

Covid 5/12/22: Other Priorities

There is zero funding for dealing even with the current pandemic, let alone preventing the next one. The FDA not only is in no hurry to approve a vaccine for children, the new highlight is its focus on creating a dire shortage of specialty baby formula. Covid doesn’t kill children, merely causing governments to mandate they not get to have their childhoods, but 40% of formula being out of stock is a much more directly and physically dangerous situation. The FDA has a history of killing children via not letting them have the nutrition they need to survive, last time it was an IV formulation that was incomplete but couldn’t be updated for years, so we shouldn’t act all surprised when this threatens to happen again.
Also Covid is still a thing. New subvariants of Omicron continue to slowly gain dominance and case numbers are increasing. The jump this week wasn’t as big as the headline number but it was still big, and is backed up by my local anecdata. There’s once again a bunch of Covid out there. The key is whether we can continue to get on with life and not fall into the trap of doing expensive prevention that doesn’t accomplish anything. So far, so good.
This intentionally still excludes China. News on that front has slowed dramatically, I plan to write up the last few weeks into a post anyway relatively soon.
Executive Summary
Case numbers up, although death numbers still down.
FDA causing specialty baby formula shortage crisis.
Still no funding for anything pandemic related.
Let's run the numbers.
The Numbers
Predictions
Prediction from last week: 400,000 cases (+22%) and 2,720 deaths (+10%?)
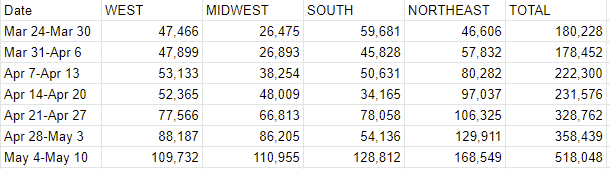
Results: 518,048 cases (+41%) and 2,084 deaths (-6%)
Prediction for next week: 640,000 cases (+23%) and 2,100 deaths (+1%)
I’d love to go back and do a study of my predictions at some point if I find the bandwidth, and in particular on whether I should be ‘sticking to my guns’ more when a change doesn’t make a lot of sense. Often a blip causes an adjustment in the wrong direction and this week feels like I ‘fell for’ that trap once again, but that implies we know it wasn’t a legitimate change.
I also suspected there was some sort of two week cycle, and, well, yeah. It’s Florida, which is literally only reporting numbers every two weeks in the Wikipedia data this past month. Flat out 0 cases last week and three weeks ago. Should have caught that, and it explains the drop in the South very cleanly. Not sure how I missed it before.
Even adjusting for that, the jump this week is large - we got the additional 13% we ‘missed’ last week and also the adjustment I made based on the miss. Early signs from a few weeks ago that things would soon stabilize appear to have been wrong. Cases are likely to continue to rise for a bit.
I don’t expect the +41% to happen again, but as new subvariants spread this seems like a time to expect large week over week case growth, so even with Florida maybe not reporting at all (need to hedge on this), I’m predicting a +23% jump.
