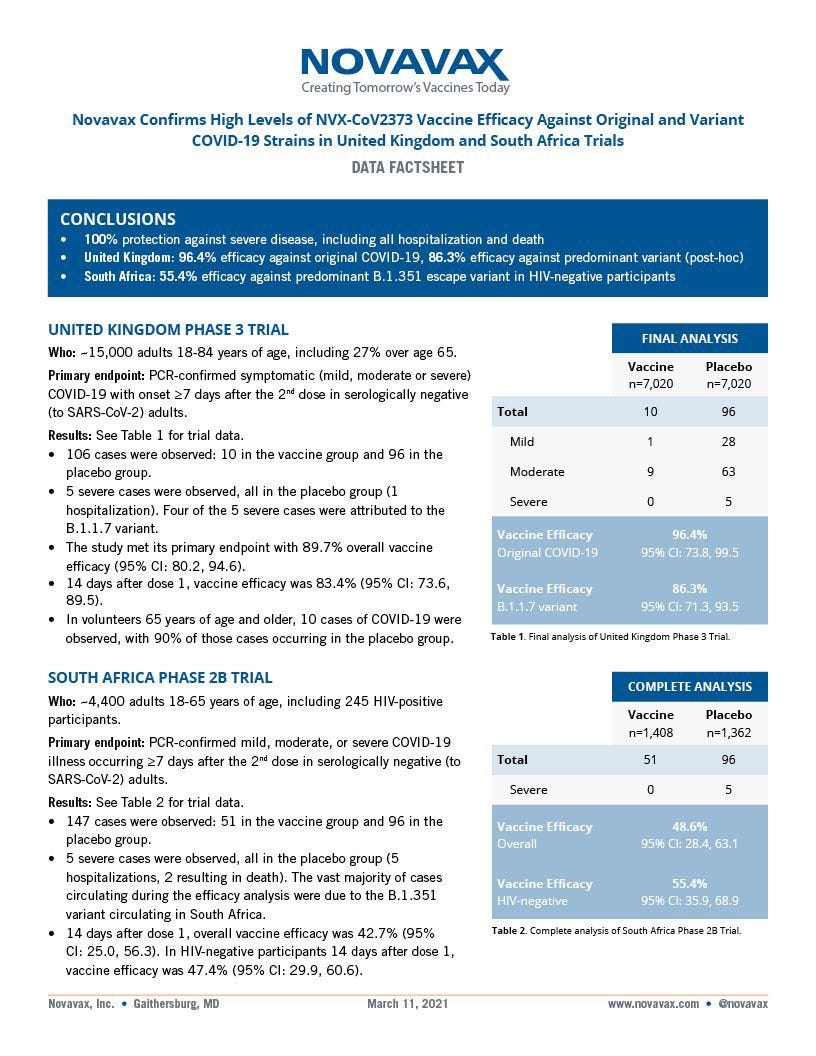
Novavax remains unapproved, and has new results (press release):

Johnson & Johnson did get approved but after several weeks of pointless delay and with still essentially no plan, after all the complaining about the previous administration’s lack of planning, so here’s what we got there:

Here’s a Bloomberg article (behind a paywall) describing what happened.
There’s nothing much left to say at this point, other than in a real sense #YouHadOneJob applies to all of this, and if you can’t do it, you’re a failure, period.
On another vaccine policy front, MR gives your periodic reminder that dose stretching (also known as vaccinating more people) reduces risk, and this includes mutation risk for obvious ‘shut up and multiply’ reasons.
On Lying
I am in general strongly against lying. Even when dealing with people or institutions who lie to you, who are mostly against you, who are not to be trusted, I still believe it is usually best to not lie.
There are limits and exceptions. Some people and systems flat out refuse to accept not lying, and some of those aren’t things one can reasonably avoid, often gating vital resources behind lying, or otherwise imposing very large costs to not lying. They train people to lie and reward liars, and punish those unwilling to lie or who endure costs when forced to tell lies, and generate norms that lying is The Way Things Are Done, and is justified and to be expected.
