

Covid 5/6: Vaccine Patent Suspension

The Biden administration’s latest strategy for the pandemic is to suspend the vaccine patents without compensation. Our life expectancies are lower than they were last week.
It’s a shame. I like the idea of rewarding those who do amazing things for myself and for the world. I like people out there knowing that if they produce amazing things for myself and for the world, they would get rewarded for them. I like the idea of not dying for as long as possible thanks to future developments in medical science. I like being a nation of laws, where the executive doesn’t just take stuff when he feels like it. And I’d like, when nice things are taken away and we mortgage our future, to at least get something out of the exchange.
Alas, the man in charge does not agree, and the government was not content with its previous efforts to sabotage the vaccination effort. That’s how it goes sometimes. You can’t always get what you want. Nor, when no one is given the incentive to produce what you need, are you likely to get that either.
Let's run the numbers.
The Numbers
Predictions
Prediction from last week: Positivity rate of 3.9% (down 0.5%) and deaths decline by 6%.
Result:

Nailed the positivity rate. Johns Hopkins has us down from 3.9% to an all-time low of 3.6%. Deaths rising makes no physical sense and the move up doesn’t show up in the Wikipedia data, so this has to be a data fluctuation one way or another. I’m going to guess that it will revert.
Prediction for next week: Positivity rate of 3.5% (down 0.4%) and deaths decline by 7%.
Deaths
DateWESTMIDWESTSOUTHNORTHEASTTOTALMar 25-Mar 311445976256412626247Apr 1-Apr 71098867178911604914Apr 8-Apr 1410701037162111454873Apr 15-Apr 21883987174711684785Apr 22-Apr 287521173160911104644Apr 29-May 5943122014409714574

The bump up in the West comes from California, which makes it harder to dig in deeply. The bump in the Midwest is more curious, but should reverse soon. Overall we see a disappointingly small decline, but still a decline, and it should pick up speed.
Cases
DateWESTMIDWESTSOUTHNORTHEASTMar 18-Mar 2447,92172,81099,568127,421Mar 25-Mar 3149,66993,690102,134145,933Apr 1-Apr 752,891112,84898,390140,739Apr 8-Apr 1460,693124,161110,995137,213Apr 15-Apr 2154,778107,700110,160119,542Apr 22-Apr 2854,88788,97397,48278,442Apr 29-May 552,98478,77885,64168,299

Progress in the West remains slow, but improvement in all regions, with many states seeing large declines. We didn’t sustain the giant improvement rate in the Northeast but we still see pretty great improvement. This is what the endgame looks like.
India
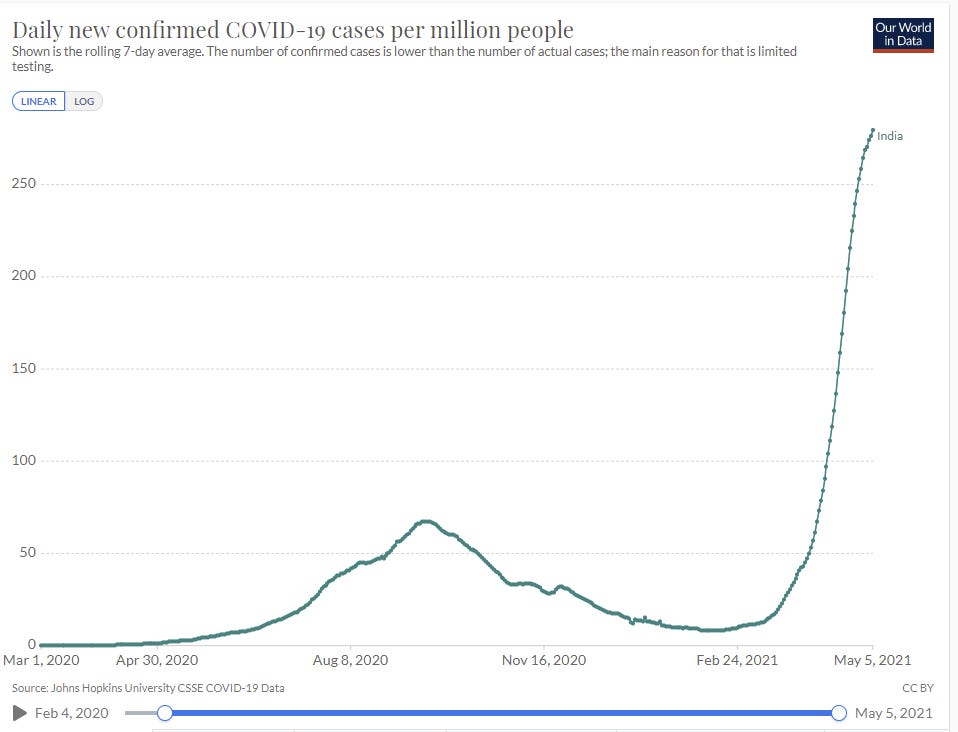