Deaths
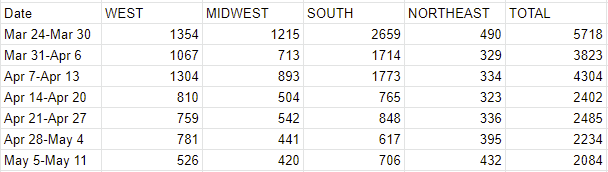
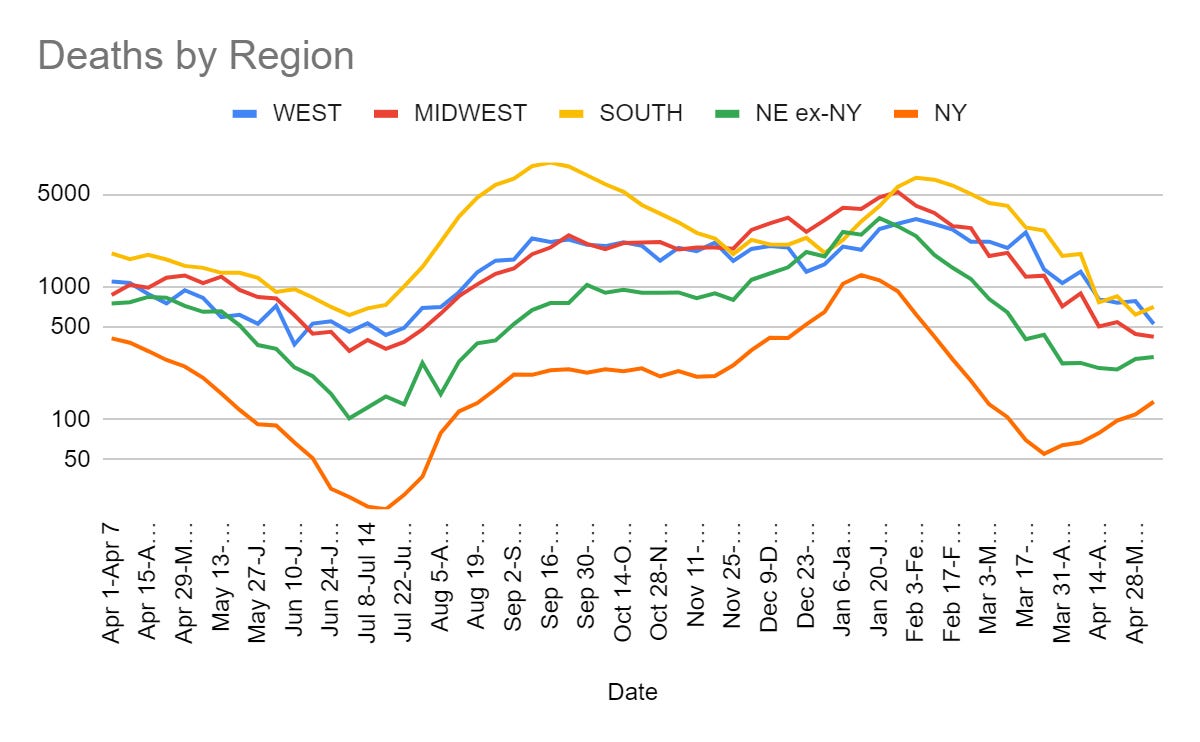
This is even more dramatic than it looks, with Florida effectively shifting over 100 deaths from last week forward into this one. The Northeast and New York lines do indicate that deaths will start going back up again at some point, but for now the ‘fading out’ of with-Covid cases and old cases continues to drop reported numbers. My guess is that ‘real’ Covid deaths have been rising, so once the backlogs are sufficiently cleared we should see deaths rise again. But we also need to adjust for Florida likely reporting nothing.
Question for everyone: Should I instead be predicting the ‘real’ answer and committing to smoothing out Florida if they don’t report in a given week? I don’t want to do that without thinking more about it first but I’m guessing I should shift to that starting next week.
Cases

Personally known cases are also on the rise, as both my kids’ schools had Covid issues this week. One school closed down, the other put masks back on but remains open. I have no doubt many cases are being missed.
Will all these extra cases translate into either new forced prevention measures or a major surge in deaths?
So far the answers to both questions are solidly no, which is great, but we won’t get many new deaths from the cases jump for another few weeks, so it’s too early to know on that front. Obviously doubling or more of cases is going to kill more people, but I expect the death rate this time around to drop even lower than before given how many cases will be reinfections or otherwise of relatively less vulnerable people.
Given that, and the general attitude everywhere, I am optimistic that we won’t see much if any rollback in the lifting of restrictions. We will instead continue to muddle through, and deal with local situations reasonably if and when they happen.
The Federal Funding
You did not receive the federal funding. Perhaps you can still take your colleagues out to dinner, but you probably can’t afford to pay your brother to come and sing.
More importantly, you can’t research or treat Coronavirus, or engage in other medical research, due to a lack of funds. This is still the situation:
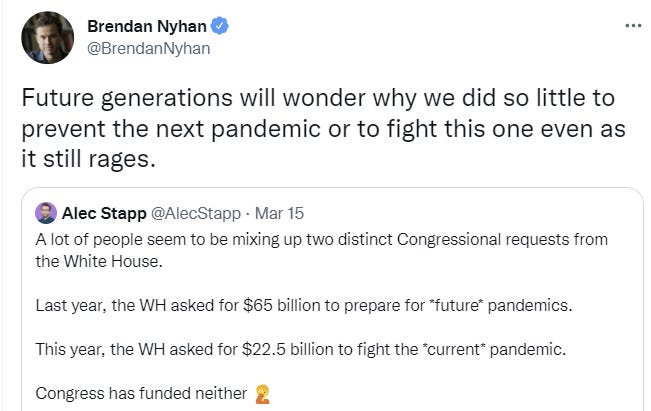
Larry Summers is likewise expecting confusion among future historians.
Even the $10 billion (reallocation of previously allocated Covid funds) compromise fell through. Zero funding. None. Zippo. Zilch. Not a thing.
It’s already too late to get fall turnaround on updated vaccine shots.
The thing is, I’m not expecting future historians to be confused here. Assuming there are still people around to be historians, I expect them either to have some totally bogus narrative that has nothing to do with anything real, or quite likely to know exactly what happened. It’s not like it’s that complicated or subtle or secret. This is who we are and how we work and what we care about, and how our dynamics play out. Us failing to predict this in advance was us having a bad model. That’s on us.
