
Covid 6/2/2022: Declining to Respond
Covid 6/2/2022: Declining to Respond

Memorial Day weekend is a good reason not to worry about reporting cases or deaths. FDA declines to respond with making it easier to get treatments we have in ample supply, or to update the vaccines. Congress refuses to fund anything at all, really.
Doesn’t sound like a state of emergency to me. Yet in California, we still have one, and we decline to respond to when we might end the ‘state of emergency.’ In New York, health officials make it clear that if it were up to them, we’d have these pandemic restrictions forever here as well.
Don’t leave it up to them. Respond.
Executive Summary
Paxlvoid and Fluvoxamine remain hard to get.
Time is not a flat circle, that’s a dumb expression, but history rhymes.
Covid-19 is a good excuse to work on curing aging, let’s do that.
Let's run the numbers.
The Numbers
Predictions
Last week I somehow once again forgot about a holiday, in this case Memorial Day, because I don’t think in those terms naturally and it still boggles my brain that it matters. But in terms of ‘why this prediction was stupid’ that’s why.
Assignment for readers: Next time a holiday is coming up and I forget about it, whoever notices first should write a comment in the Substack version that says ‘you forgot to take into account the upcoming holiday!’ and whoever does scores points. Note that if I don’t explicitly mention the holiday I’m probably forgetting about it.
Prediction from last week: 700,000 cases (+9%) and 2,725 deaths (+15%)
Results: 566k cases (-12%) and 1,994 deaths (-15%)
Prediction for next week: 675,000 cases (+19%) and 2,400 deaths (+20%)
As usual with a holiday drop like this, one must hedge between ‘it was the holiday and will be even higher than trend next week’ and ‘it wasn’t entirely the holiday, this was a real drop.’ Even if I’d remembered the holiday my prediction would have come in high. Is it possible cases have peaked for real? Definitely possible, but the decline in deaths now makes zero underlying sense outside of the holiday, so I’m guessing we’re looking mostly at a large holiday effect.
Deaths
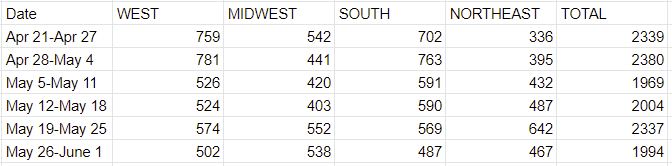
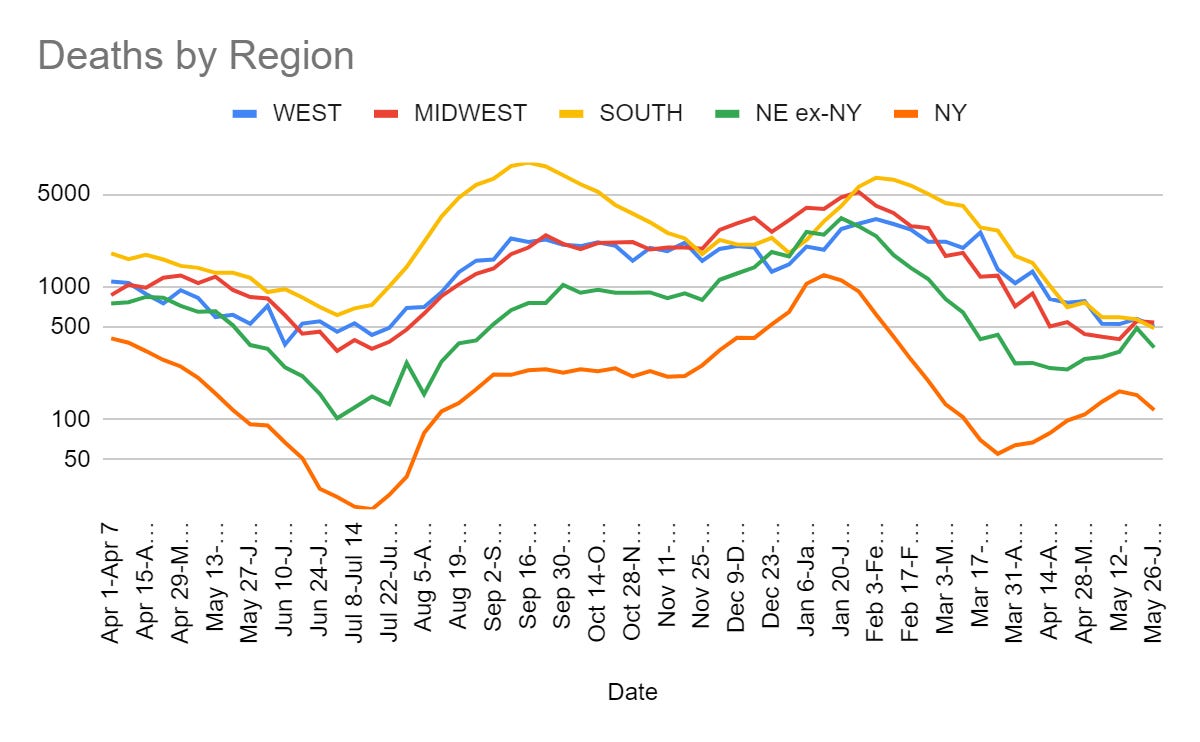
Ah, Memorial Day, yet another holiday. Silly me.