If one wishes to cultivate virtues like honesty, justice and honor, what is one to do? Where do we draw the line?
There’s no clear answer, but I think this is clearly one of those cases:

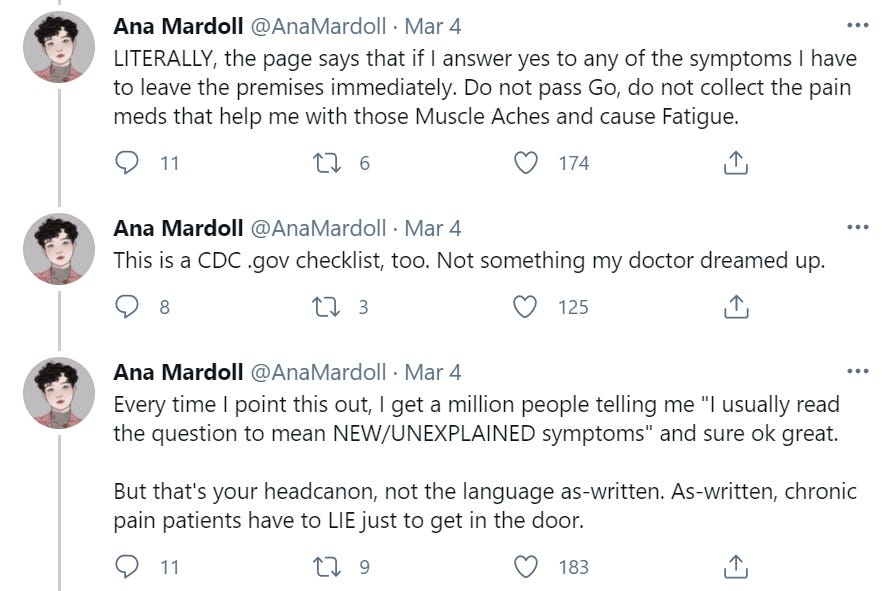
I understand what the people designing the checklist were thinking. The first half of their thinking, that we need a checklist of questions to see if anyone has symptoms, makes perfect sense. Good thinking there. The problem is the other half where they implicitly assume that everybody knows that words do not have meaning and that everyone knows to lie about the questions when it would be pragmatic to lie.
There are several problems with this approach.
One is that once people realize ‘oh, clearly they don’t think their words to be taken literally’ then everyone makes their own determination of what things to mention and what things are none of anyone’s damn business, perhaps because they want to not be shown the door out of the building. Then there’s that to normalize that anywhere is to normalize it anywhere. We’re teaching that words are not supposed to have meaning, that we shouldn’t put necessary qualifiers on statements.
Then again, that could all be wrong. I am not at all convinced that the head cannon that it’s ‘new/unexplained’ symptoms is actually the intention at all. If you give people that kind of wiggle room, a lot of them will think ‘oh, sure, I can explain that’ and pretend everything’s fine when everything is very much not fine, and also there’s constant pressure on everyone to not be socially awkward, so you kind of need hard and fast rules to avoid disaster. Which people will then of course lie about, once they realize how this works.
Presumably the solution is to ask the question, then if someone says yes to check if it’s chronic or otherwise explained before escorting them automatically out of the building, or at least to say ‘non-chronic’ or ‘new’ or something. I would actually want to avoid ‘explained’ here and at most let a follow-up determine what counts as explained.
If You Aren’t At High Risk, Should You Get The Vaccine Yet?
The trickier moral dilemma is the vaccine.
If you are at actually high risk and are eligible for the shot, yes, 100%, you should absolutely get the vaccine as soon as possible.
The questions worth asking are, should you be willing to lie to get the vaccine? Should you get it while there are others who are high risk, even if you can get it without lying?