Matt Yglesias titles his post this week ‘we need to find ways to do faster clinical research’ but it seems more like we need to find ways to do much in the way of clinical research at all, on Covid or almost anything else.
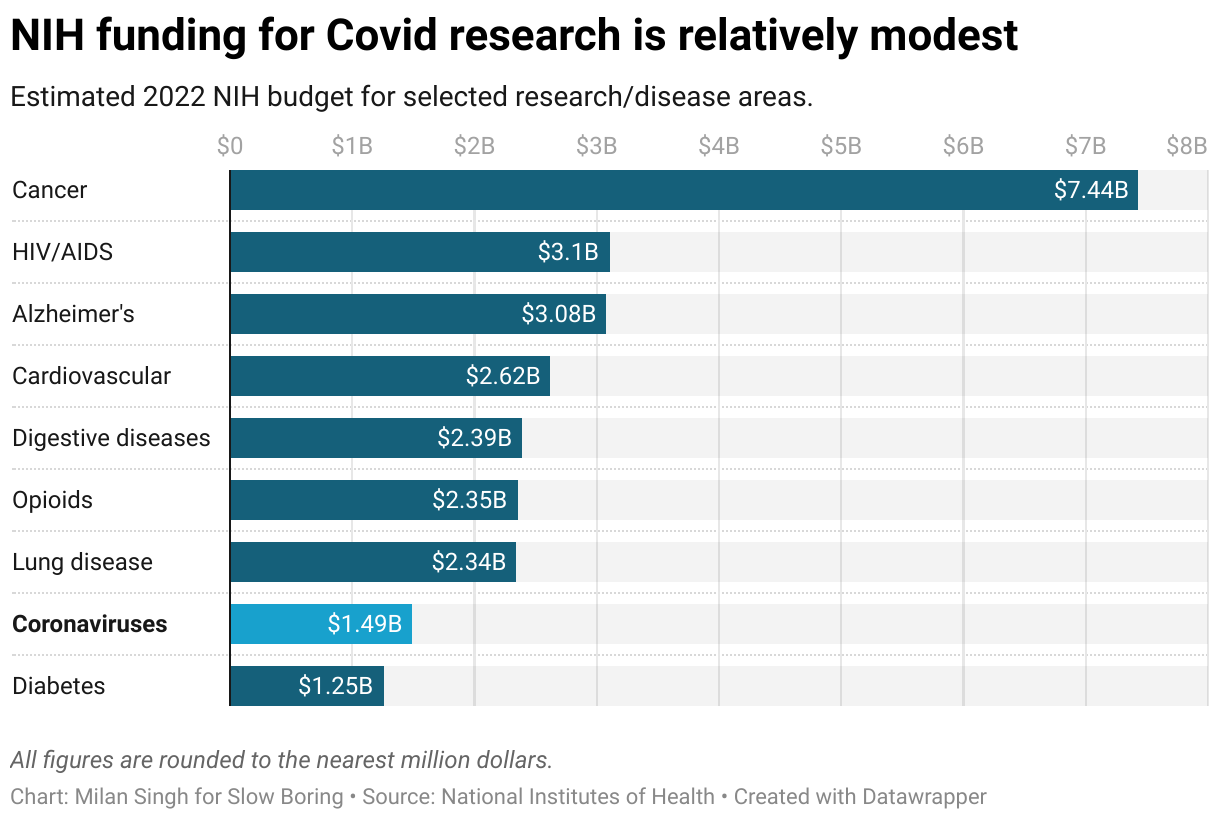
Coronaviruses, and other potential future pandemics, seem important. It seems important to prevent them. Congress disagrees.
When we do run useful studies that are trying to figure out answers rather than jump through regulatory burdens, it is interesting to once again point out how dirt cheap they are.
Matthew Herper at Stat used the ivermectin result as the peg for a piece on platform studies, writing “New Covid trial results may point toward better ways to study medicines” and explaining that TOGETHER was just one of several successful studies that all used a new and unconventional methodology.
TOGETHER, like the RECOVERY study conducted in the United Kingdom and REMAP-CAP, conducted basically everywhere but the United States, was a platform study, a streamlined clinical trial that evaluated multiple medicines at once and that use a common placebo group. It’s from these platform studies that doctors have learned perhaps the most about Covid-19.
One thing Herper notes is that these trials were “comparatively inexpensive,” with one costing $10 million and the other even less.
The main barrier to finding out vital information about a pandemic is not a lack of federal funding, rather it is the far more brazen ‘the government will not let us find out in better ways, and thus this is the best we can do.’
Of all the studies we did, a large percentage of the value came from one study that cost $10 million, and which was privately funded.