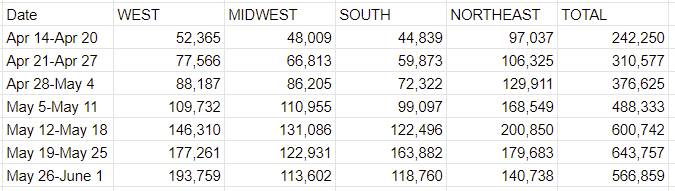
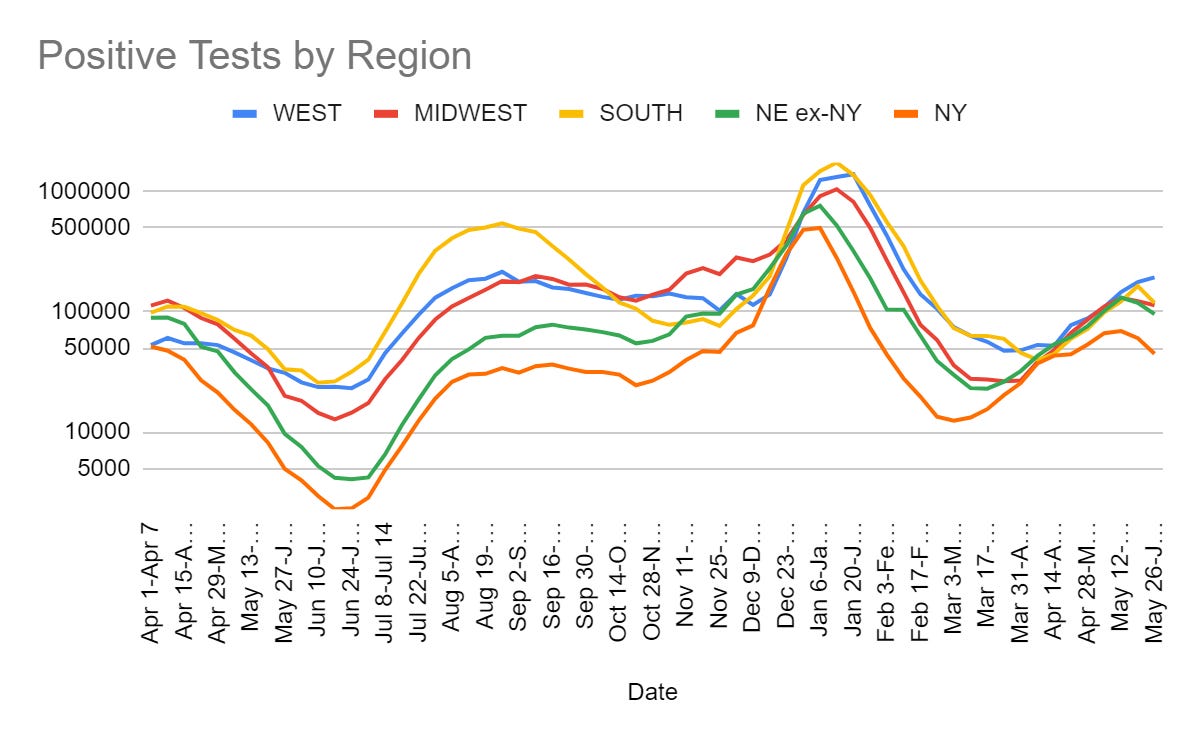
Cases
Vaccine Discussion Offer
Chise, who has provided good information several times, says their DMs are open for anyone with vaccine-related questions or even want someone to listen because you are unsure. A fine public service, if you need it please use this resource or pass it along to someone else who needs it.