I’ll take the second question first. If you are legally eligible and can get the vaccine without lying, I say yes, 100%, you should absolutely get the vaccine as soon as possible.
This is rather overdetermined.
Authorities explicitly want you to do this, and I want you to do this as well, because the most important thing is getting shots into arms and not letting shots sit on shelves, and we’ve set up alternative methods to help the most vulnerable via pharmacies and also the best way to protect most of the remaining most vulnerable is to get as many people as possible vaccinated.
On the margin, if you don’t book an appointment, either the appointment and shot you decline will go unfilled, or it will probably go to someone else who is ‘high risk’ according to some list but unlikely to be actually high risk, or someone who is lying. In many jurisdictions all you have to do is say you are somehow eligible. That’s it. No one is verifying anyone’s claims.
If there’s someone in contact with you refusing to claim a shot they are eligible for on these grounds, and this is exposing you or those around you to covid risk, I think it is correct to be rather upset about this. It’s not a reasonable concern.
The real question and least convenient world is, suppose (because this is the case in at least many places) that the law is inefficient, unjust and unenforced and none of that is an accident. For example, suppose there’s a giant list of ‘high risk conditions’ that qualify people, including ever having smoked a few cigarettes, or having a ‘developmental disorder’ which explicitly includes your motherf***ing Tourettes (which can also get you medical weed). And it’s clear that they never actually ask for any kind of verification - in Washington DC they literally just ask ‘do you have one of these 20 things?’ and all you have to do is say yes. Press X to not die.
It is valuable and important to cultivate the virtue of not lying, but at some point this isn’t even lying anymore because you are dealing with the words of actors rather than scribes and the actual meaning of your words is the pure and truthful ‘I want to get vaccinated.’
How meaningfully different is all this from a box that says “I want this vaccine”? How meaningfully different is this box from the box that says ‘I have carefully reviewed the 40 page user agreement?’
Did you pack your own bags?
Then there’s the question of Prizer’s CEO, who it seems is not vaccinated, and this forced him to postpone a trip to Israel. Presumably the PR department decided that it would be a bad look to ‘skip the line.’ My suspicion is he’s actually vaccinated but is pretending he isn’t and he can’t tell the Israelis that.
Not only should he be vaccinated, he should have been the first person vaccinated. That’s basic Skin In The Game 101. The person in charge of making the vaccine takes the vaccine. Instead, we’re so concerned about perceptions of ‘line jumping’ that the person who literally led the vaccine development effort doesn’t feel entitled to publicly claim a dose for himself, let alone feel under his proper obligation to take a dose (that would also benefit him, but the point is that he proves that he believes this and we can know that.)
Similarly, a better vaccine approval system (for the first vaccine, anyway) might be that everyone at the FDA decides secretly when to get themselves and their families vaccinated, entirely up to them, and when enough of them decide to do it, the vaccine is approved. You can have any meetings you want, but they don’t count for anything. Ideally you’d hold some people out-of-sample so you could do this for other vaccine candidates later.
Who Wants the Vaccine?
The above section assumes that if you’re reading this, you’re aware that vaccines are the greatest thing and the only question is how to get one.
Alas, this is far from a universal perspective. Here’s current survey data, and some more:

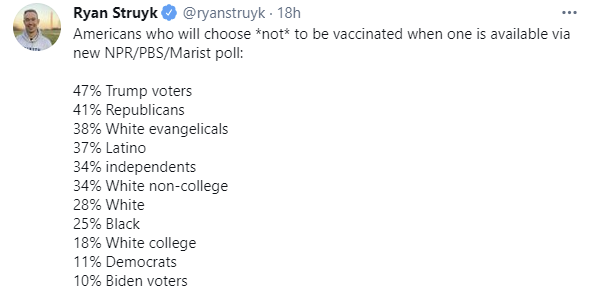
The six point gap between Republicans and Trump voters makes the role of tribal identity here very clear.