So you might think the NIH and other federal agencies focused on public health would be funding this stuff. But you’d be wrong. It’s all private donor money, mostly (according to Herper) from Stripe CEO Patrick Collison and FTX CEO Sam Bankman-Fried.
Because of course it was Patrick Collison and Sam Bankman-Fried. There are a handful of other names one could add to that list, but the world actually is this small and contains this few people, so there were more than two people who might potentially have written these checks but realistically there were maybe… ten of them?
Lately I’ve been looking into the more general question of ‘what in-some-sense-realistic policy changes might do the most good on the margin?’ much of which is extremely difficult to quantify and therefore to prioritize. Early in the pandemic, being allowed to learn key facts about Covid-19, or being allowed to develop and deploy helpful things like tests, treatments and vaccinations in reasonable time, would have saved millions of lives and trillions of dollars, and prevented or minimized many massive life disruptions across the board. At this stage, how high a priority these questions have depends on how likely that is to happen again how soon.
Physical World Modeling
Recovery from Omicron infection may produce narrow antibodies in a way that vaccination (or the combination of Omicron and vaccination) don’t, perhaps leaving people vulnerable to new variants. Vaccination still a very good idea.
Yes it helps to open a window, we needed a study for that.
Paxlovid has a strange problem. If you don’t deploy it quickly enough, it will be ineffective. If you deploy it too quickly, your body might not have time to develop its defenses, and then sometimes Covid rebounds afterwards. This didn’t happen in trials under old variants, but Omicron symptoms show up faster, and also some virus maybe gets stuck in the respiratory tract which makes rebounding more likely, so it is happening now sometimes. It’s still only about 2% of cases, but it does happen, and it raises the possibility that resistance to Paxlovid might evolve. Mina recommends moving us to a 10-day treatment plan. If we had unlimited supply, I would strongly agree. However, unless the resistance question is a big deal (I don’t know how big it is), it is hard to say that getting 98% of the effect for 50% of the supply is a bad deal while supply shortages persist. Yes, there’s currently enough supply for everyone eligible, but until everyone is eligible I still consider there to be a supply shortage.
Shooting fish in a barrel department presents The FDA’s Extreme Innumeracy. Once again, the J&J vaccine is being limited due to blood clot concerns, where those concerns are size epsilon. Once again, to the extent this changes perception it will make things worse rather than better. As far as I can tell, approximately no one is getting J&J at this point anyway, so in practice it doesn’t matter except to illustrate that it is likely to happen in the future when it does matter.
Prevention and Prevention Prevention Prevention
Europe’s ECDC stops recommending masks at airports and on planes.
I found this thread interesting as an illustration of how much some people continue to let their lives and brains be hijacked by Covid concerns. Here’s the part before the first poll.

All these details about exactly where to do how much masking where and how much exposure to accept each step of the way. I remember those times, and I do sympathize when dealing with elderly that have comorbidities. When I see young healthy people potentially obsessing, turning life into some sort of morbid probability matrix because one particular potential risk (Long Covid) has been made more salient and blameworthy, I sympathize a lot less. When scaremongers say things like us not being ‘ready’ for ‘one eighth of the population with months or years of disability’ I don’t even know how to engage with a claim that implies such a different world than the one we exist in.
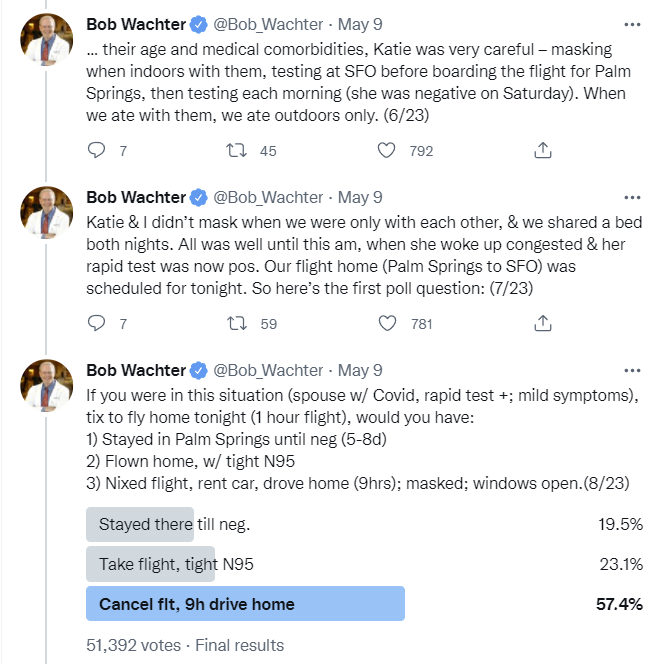
Now the question was, what to do once Katie tests positive? My answer before reading further was very much with the majority, of course you rent a car and drive home. Staying in a strange place for 5-8 days while sick and unable to do anything, forced to rent a place, seems way worse than a nine hour drive. You certainly can’t stay with older friends. So I’m confused that 19.5% of people wanted to stay, even if the place is called Palm Springs.