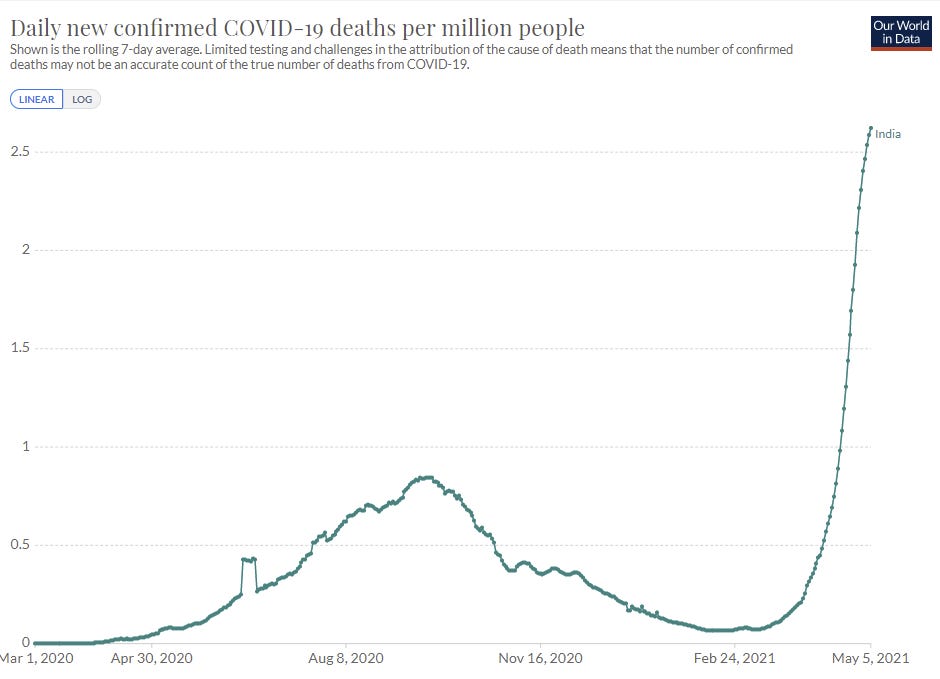
Things continue to get worse in India, but the graph no longer looks as fully vertical as it did previously, so this continues to count as good news relative to the range of possible outcomes. If things peak not too long from now, it will still be the biggest disaster of the pandemic, but it won’t be anywhere near as bad as things could have gotten.
Vaccinations
We all know how it started.
How’s it going? Keeping up the momentum?

As a reminder, we were once over 3 million doses, and we’re giving out more second doses now than we were then.

Every week, the graph of vaccinations looks more like the electoral college maps:

I found this chart enlightening when I first saw it:
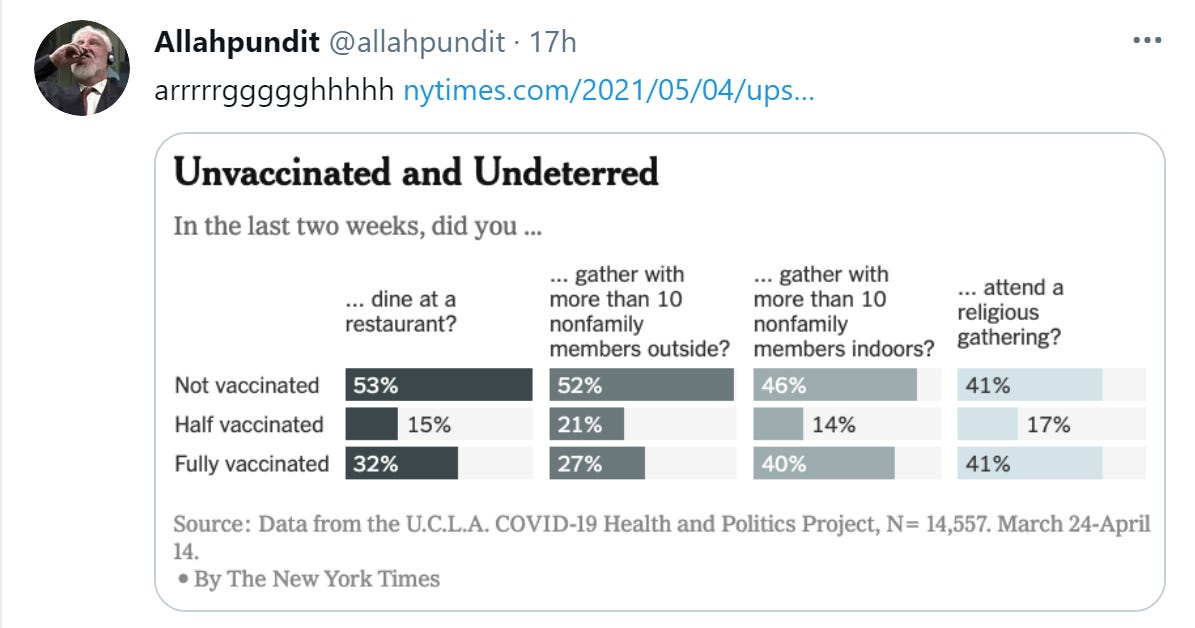
The problem is that this isn't what I thought it was. I thought it was what percent of each group did each thing. Instead, it was what percent of everyone who did the thing was in each category. That forces us to consider base rates, which makes the whole thing complicated.
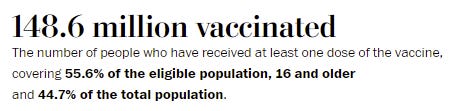
The good news is that even now only 55% or so of all adults are vaccinated, which means that people who are vaccinated are indeed doing more things. Yay!
Indian Strain Does Not Escape from Vaccines
The situation in India is terrible, but at least there is this bit of good news - the vaccines will continue to function, at least against the current strain:
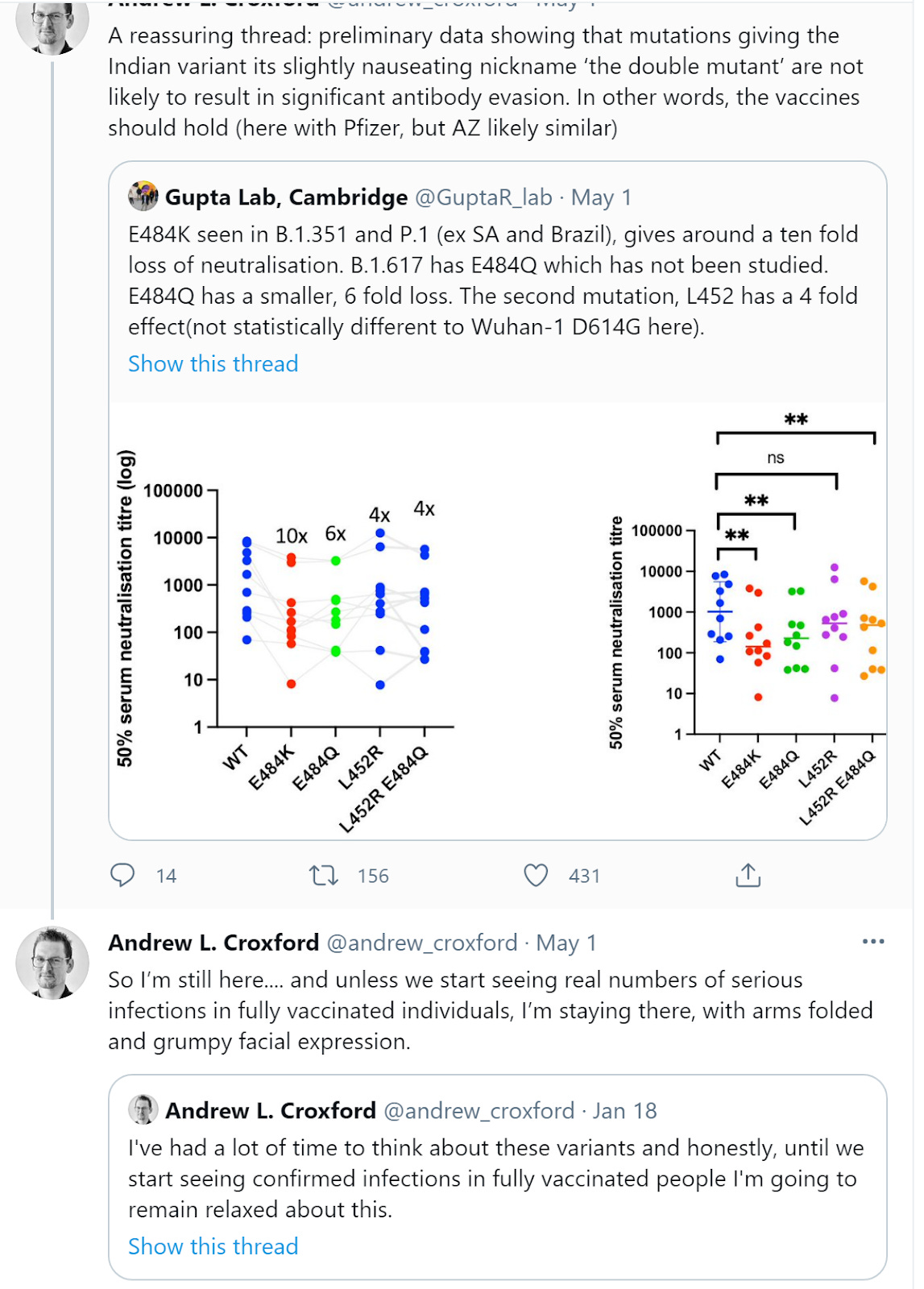