I wonder several things. First, I wonder how much the ‘wait and see’ category is mostly ‘I don’t want to have to think ever and this is an excuse not to for now’ because most of those people aren’t yet eligible. They know they don’t want to think enough to look over a list of conditions and figure out how to get an appointment, so why think about something now when they can at worst have to think about it later, and hopefully by then the answer is obvious?
The group that says ‘get only if required’ feels like it has to be way bigger than that. Are the majority of people who aren’t in the first two categories really going to give up their job or place in school rather than get the shot? That’s a super strong preference to not take the vaccine. I am super excited for the vaccine but would I quit my job or drop out of school to avoid it under a normal person’s life circumstances? No, I would not. I’m guessing most of this is all talk.
There’s also the question of blame and social pressure, because it seems (standard warning about anecdotes) like there’s a lot of this:
Mostly people deciding about vaccines aren’t basing their decision on physical world models and a study of immunology and statistical findings. They’re responding to various forms of social pressure and information cascades and blame dynamics. For various reasons there’s a bunch of ‘vaccination bad’ social pressure in many places, so my model says that such folks will mostly reverse when the forces going the other way are sufficiently strong that the social pressure has to back off, and such folks aren’t realizing that the pressure from other sources will relieve the social pressure when the time comes. If you can’t (hold a job / go to school / travel / go to a restaurant / etc) without vaccination, they’re gonna fold and they know it, but for now their social rewards are for putting up a front that they’re not going to get vaccinated, so that carries over to the survey because there’s no incentive to be super-honest and self-aware.
I continue to be rather baffled by the whole ‘wait and see’ attitude, unless it’s another case of avoiding blame and social pressure, in this case by avoiding taking a position, and doesn’t cash out to anything at all. What are we waiting to see, at this point? We’ve given about 100 million doses in the United States and everything’s going great so literally what do these people worry they are going to see? Is it basically this?

Seems like it would have to be, except without as plausible a mechanism as that one.
So I guess that means it’s time to address the whole blood clot thing...
AstraZeneca and Blood Clots
Even by 2020-2021 pandemic standards this one seems beyond ridiculous.
Several places, including Denmark and Thailand, have suspended use of the AstraZeneca vaccine due to concerns about blood clots. There have been voices of panic, warning that if this turned out to be a real thing that it could destroy public confidence in all vaccines, perhaps for all time.
I did not have to look to know this was almost certainly Obvious Nonsense, because it looked nothing like what the response would be if it wasn’t Obvious Nonsense.
And also because blood clots on this scale are somewhat more plausible an issue than being struck by lightning more often, but not that much more plausible.
And also because math. If there was a blood clot issue big enough to make the AstraZeneca vaccine potentially not worth using, either it comes along only after a several month delay and then suddenly happens to tons of people, or we somehow missed it for several months under mass vaccination drives. Thus, until I got back home I didn’t bother checking for data.
Then, of course, I saw this from the BBC:


Here’s the BMJ confirming that investigations show zero signs of a statistical effect of any kind. Even if somehow there was some small effect, the chance of this being big enough to justify not using the vaccine is very, very close to actual zero.
I love this post by Nate Silver...
...because, while there are a lot of previously existing real consequences and they’re really terrible (and thus that part of it is really weird), the implicit assumption here is that none of this has anything to do with an actual problem with the vaccine and that no one even thinks anyone else actually doubts seriously this. There’s common knowledge that the concerns are stupid.
The amount of damage done to vaccine efforts due to the suspensions and beyond catastrophic messaging and failure to do any math at all, both by suspending them directly and by making everyone around the world have one more reason to worry, is rather large here.
I wonder how many people didn’t get laser eye surgery due to the throwaway Ned Flanders joke on The Simpsons. I’m guessing more than one might think. I know that I was for a time under some social pressure to get it, but I didn’t want to, and the throwaway joke gave me some ammo to push back. Then compare that to this.