More worrisome are the 23.1% of people who wanted to take the flight while known to be positive. Thus, almost one in four people who follow a cautious doctor who writes frequently about Covid in the style above think that a known symptomatic Covid case should still go to a terminal and get on a flight. How many more of the general population must think the same way? That it’s fine to go around exposing people when you’re sick?
Well, maybe it’s not as clear cut as all that?
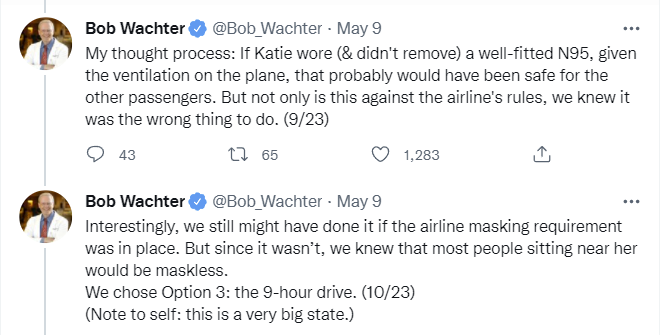
This is certainly a rather strong ‘planes are safe for Covid’ position, where it would be fine to put a known Covid-positive case on a plane (and more importantly, in the terminal to and from the plane) so long as everyone involved had masks, but without others wearing masks it turned into an unacceptable risk.
I notice my skepticism that things fit into these windows. A mask is a modest risk reduction. Even if we are super generous to both masks in general and mask use in practice and say 75% reduction between the two scenarios, a factor of four is actually rather unlikely to change the answer here. Which suggests that the masks are serving more of a symbolic ritual purpose, rather than anything else.
In any case, option 3 was chosen, which seems clearly correct.
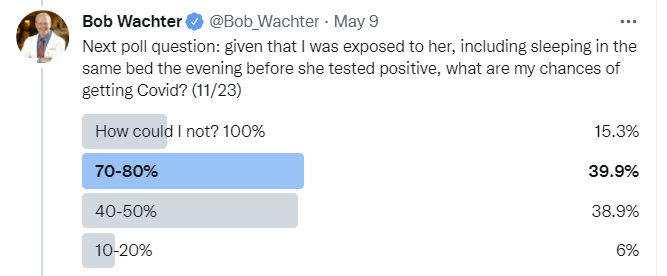
It’s funny how there’s four choices and they only cover 40% of probability space, but each contains a range. I don’t know if I’ve ever seen that before - normally either you cover most or all of the ground or you choose between four point estimates - e.g. if this said 15%, 50%, 75% and 100%, that would make perfect sense.
Here’s Bob’s answer.
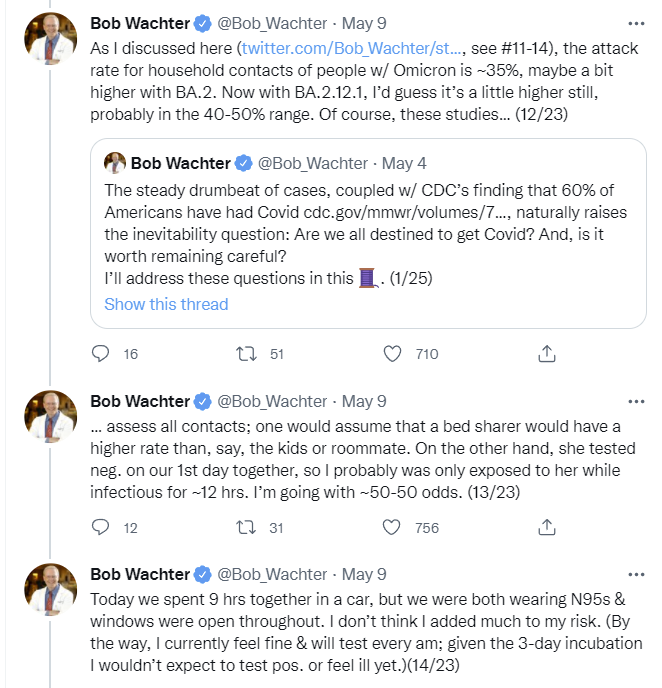
It seems odd to do that analysis and still get up to 50%, but a lot of this is that the 35% household attack rate is highly unintuitive. We know it intellectually, but man is it weird.

I agree that the only ~5-10% chance here is right. And I’m happy with the 87% on the final vote given this is the internet. Rest of the thread is wrap-up.