Mutations not being additive seems like very reassuring news, implying that there could be a maximum amount of infectiousness or vaccine escape that a Covid-19-type thing is capable of easily achieving. I don’t see why we would stop using the term double mutant, but it makes it a lot less scary.
If there’s one place I’m most worried about engaging in motivated reasoning, it’s the possibility of vaccine escape. I notice a much larger flinch away from looking here than I do elsewhere. I think I’ve overcome that flinch, but I could be wrong about that, and it’s a super important thing to not make an effort to avoid seeing. So while I’m confident, I want to task my readers with keeping me honest on this one even more than usual.
P.1 Is The Medium-Term Infection
In many ways it is better to think of Covid-19 as a series of different infections from different variants. When the English strain shows up, it starts again from patient zero, starts again in each nation and region, and grows. When P.1 shows up and shows it is a more fit strain yet, it does this once again.
If you’re looking at the endgame scenario, the question is whether we’re seeing an increase or decrease in the most dangerous variant’s numbers in absolute terms rather than relative to the overall number of cases. Thus, in a place like New York, the ‘real’ graph of our future situation is the graph in P.1.
This is delayed due to how long it takes to do sequencing, but it looks like this:
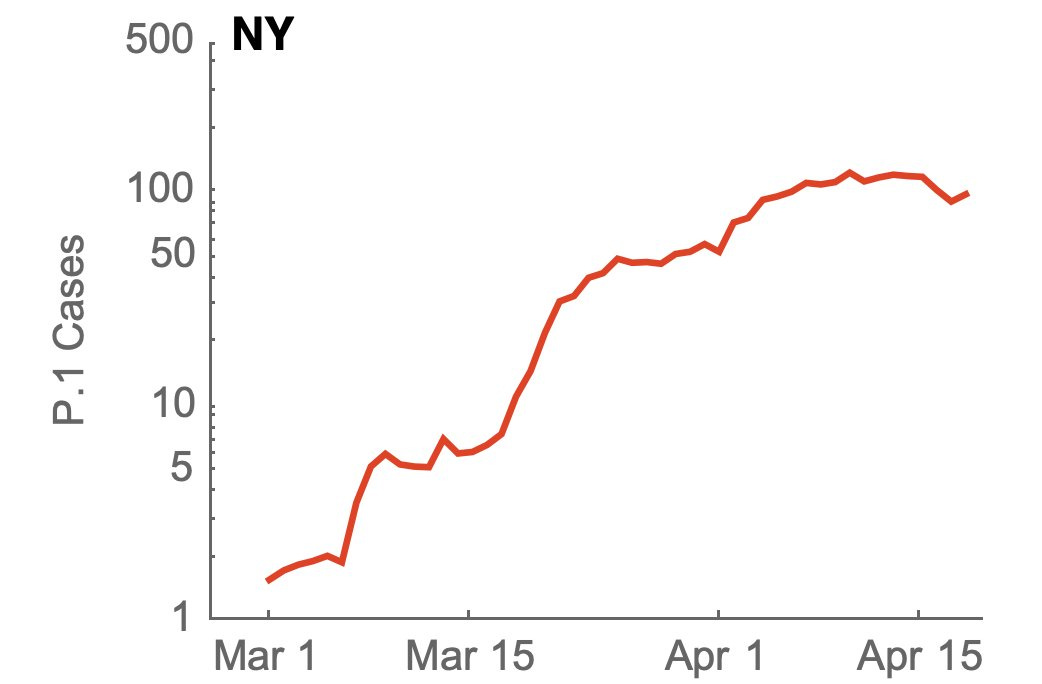
Compare that to the graph of New York City’s cases, which looks like this:

Things had stabilized for P.1 by early April, when regular cases started cratering. Now, with regular cases declining even more rapidly in percentage terms, things are clearly improving even on the P.1 front, at least somewhat. We’ve passed the next test here, not only the previous one. As additional vaccinations come fully online, things will only improve, and I expect other areas to also hit this target.
The last month has been far more impressive than it has looked on its surface. We went from mostly the old strain to mostly new strains, and we are still steadily improving overall. The news really is quite good.
I worried last week that in relatively hesitant areas, we might run out of willing arms before we get to herd immunity. That is still a real worry, but I am not worried that large other areas won’t get to New York’s current effective immunity level given how many vaccinated people aren’t yet finished being vaccinated. That doesn’t allow a safe return to normal, but it does allow suppression when combined with moderate levels of precaution from the unvaccinated. My trip to New York this week revealed a city still taking its precautions deeply seriously, despite the majority of people being post-vaccination. I was clearly taking below average amounts of precaution, which was a new experience.
Exploring Vaccine Hesitancy
As a reminder, and to avoid any possible misunderstandings, as I keep saying week after week, the vaccines are very safe and super effective.
If you’re reading this, you almost certainly know this. If you’re reading this somewhere you can get vaccinated, and you haven’t done so yet, stop reading now, go get your first shot. We’ll wait.
Not everyone, unfortunately, is in your epistemic position. Thus, we have vaccine hesitancy.
What are the real reasons for vaccine hesitancy? There are lots of theories out there, and I’m confident someone cares about any given justification one could come up with, but what are the most common true objections?
There’s a lot of plausible candidates for the most common true objection.
A survey about vaccine hesitancy in the army has some good data on this, and is worth looking at in detail. I wish the data was better and came with numbers attached, but it’s still good to have a look at the slide of the Top 12 reasons soldiers are refusing vaccinations (it’s pasted here, but it’s a lot easier to read at the link.)