We Have Established as Common Knowledge That Andrew Cuomo Is The Worst
Andrew Cuomo has been The Worst for a long, long time. I have it on very good authority that he got his start cruelly bullying his brother Chris in early childhood, kept going from there, and Mario Cuomo should be viewed in many of the same ways we might think of Marcus Aurelius - you can be a great leader while you’re alive, but all is lost if you botch the line of succession.
For those following the actual underlying scandal and cover-up, there’s this: Cuomo administration altered a Covid report, intentionally omitting the true magnitude of Covid’s impact on nursing homes. (HT/Source, administration response that their cover-up was sufficiently badly implemented that it was legitimate).

It’s worth noting also that the inappropriate workplace behavior is looking worse and worse, as there’s more and more accusers and the things he is accused of get worse and worse. By any reasonable standard yes he should definitely go down for the sexual harassment if it wasn’t for the fact that he very much needs far more to go down for the directly caused mass deaths and cover up of the mass deaths and it’s hard to truly go down for multiple things at once.
So basically this (and you gotta love the photo):

At first it was plausible to claim the sexual harassment accusations were some combination of false or not that serious. That no longer seems plausible.
What seems clear is that, if it wasn’t for the nursing home situation, Cuomo wouldn’t be facing any of these accusations, would likely never have faced them, and he would have continued to get away with lots of sexual harassment.
All the revelations are entirely unsurprising. What would have been surprising would have been if Cuomo wasn’t engaging in and getting away with lots of sexual harassment, because the prior on such behaviors by men with power is rather high, and Cuomo is a mean petty tyrant and bully and a liar - remember, he’s the worst - so to have his behavior in this other realm suddenly be appropriate and reasonable would have required an explanation. Then, once his grip on power had sufficiently slipped and things turned against him, things turned against him and others amplified and encouraged reports of his actions rather than discouraging and suppressing them, and others (including the victims) suddenly interpreted his actions as unwelcome and offensive rather than maximally permissible.
And now essentially every Democratic politician in New York is lining up to call for his resignation.
I do find the dynamics here interesting in a broader sense, but this is already dangerously deep into ‘there be dragons’ territory and I’m only going here because it’s Cuomo, so let’s move any further discussion to a different venue more appropriate to such issues.
And Yet, No, Technically We Are Incorrect, Eric Topol Is Actually The Worst
Beware scope insensitivity! For it seems likely Eric Topol did this:

No, seriously, it looks like he did that. Thread. See the MIT link for more details.
If this actually made a difference, the amount of blood on this man’s hands is staggering. Not history’s greatest villain, but we should not be confident he doesn’t make the list.
From The Drunkwriting Files of Polimath: A Short Dramatic Scene Within the CDC
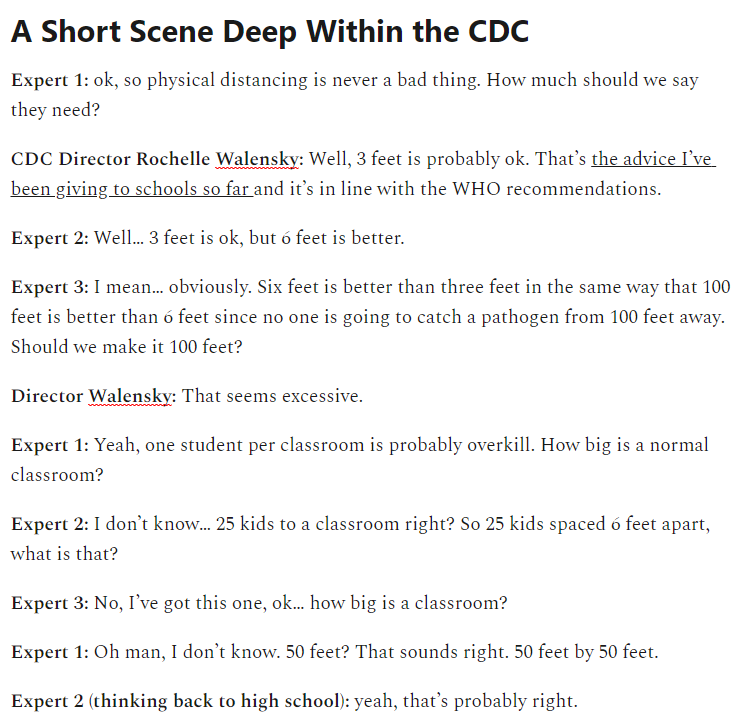
Seems legit. Tacos are great.