Think of the Children
The younger ones still aren’t legally able to be vaccinated. The odyssey on that continues.

So now they’re willing to do the reviews one at a time after delaying to not do that, which is odd but I try to avoid ratting on people for having been wrong before when they decide to do something right now. Meanwhile, there’s no communication issue since there’s no decision, the vaccine is illegal. If it was legal, I’d say something like ‘future variants may decrease vaccine effectiveness somewhat’ I suppose, although my motivation is not ‘scare off as many parents as possible.’
It’s very scary to hear things like ‘we will probably authorize’ if it is as good as adult vaccines against Omicron. How close a bullet did we dodge with the extreme effectiveness of the vaccine against the original strain? If the vaccine was first developed now, would we even approve it?
In Other News
New Zealand’s borders fully reopen.
Bill Gates tests positive for Covid, properly treats it as an annoying need to isolate.
An N=1 experiment with air quality during air travel. We should systematically do a lot more of this sort of thing.
Is there a reason we’ve been swabbing everyone with alcohol before giving them the vaccine? The lost time adds up. This paper claims that evidence points against the practice being useful, yet we continue to universally use it without any plan to verify its usefulness, experimentation being illegal and all. I’d say run the experiment, but I can only imagine how this would sound.
Australia’s failure to get its house in order on vaccination cost $3000 per household in economic damage versus ‘an optimal vaccine rollout.’ It’s a lot more than that if ‘optimal rollout’ were based on when the vaccines could actually have been deployed under a fully sane world. The $3k only covers the mistakes made by Australia.
Why can’t we give out our supply of Paxlovid? Many reasons.
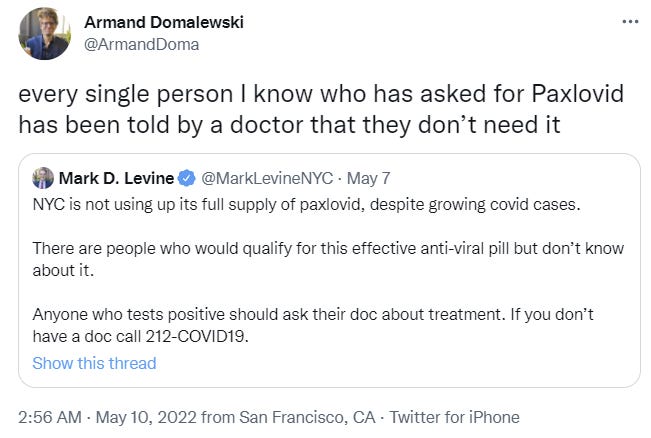

Many people don’t know about Paxlovid. Many doctors don’t know about Paxlovid, or don’t offer it, or when the patient explicitly asks tell them that they don’t need it and refuse to prescribe it.
Yes, any given patient is highly likely to be fine either way, but this is the opposite of traditional defensive medicine, which makes me wonder. Suppose you tell a patient that is eligible for Paxlovid they ‘don’t need’ Paxlovid, and then they get a severe case of Covid. Would they be able to sue? I notice how I’d be inclined to find if I was on the jury.
Formula For Dying Babies
There’s a shortage of specialty infant formula. Half of all types are unavailable. Some parents are panicking, without a plan for how to feed a baby that can’t use regular formula.
An infant formula plant shutdown triggered by two infant deaths has created a new nightmare for some parents: There’s now a dangerous shortage of specialized formulas that are the only thing keeping many children and adults alive.
The Abbott Nutrition plant in Sturgis, Mich., was not just one of the biggest suppliers of infant formula nationally, but it was also the major supplier of several lesser-known specialty formulas that are a lifeline for thousands of people with rare medical conditions, including metabolic, allergic and gastrointestinal disorders, which can make eating regular foods impossible or even dangerous. The situation has not only rattled parents and medical professionals, but has raised questions about whether the federal government should do more to ensure critical, life-sustaining supply chains don’t break down.
“If this doesn’t get fixed soon, I don’t know how my son will survive,” said Phoebe Carter, whose 5-year old son John — a nature-lover and “paleontologist in training” — has a severe form of Eosinophilic Esophagitis, a rare digestive and immune system disease driven by a dysfunctional immune response to food antigens. “I just can’t stress that enough.”
One of my good friends looked into this a bit and isn’t buying that the shortage could be caused by shutting down this one plant. This article’s primary contribution is that the supply chains were already strained before the shutdown due to demand fluctuations on top of supply issues in the wake of the pandemic. It’s certainly a large contributor, and it’s possible without the shutdown we wouldn’t have a problem.