Or in written list form:
It’s not FDA approved.
It hasn’t been proven safe.
What’s the point? I’d still need to wear a mask.
This is the first time I get to tell the army NO!
I am not in a high-risk population.
I already had Covid-19.
The vaccine symptoms are worse than the virus.
The virus has the same morbidity rate then the flu.
I don’t want to get my family sick.
I am being safe. It has kept me healthy so far.
The vaccine may impact my pregnancy.
I just feel skeptical and don’t know what to believe.
It’s also worth taking in the perspective of the writer of the article and of the writer of the slide. Both writesr take it as common knowledge that the reasons to not take the virus are stupid and wrong, and that the job is to fix what’s wrong with these soldiers who are refusing.
There’s no acknowledgement that maybe we’ve messed up in how we handled this whole thing, or that some of the concerns might be reasonable, or that maybe we treat our enlisted soldiers like garbage or worse and they might really, really want to tell the army where to go. It’s a volunteer army, but the recruiter can lie to you, and once you sign the contract you definitely can’t quit.
Consider this whole thing, as I will do from here, from the perspective of the hesitant soldier.
There are a few categories of objections here.
The first category (1,2,9 and 11) are the straightforward safety concerns. These concerns are wrong, but I say that as someone who knows they are wrong. And the responses suggested here other than to #9 are... not great.
The FDA didn’t approve your energy drink? How is that relevant or in the appropriate reference class? If the vaccines have undergone such a rigorous process as you say, then why hasn’t the FDA approved them?
The clinical trials were three times as large as normal? How about the one hundred million Americans who got fully vaccinated? Maybe mention that? And again, what’s your answer to the obvious: If it’s so damn safe why hasn’t the FDA fully approved it?
There aren’t any obvious problems with pregnancy? Gee, mister, that makes me feel way better. No idea why we’re voluntarily going with this weaksauce over much stronger alternative arguments. If I’m listening for bullshit, guess what I’m thinking right now?
In related news, Stat News argues that the emergency use status of the vaccines shouldn’t interfere with vaccine mandates by employers and schools. As a matter of law I think they’re probably right (although of course I Am Not a Lawyer and all that) but as a matter of practicality this is a strong argument that it’s important that the FDA needs to issue a full approval. We’ve just had the biggest Phase 4 in history. Taking at least Pfizer and Moderna from ‘emergency’ use to full approval would do a lot to reduce hesitancy and free the hands of those who want to mandate vaccinations, without being coercive.
If you want to solve this issue, the FDA should simply approve the vaccines, full stop, not simply emergency use. Problem solved.
If not, the response to a soldier should be that the FDA are a bunch of ass-covering assholes who would prefer never to actually approve anything, and maybe that would get through to them in a language they can understand.
The second category (7, 8 and 10) are claims that Covid-19 isn’t that big a deal compared to the cost of getting the vaccine.
Here we see that response #10 says both “masks and social distancing work” and then goes straight to “but they don’t ‘directly combat’ the virus” implying they don’t count. When you’re lying about everything, it’s hard to keep your lies consistent, so I guess I’m somewhat sympathetic to this local predicament, but man it’s glaring.
The answer to #7 isn’t going to convince actual anyone. The ‘mild symptoms lasting 24-72 hours’ are exactly what the soldiers are complaining about, and the response is to tell them they’re imagining things, which they most definitely aren’t. Smooth.
For #8 they quote some statistics and it seems fine, I guess, although it leaves some ammo on the table. It’s kind of bending over backwards to be maximally generous to the flu’s deadliness. I’d have gone with different wording, but mostly this one is fine.
It’s interesting when they strengthen the answer to the point of deception, and when they weaken the response to the point where it doesn’t respond to the concern.
The third category (3, 5, 6) are claims that it’s not in the soldier’s personal interest to get vaccinated, because they’re young and healthy, as most active soldiers are, so why should they get sick for several days and maybe face risks they don’t know about? This also overlaps with 7.
The response to #6 isn’t an outright lie exactly, since the word ‘may’ does a lot of work. The sun might have just exploded. But in practice, yeah, this is lying.
The response to #3 is, and I quote, “F*** you.” If you all mostly comply, we’ll lift the outdoor mask mandate? That’s your pitch?
The response to #5 is, and I quote, “F*** you.” Or, technically, ‘it’s not about you.’ It completely accepts the (incorrect) premise that the soldier doesn’t benefit, which doesn’t seem like the approach I would take.
Then there are two standalones.
There’s the remarkable #4: This is the first time I get to tell the army, NO!
And oh my is the answer to that one “F*** you.”
Which leaves #12, which is the most interesting of the responses.
That’s because the soldier has spoken The Words, and has spoken them rightly.
Rather than voice a specific and explicit concrete objection, to which the answer of necessity is going to be some combination of ‘you’re wrong’ and ‘F*** you,’ the soldier has given a general feeling of uncertainty without any concrete objection. Thus, there’s no way to say they are wrong, and no basis to curse them out.
Instead, “I just feel skeptical and don’t know what to believe” elicits this response:
“The choice to get vaccinated is a personal decision and should not be taken lightly. Talk to a medical professional, consult the FDA Factsheet, and review the educational materials available at www.carson.army.mil and from the CDC to weigh risks and benefits.”
Suddenly we’re acting like this is a Very Reasonable and Responsible Position, which needs to be solved by consulting official sources and doing further research. Only after that, when the soldier comes back with an actual concern, can we know which of our two responses to use, and justify using it. I mean, there’s no way this person is skeptical after talking to all the Responsible Authority Figures, right?
NPR claims that lower rates of vaccinations among blacks and latinos are entirely due to accessibility issues and have nothing to do with hesitancy. I completely buy that the access issues are doing a lot of work here, but it seems odd to attempt to suddenly shift from “here are all the legitimate and sympathetic reasons why these groups would be hesitant” into “they are not and have never been hesitant, it’s that we didn’t give them access and made access depend on things that systematically excluded them.”
It’s a claim that we’ll be able to evaluate soon enough. As appointments become widely available via walk-ins in more places, with essentially no hoops involved, either the rates will converge or they won’t. I am skeptical because it seems like it’s a motivated shift in explanation rather than an attempt to track the truth - we want to make skepticism more blameworthy, so we need to not identify these increasingly blameworthy motives in the wrong places, hence the shift. I am only somewhat skeptical because it seems clear that providing easier access has a dramatic effect on vaccination rates.