Variants
Trevor Bedford thread confirming BA.4/5 will likely outcompete BA.1.2.12, confirmation at least a lot of that is immune escape, and the note that a BA.1-based vaccine update would be helpful but a BA.4 or BA.5-based update would be much better at this point.
Big Time Surge Story
How is the other half not living? It’s calling another big time surge. The note here is specific to San Francisco but the logic is universal. Everywhere will have their turns.
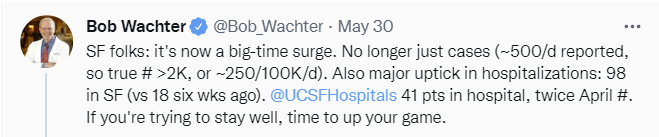


The framing here seems like the ‘friendly’ version of paternalistic public health. Are you trying to stay well? If so, time to step up your game. If not, then that’s fine too says your grandmother, don’t try to stay well and be home for dinner.
On some level I find that fair, because the whole point is that it is not worth trying to stay well, if stay well means avoid infection, which is slightly unfair but all right, fine, sure. Permanently avoiding infection is for most people not a good plan, and if you did need to have that as your plan then yes it’s time to step up your game and pull out that P100.
The contrast between Bob’s two graphs is interesting. In the first one, we have less than half as many cases now as at the start and less than a fifth of the peak. In the second, we have more patients needing care now than we did before and over a third of the peak. This implies a lot of cases are not being reported, and that this is not mostly reflective of lower severity unless most patients under care are ‘with’ rather than ‘for’ Covid (because math).
Similarly, on the question of whether the unvaccinated should be worried right now, Matt Yglesias points out the graph versus NYTimes story differential here.


Let My People Go
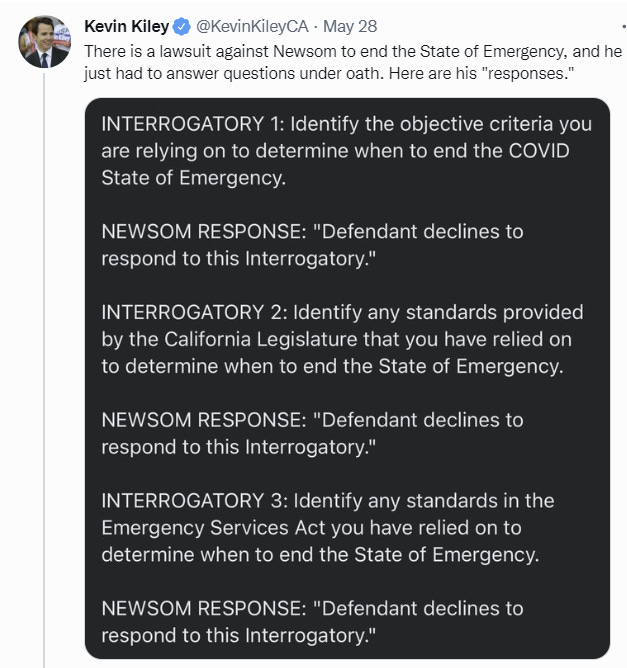
There are no standards. There are no criteria. There is only emergency.
Defendant inquires about never. He asks if never works for you.
Meanwhile CDC continues to recommend the full ten days quarantine period for children under the age of two, because they are unvaccinated and couldn’t mask. Words, I have none. Maddening lack of connection with the physical realities of life.

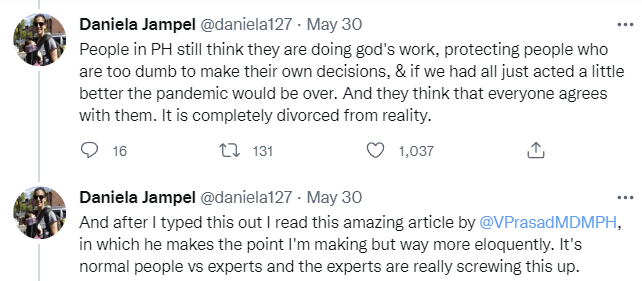
Link to the referenced article here. Both are fine but I prefer the thread.