This one points out that before the recent recall, we were on the edge of disaster to start, through a combination of the usual supply chain disruptions and the usual tariffs. We went out of our way to ensure that the supply of baby formula couldn’t compete against American dairy farmers, and, well, whoops. This quote from that post (the quote is originally from here) is very on the nose:
Canada agreed that, in the first year after the agreement takes hold, it can export a maximum 13,333 tonnes of formula without penalty. In USMCA's second year, that threshold rises to 40,000 tonnes, and increases only 1.2 per cent annually after that. Each kilogram of product Canada exports beyond those limits gets hit with an export charge of $4.25, significantly increasing product costs….
Canada wanted to attract investment for a baby formula facility because it uses skim milk from cows as an ingredient. Healthy consumer appetites for butter leave provincial milk marketing boards with a surplus of skim. Baby formula looked like a smart use for it, and Canada didn’t have any significant infant formula production before Feihe arrived.
Expanding this plant, or building a second infant formula plant somewhere else in Canada, look like less attractive business propositions under this new trade deal.
I don’t get why even people who generally sound even more infuriated about this than I do, like Scott Lincicome, still produce sentences like this first one:
These regulatory barriers are probably well-intentioned, but that doesn’t make them any less misguided—especially for places like Europe, Canada, or New Zealand that have large dairy industries and strict food regulations. Indeed, as the New York Times noted about “illegal” European formula in 2019, “food safety standards for products sold in the European Union are stricter than those imposed by the F.D.A.”
Well-intentioned? If your goal is profits for a politically connected set of rent seekers, sure. If your goal is anything else, I notice I am confused what these intentions are and how they could be defined as falling under this category of ‘well.’ I flat out refuse to buy the argument that this arises out of physical world models that cause genuine concern that Canadian formula would hurt American children.
There are two possibilities. One, the optimistic one, is that this is mostly about getting insiders more money. The other is that this is about expanding a bureaucratic power base or otherwise simply preferring worse outcomes to better outcomes.
Then we created a system whereby a large portion of all formula is heavily (as in >90%) subsidized from a legally mandated single-source, which happens to be the single source that got shut down.
And with that stage set where we restrict supply in order to jack up prices to begin with, guess who is once again going to cause children to not be able to get nutrition and potentially die from that?
That’s right. The FDA. Who shut down the plant after two deaths. Then kept it closed, citing ‘health code violations,’ it has been three months and they won’t say anything about when it might be allowed to reopen.
Still, it’s not clear why the plant is still shut down nearly three months after the recall. Neither FDA nor Abbott will answer specific questions about the status of the investigation or what the plan is to reopen the facility, which has further strained the infant formula supply chain.
One solution would be to import formula from the highly dangerous Europe and Canada, but as noted above that’s not permitted.


Meanwhile, what is law enforcement up to?
In a separate incident last year, Customs and Border Patrol (CBP) bragged in a press release about seizing 588 cases of baby formula that violated other FDA regulations. The seized formulas were made by HiPP and Holle brands, which are based in Germany and the Netherlands, respectively. Both are widely and legally sold in Europe and around the rest of the world.
…
But the new "export fees" included in the USMCA likely make it more costly and difficult for America to import extra supplies of formula from its northern neighbor. Chalk it up to another self-inflicted wound of the trade war with China.
That’s right. It’s not only about not giving people life saving medicine. It’s also about denying young children the ability to eat. My presumption is this won’t reach the point of babies starving to death this time - unlike when the FDA prevented IVs from properly supplying babies with the proper nutrients for years. I hope.
What is the FDA saying it is doing about this?
“We are doing everything in our power to ensure there is adequate product available where and when they need it,” said FDA Commissioner Robert M. Califf, M.D. “Ensuring the availability of safe, sole-source nutrition products like infant formula is of the utmost importance to the FDA. ”
They’re holding meetings, expediting reviews, monitoring the supply chain, compiling data, ‘Expediting the necessary certificates to allow for flexibility in the movement of already permitted products from abroad into the U.S’, ‘Exercising enforcement discretion on minor labeling issues for both domestic and imported products to help increase volume of product available as quickly as possible’ and most importantly ‘Not objecting to Abbott Nutrition releasing product to individuals needing urgent, life-sustaining supplies of certain specialty and metabolic formulas on a case-by-case basis that have been on hold at its Sturgis facility.’
However, they note:
It’s important to understand that only facilities experienced in and already making essentially complete nutrition products are in the position to produce infant formula product that would not pose significant health risks to consumers.
So things they are not going to allow while doing ‘everything in their power’ to fix the problem they themselves are causing include: Letting anyone enter the market, letting known-safe formulas approved elsewhere into the USA, waiving procedures of any kind beyond ‘minor labeling issues’ or letting the Abbott Nutrition plant resume production or any at-scale distribution on any known time scale.