In Other News
France is going to start vaccinating on weekends.
Report from WSJ that P.1, the new Brazillian variant, is really dangerous (WSJ link).
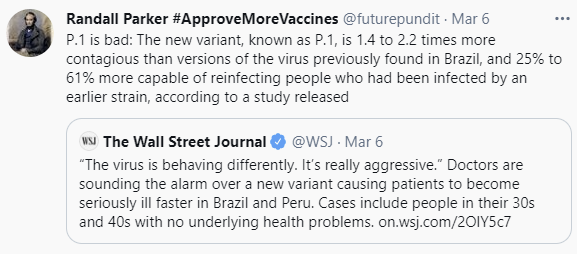
I haven’t seen talk elsewhere and haven’t had an opportunity to follow up on this. These numbers even if accurate are definitely something vaccination can overcome if we have enough time, which we likely do if this hasn’t arrived here yet. The highlighting of ‘cases include people in their 30s and 40s with no underlying conditions’ highlights that this is clueless journalism where wet ground causes rain, so I’ll hold off on updating much until more information is available.
Goodbye what-to-do-now thread from Covid Tracking Project, alas not that helpful. Links to data summary and a guide to federal resources.
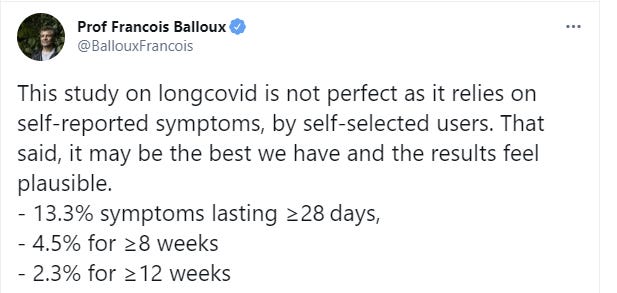
New nature study on long Covid (paper). As he says, it’s not great, but the alternative data points seem even worse.
Alex Tabarrok reports that the condition of his students is increasingly dire.
California variant seems unlikely to be important.
CDC study on Covid and obesity.
Australian doctors are uncertain in what ways they can legally promote vaccinations due to anti-drug-advertising laws. MR chimes in and reminds us that England banned mask advertising.
A modest proposal on price gouging.
CDC still, today, discouraging use of N95 masks because of supply concerns. Delenda est.
Our vaccine messaging is so terrible that the mayor of Detroit turned down an allocation of J&J vaccine doses, so his city’s residents can ‘get the best.’ As far as I know, he remains the mayor.
Twitter thread of examples of ‘public health experts’ calling for kids to return to school.
If you’re finally going to vaccinate around the clock, why not give it an ‘80s theme?
Doing a randomized oncology trial means overcoming 50+ people with veto power over several steps. There is indeed likely someone you forgot to ask.
From LessWrong: A tool called MetaForecast that is Exactly What It Says On the Tin. I don’t find such things that useful right now but this seems much better than trying to find the data elsewhere.
Facebook is censoring doctors writing in the Wall Street Journal on grounds of ‘misleading information.’ As Gu points out in his thread, this sets a highly dangerous precedent and the procedure being used to decide what to censor makes no sense and is fully arbitrary. It would be entirely unsurprising if links to this column were to be censored by Facebook. Please do not rely on them as a source of news, or ideally for anything at all.
Next week I plan to return to the Thursday cycle of posting.