Overall, that evidence means that the article seems like very good news. What it does make a strong case for is that there is a lot of ‘soft demand.’ The bad scenario for where we are would be that 60% of eligible people have already been vaccinated, and most of the remaining 40% are actively having none of it. They are like the soldiers. They won’t accept the shot unless convinced or heavily coerced.
Instead, this new picture finds evidence that what we have are a lot of people who prefer being vaccinated to not being vaccinated, but don’t prefer it enough to jump through a bunch of hoops. That’s great! All we have to do is get rid of the hoops and the need to jump through them, and offer them easy access. Now that we have abundant supply, that is relatively easy. Certainly I buy the anecdote that Asians have relatively low levels of hesitancy when given good access.
As someone who spent a substantial amount of time and effort to get vaccinated earlier rather than later, and to get those around him vaccinated earlier rather than later, I think those unwilling to do so are setting their price too low. We can separate this setting of a low-price into a few different components.
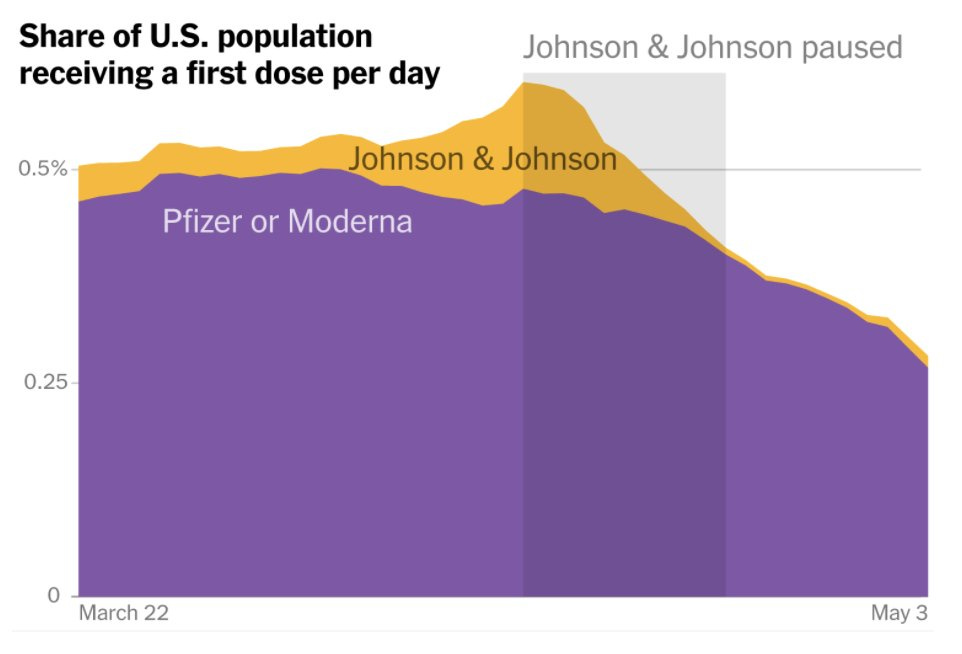
One explanation, which is the most hopeful with respect to the vaccines, is that their circumstances mean that paying the relevant costs is more expensive, and they have less ability to pay such costs. They care, but as the article claims, they are simply unable to take even a few hours off of work, or figure out how to navigate the barriers previously required. There is some of this, but we have some evidence that is then hard to explain if this is the main thing happening, such as the failure of J&J shots to rebound, and the distribution of shots on different days of the week.
J&J shots are going, well, not great:
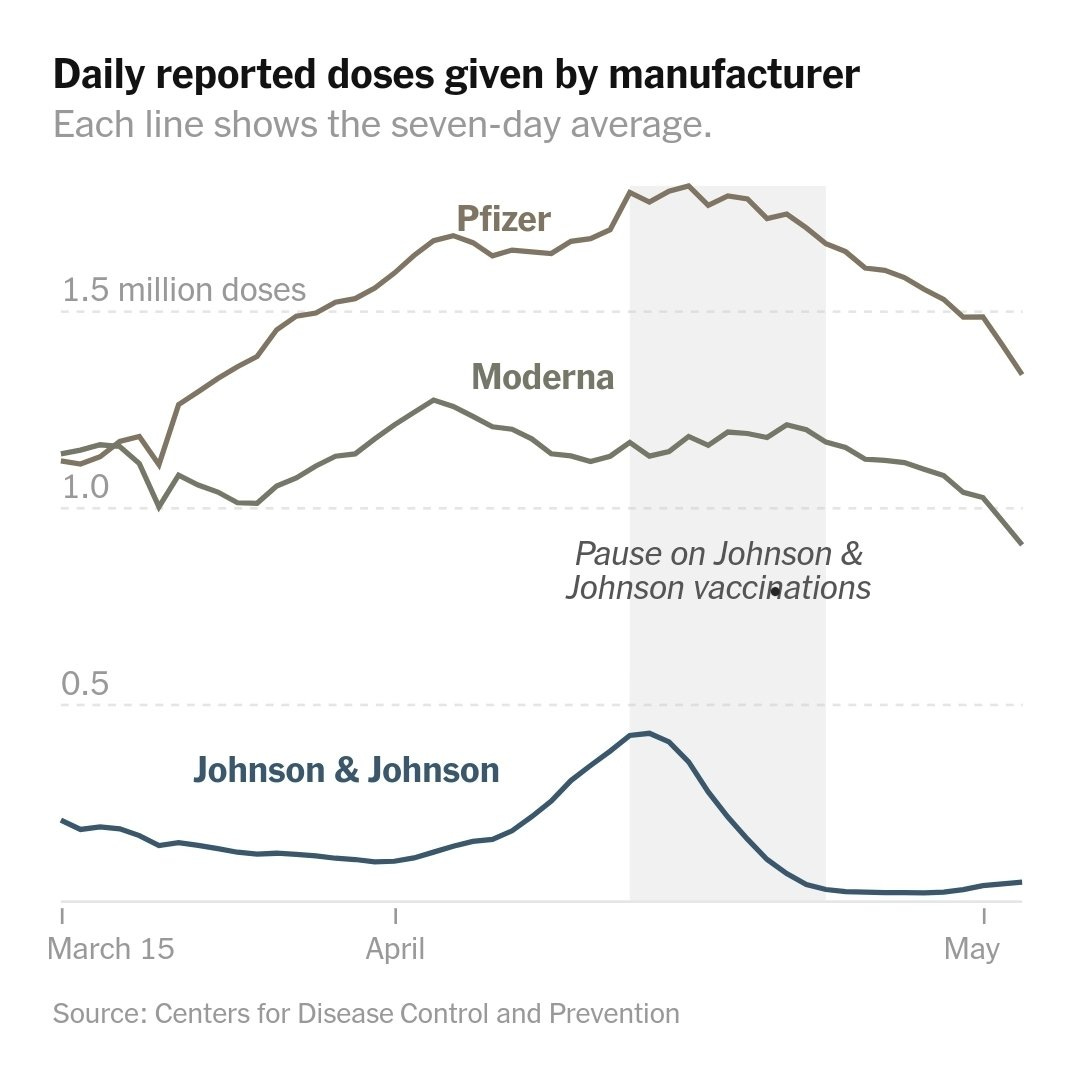
If people simply cannot miss work, and are worried about side effects causing them to miss work in addition to the appointment itself, this suggests people will plan their shot around not missing work. That means getting a shot on Friday or Saturday, and yes we see giant spikes in shots given on Fridays and Saturdays, including during periods when supply constraints looked like they were binding. That seems like strong support. We’ll see if this can be sustained; if this theory is correct, Friday and Saturday throughput should continue to bind.
A second explanation is that this is shallow demand, pure and simple. If someone wouldn’t be willing to spend much time, let alone much money, to get a vaccine, that’s a revealed preference that they don’t value the vaccine much. This seems highly plausible to me, that there are essentially three camps rather than two camps. There’s the people who want the vaccine enough to ‘bid’ on it in various ways and make it a priority. There’s the people who actively don’t want the vaccine, often violently so. But then there’s also a large group, plausibly larger than the second group, who are fine with it but are mostly trying to live their lives and value the vaccine at some positive but small number.
I wonder how much of that is because we’ve set the price of the vaccine, and much of health care, to $0, thus sending the implicit message that such services are, in emergencies, not that valuable. And also the general instinct to not think about one’s health when one isn’t forced to. We do seem to see a pattern of people who have the ability to get expensive medical care that they ‘should’ want, but not to spend small amounts of time (and aggravation) to collect it.
What’s The Worst Possible Thing You Could Do?
If you’re the President of the United States, in terms of actual impact the answer is presumably ‘launch all the nuclear warheads.’
If one restricts to the pandemic, the answer would be to sabotage vaccine production and distribution. Nothing else comes close. One could plausibly argue that nothing else even much matters.
How would one sabotage vaccine production and distribution?
Sabotaging distribution means doing things like not approving known-to-be-safe-and-effective vaccines, or suspending existing approvals and sending the message the vaccines are unsafe, or holding up distribution to worry about things like equity, or holding onto vaccine doses for extended periods with no intent of approving them ever.
Oh, wait. Those are all things done by the Federal Government during the Biden administration, with no visible attempt to prevent them from happening or even regret expressed about them. You could even add, during the campaign, questioning the vaccine development process as ‘rushed’ or ‘politically motivated,’ plausibly being the cause of vaccines not getting approved a month earlier and creating much additional vaccine hesitancy.
You’d also give doses to children who don’t need them rather than those in other countries that badly need them, so naturally Pfizer is on that one and soon will be applying for approval for children as young as two years old. And of course you’d continue not to do the first doses first, and continue to use full way-too-big doses of Moderna, and so on and so forth.
None of that means one couldn’t have done or in the future do more of those things, so actions haven’t been maximally destructive. But they’ve been quite destructive.
The other half of the worst thing you could do is sabotaging production. The easy way to do this is to screw up distribution. If things aren’t approved yet, at best then that’s going to slow down production until after approval. So are all the regulations involved in production, like needing to apply for permission and wait substantial time for permission for things like ‘put more of the vaccine into each vial because we’re short on vials.’
That’s all passive resistance to lifesaving medicine. Could we kick this up a notch or two?
The ultimate way to hurt vaccine production, not only now but indefinitely into the future, would of course be to destroy the financial incentive to produce vaccines. The less you’re willing to pay, and the less you let companies profit, and the less you reward those companies for quick scaling up and delivery of production, the less doses you’ll get. This starts with not paying for building production capacity, and its central action is not paying much per dose or paying more for early delivery. If you want to go for bonus points, you can be like Europe and hold up negotiations for weeks to drive down the price even lower.
That’s all negative actions, though. It’s easy to sabotage efforts by not doing the right thing, especially when the right thing costs tiny amounts of money and looks like rewarding corporations, and is an action rather than inaction and thus blameworthy.
So it’s a big step-up in the civilizational sabotage game to actively take away the incentive to create vaccines, by stripping away intellectual property protections without any compensation, in the middle of a pandemic:
There’s a simple solution to the problem of intellectual property if you wanted to make the situation better rather than worse. You could buy the intellectual property rights from the companies involved. So, basically, this:

It’s not that much money, everyone would be happy, and the precedent would be excellent. Pay enough, and they’ll even aid you in technology transfers. Even better, you could repeat this process with other drugs. Buy out the monopoly at its economic value, remove protections, and the people save many times that much money in costs. It’s a great idea.
Doing this without compensation is about the worst thing one could do. If your new ideas outright save the world, we’re going to reward you by confiscating them, voiding the contracts and promises agreed upon and informing you that we are not a nation of laws. That’s exactly how not to get vaccines next time there’s a crisis, or anything else next time there’s a crisis, or really anything else useful at any time for any reason.
The message we’ve sent, loud and clear, is that we are not a nation of laws and we do not reward those who deliver the goods for us. Instead, we retain protections on things like insulin that are pure rent seeking, while taking away protections that are doing exactly what patents are designed to do: reward those who produce world-changing positive innovations via temporary ability to profit.
We are a nation of a person in charge, and if that person decides to confiscate your property because it’s good politics, well, tough.
It’s a horrible, horrible precedent. We will pay for it in money, will pay for it with our freedom, and we will ultimately pay for it in blood.

mRNA vaccine technology is potentially a full cure for infectious disease, and plausibly also a cure for cancer. The federal government sabotaged all that, big time.
What did we get in exchange? What’s in the box?
NOTHING!
Unless, of course, they are not so stupid In which case the destruction of the rule of law and of private incentives, and the signaling that political expediency is the most important thing, was the point.
You see, this will not increase vaccine production (MR link with full explanation, recommended), for two reasons, even if vaccine ingredients didn’t prove to be limiting factors. MR also recommends this Barron’s column. Here’s another confirmation that no, this won’t improve short term supply.
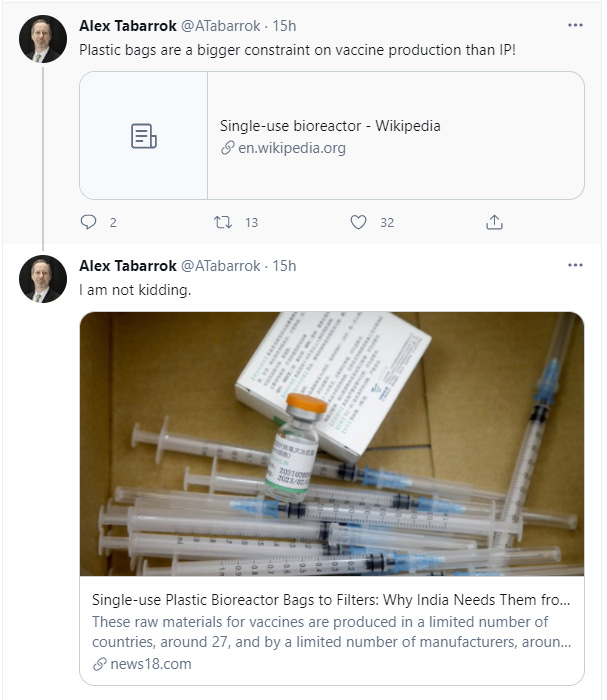
Many people have this idea that all the knowledge and skill required to produce the vaccines lies in the patents. Once you lift the patents, lots of other companies can go start producing vaccines. Except, that’s not actually true because
The vaccines require technical expertise not included in the patents, which is expensive and slow to transfer, and which would also transfer valuable knowledge that can be used for other R&D and other production and thus which the vaccine producers are not going to transfer without compensation.
Moderna explicitly already said they wouldn’t enforce the patents, and no one really expected the others to either.
Read that second one again, if it’s new to you. The greedy capitalists whose rights you took away without compensation were already voluntarily giving those rights away. If there was already clearly no intent to enforce the patents, what good does lifting those patents do?
It sends the message that the United States is willing to confiscate property for political gain, when it feels like it, on the basis of the executive’s say so.
Even though that won’t produce anything useful, yes, it’s still bad for business and still punishes exactly who we should be rewarding, or at least demonstrates that such punishments should be expected, as measured by the stock market. Remember Moderna already waived its rights:

As usual, the usual suspects wasted actual zero time demonstrating exactly the slipperiness of the associates slopes, as they quote the decline in shareholder value as a good thing:

What makes such a statement so maddening is that she’s right. We should totally do insulin! It’s completely insane that we’ve allowed regulatory capture and rent seeking via intellectual property protections on “inventions” like insulin. The congress should get together, write a bill and pass a law that stops such things from happening now or in the future via changing protections, ideally without confiscating private property, and then the President should sign it, and then the bill should become law. Then do copyright.
Won’t Someone Please Think of the Children?
The minds of many parents I know are turning to the question of summer camp. Is it safe to send your young child?
Are all the people you care about that will be in contact with that child either other young children or fully vaccinated by the time the camp starts?
If the answer to that question is yes, then yes.
If the answer to that question is no, then given that vaccinations are now available to everyone pretty much on demand, why isn’t the answer yes?
If the answer to that question is that someone is seriously immunocompromised, or otherwise super important to the child’s life and won’t get vaccinated (for whatever reason), then and only then is it time to look at the camp’s procedures to see whether you’re comfortable with the level of risk being taken. In particular, you’ll need to ask how many children and unvaccinated adults will be in contact with your child, how close that contact will be, and how much time will be spent indoors, and do a calculation.
I still think that calculation should almost certainly be ‘yeah, it’s fine’ but at that point, as they say in the advertising business, it’s up to you.
My general answers regarding children generalize this. Young children are not at enough risk from Covid to let this change how they live their lives, so them catching it only matters to the extent that they would pass it on to vulnerable others.
By the end of May, with notably rare exceptions, patience with those in the United States who are still vulnerable can reasonably be at an end. Those who decline the opportunity to be vaccinated can manage their risk however they choose, but life beckons.
Speaking of life beckoning: I strive not to use the word evil, I avoided using it in the previous section, but this is evil in its purest form:

Anyone who doesn’t recognize this as such has lost their soul. Any parent or teacher who enforces this should be treated as the mustache-twirling villain they are. I am deeply sorry to any child who has been so absurd and tortured, or living in so much fear, that they are tempted to put up with this.
If you do not think school’s primary nature is ‘child prison’ and/or that those running it are pro-children, then you have new data your model needs to somehow explain.
In Other News
V-NY day approaches, and Cuomo fully opens up stadiums, opens up Broadway, offers subsidized vaccinations at Mets and Yankees games. Took everyone on Broadway by surprise, so it’ll be a while before they can actually get on with the show. Remember, you’ll want to wait to get vaccinated until you attend a game at the stadium, together with tens of thousands of other people. That way you get free tickets!
Alternatively, you can show up at the local CVS and maybe pick up a gift as well :
In many cases, Walmart too. Basically everywhere at this point. No excuses!
South Korea says AstraZeneca shot 87% effective after one dose. Which would be pretty good after two doses. First doses first, indeed.
Police have low rates of vaccination, endangering those around them who they forcibly interact with and likely killing them (WaPo), but no one is able to make them do the right thing and stop endangering the public. A little on the nose, if you ask me.
Airline boarding procedures were already worse than random, and changes in response to the pandemic made them worse still. It seems that looking like a good procedure is more valued than being an actually good procedure. There seems to be a strong match between ‘this is a quick boarding procedure’ and ‘this is a safe procedure,’ so the problem is purely that good procedures don’t look good and/or don’t feel ‘fair’ somehow, or miss out on some opportunity for price discrimination. Is there an improvement that would also look and feel like one?
MIT requires vaccinations, although so far only for students. I expect most colleges to follow suit if only to avoid potential liability concerns. Not spreading the requirement to faculty and staff seems like a clear mistake.
New higher estimate of true number of Covid deaths via MR, not enough data to know how much credit to give this.
The Covid Response Project chronicles the Covid-related experiences of people across different states. I’ve sampled and it seems like a good source of real people’s anecdata. There will definitely be surprises.
Twitter thread and paper discussing origin of variants of concern. Not sure there’s practical updates to be had, but interesting information.
Pfizer begins shipping some vaccine doses manufactured in the United States abroad, starting with Mexico.
Potential universal coronavirus vaccine proposal. From what I can tell this is highly unlikely to work but you never know.
Vaccination availability site of the week, Vaccinate the States.
Marginal Revolution points us to a study of future work-from-home (WFH) patterns (paper), and finds dramatic effects the study expects to linger beyond the pandemic. I hope to check this out in detail in the future, but the headline impacts are gigantic. They expect WFH to go from 5% of full workdays to 20%, and for this to be a 5% productivity boost, most of which will be due to reduced commuting. Commuting is much worse than people think it is, so this is a really, dramatically large effect, in the range of ‘potentially a bigger long term deal than the pandemic.’ This isn’t a fake productivity boost, it’s literally getting rid of purely wasted unpleasant time (that also burns a bunch of carbon to boot). Given the amount of time being saved, it also implies that on the margin there’s still going to be a dramatic underutilization of WFH as an option. If a change to 15% of the workforce produces a 5% productivity boost by saving useless time (and it’s still an if, the story has to check out), clearly we are not using anywhere near enough of it.
Not Covid, therefore... we’re coming back, baby! HYPE!