Once again: FDA Delenda Est. Tariffs Delenda Est, longstanding but never-highlighted group member, especially when they’re on things like specialty baby formulas and solar panels we’re now going to build less of than we were under the Trump administration thanks to worries about retroactive 240% tariffs, no really. We really, really don’t care. And also of course delenda est to the idea that the solution to all our supply problems is to never use prices to control demand, demand perfect safety and to insist that all necessary production magically happens here in America somehow anyway.
“Parents shouldn’t have to pay a price because Abbott has a contaminated product,” DeLauro said, adding that there had to be a way to induce other formula manufacturers to get products onto shelves more rapidly. She also invoked the possibility of using the Defense Production Act to get more formula in the pipeline: “If there was a shortage, why weren’t we in the business of making sure that wasn’t happening? What did we do in times of crisis in the second World War, and so forth? We produced what we needed to produce.”
Earlier, it turns out… there may not have ever been a contaminated product at all?
The worst blow came in February, when Abbott Nutrition recalled formula made in its Sturgis, Mich., plant. Two babies who drank formula from the plant died of bacterial infections, and others were hospitalized. Although bacteria wasn’t found in the samples they drank, Abbott announced the recall as a precaution.
Yes, they uncovered various signs the plant wasn’t as clean as we’d like it to be, but almost nothing is as clean as we’d like it to be, the costs of closure are orders of magnitude beyond plausible costs of contamination in practice, it’s very possible those costs were damn near or actual zero, and it’s now been several months.
While I did consider splitting this off into its own post, Scott Lincicome’s coverage is mostly excellent and contains a lot of great detail, so if you want to link to something on this for general consumption, probably fine to link to him instead.
Not Covid
Do you trust science? ‘The Science’ also known as Science™? The ‘scientific community’? When someone trusts a different one, how do you label that?

In other words, Alec’s quote mark starts too early. The polarization is in trust in ‘science,’ aka Science™, which is not something one should trust even in the good circumstances that didn’t involve the last two years of its track record.
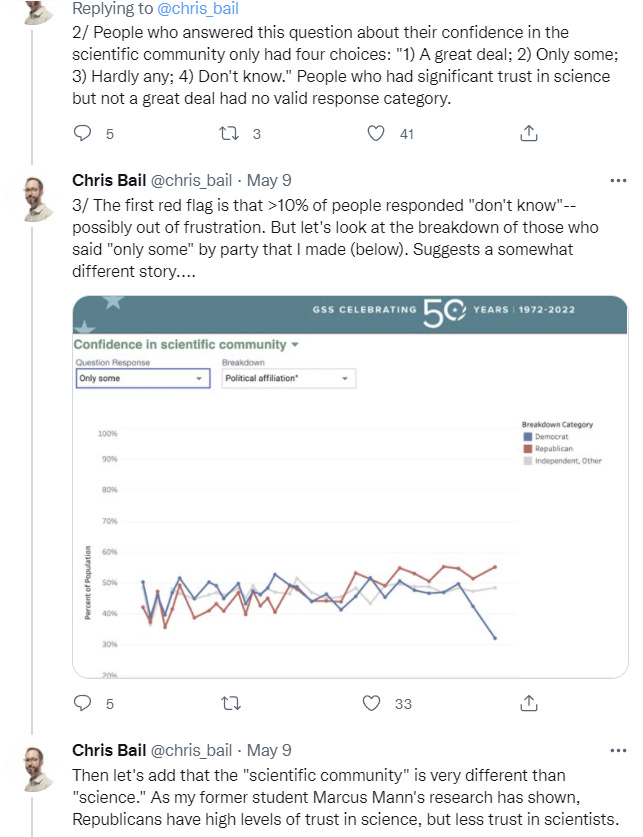
The mystery, if anything, is why the gap isn’t bigger.
Also, it seems like the EU is considering mandating AI scanning of all text communications? After GPDR only killed a third of all app development they figured they’d have to step up their game.
On the issue of alcohol wipes, I've got Type 1 Diabetes and inject insulin and prick my finger multiple times per day. Every instruction I've ever seen/gotten says to clean the site before hand with alcohol or soap & water. I've never done that and over 10 years and 1000's of injections & finger pricks, nothing has ever happened. From conversations with other diabetics, the vast majority don't clean before injections and also haven't seen any issues. It's not an RCT, but there should be an enormous amount of data you could collect to see if there's any meaningful risk of not cleaning an injection site.
"Many people don’t know about Paxlovid."
Pfizer is buying radio and TV ads that explain that there is an oral treatment you take at home for COVID and telling people to call their doctor as soon as they have symptoms. It never explicitly mentions Paxlovid because then they have to put in all the disclaimers, side effects, and drug interactions. I've seen the ads during NBA and NHL playoff games and on local sports radio programs.
https://www.ispot.tv/ad/bAea/pfizer-inc-move-fast-oral-treatment