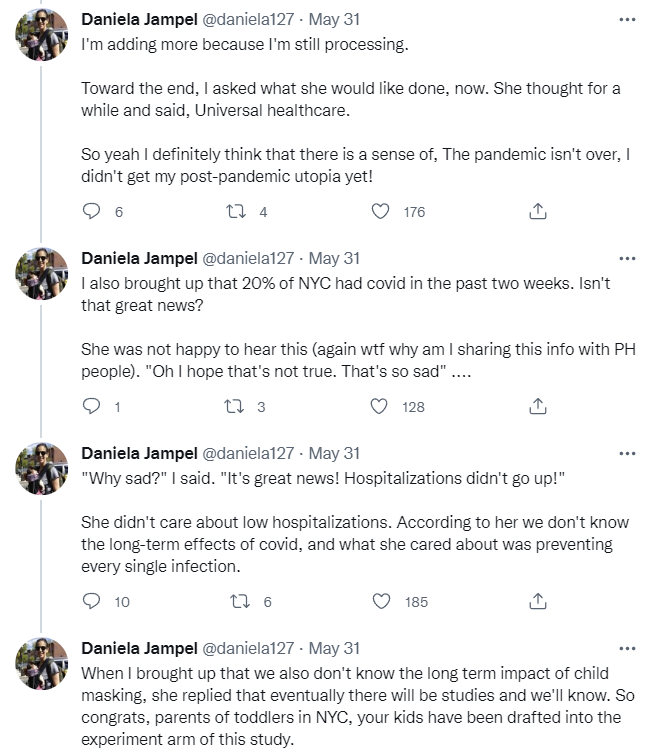
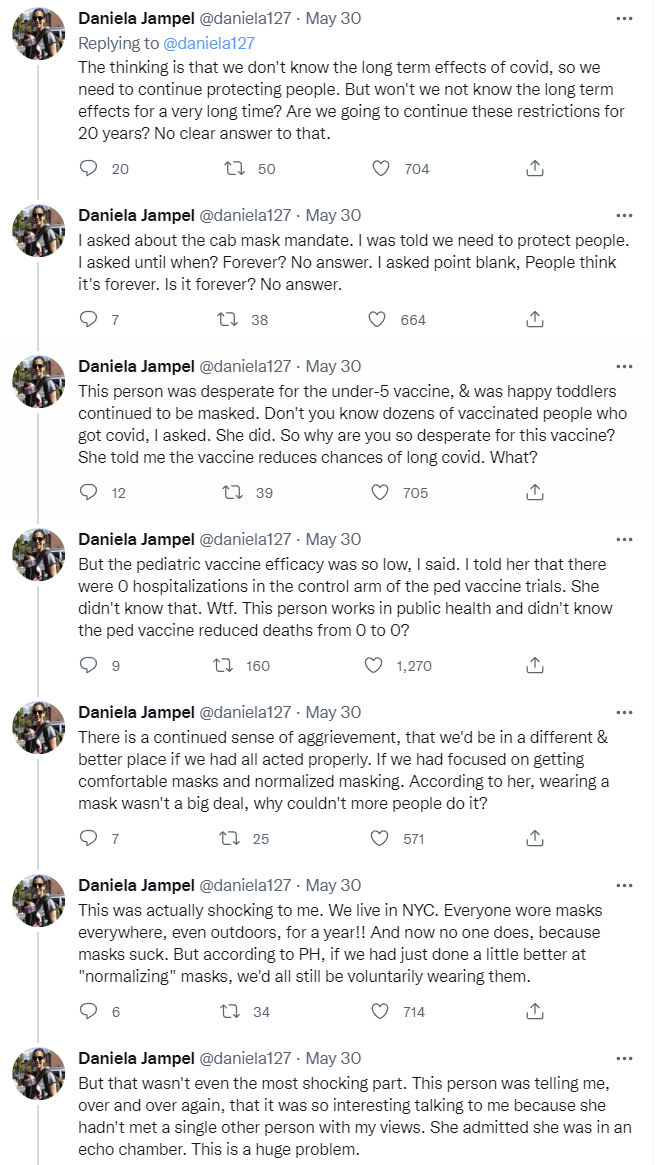
The amount of willful ignorance, of selective faith in the facts that fit whatever narrative supports restrictions today, the not caring about costs, would have been stunning two years ago. Now it’s completely unsurprising, although the ‘I never talk to anyone with the view that we shouldn’t take lots of pointless public health measures’ still packs a punch.
The juxtaposition of ‘we don’t know the long term effects of Covid so we need to destroy life indefinitely’ and ‘we don’t know the long term impact of child masking but eventually there will be studies and we’ll know’ could not be more clear.
And of course, there is nothing the kinds of restrictions we are talking about could meaningfully do over the medium term to prevent infections, even if everyone did cooperate, but hey, it’s not as completely insane as putting kids through live shooter drills.
FDA Delenda Est: Approved Treatments Edition
Tyler Cowen reminds us that Paxlovid remains remarkably hard for regular people to get and that this (OF COURSE!) is largely the FDA’s fault since they could allow pharmacists to prescribe it themselves. Quoting in full:
Pharmacists still cannot prescribe the medication themselves, a step that would cut the time it takes patients to secure the drug.
The Food and Drug Administration “is looking at this and thinking about it,” Dr. Jha said. “Whether they’re going to make a change, when and how, etc., is totally in their wheelhouse.”
Many patients are still handling the sometimes-cumbersome steps on their own: locating a virus test, then securing a Paxlovid prescription from a health provider, then finding a pharmacy that carries the pill, all within days of first showing symptoms.
Dr. Jha described being frustrated by physician colleagues who have told him they still limit Paxlovid to patients 65 years and older.
Tyler: But no they still will not do this. I repeat myself, but you need to keep in mind the only time panel members have resigned from the FDA is when the Biden administration pushed through the booster shots. Here is the full NYT article, via Rich Berger.
Then everyone goes around wondering why so few people are using Paxlovid. And this is what is ‘in their wheelhouse.’
Then there’s Fluvoxamine, WSJ asks why the FDA said no to prescribing it for Covid, which I covered two weeks ago. I mentioned then that I wasn’t concerned about that because it was mostly ignorable - you could still get Fluvoxamine if you cared enough, and if you didn’t care enough you were never going to get it. In practice, however, doctors are remarkably reluctant to write that kind of off-label prescription and there are numerous reasons why almost no one will end up taking it without the approval.
So once again, I can only conclude the FDA has reached the same conclusion as the top comment on Tyler’s post.

CDC Delenda Est
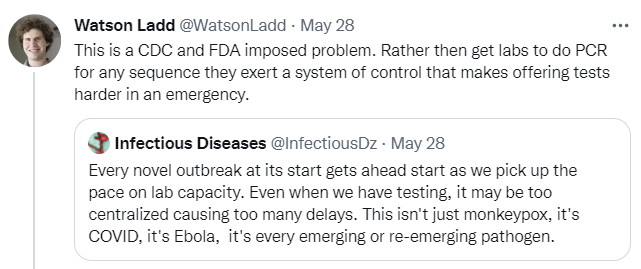
Remember when Trump complained that the problem was that we had all these cases because was did all those tests? Well…

…yeah.
The quote is from this Kelsey Piper post about Monkeypox, including that we’re still doing the whole ‘downplay the situation so people don’t panic’ thing, which is going into my list of Monkeypox links that I will use if I write a post that I sincerely hope I never write.
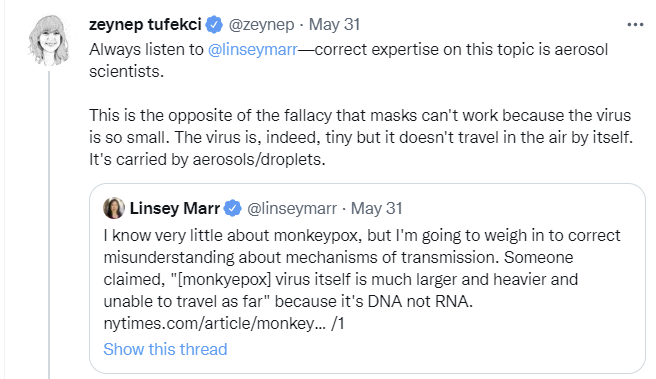
And on another note on Monkeypox, it’s worth pointing out that history is rhyming again, oh no:
Think of the Children
In Other News
The new reality of Covid, summarized.

The reality of what’s going to happen early in the next pandemic.
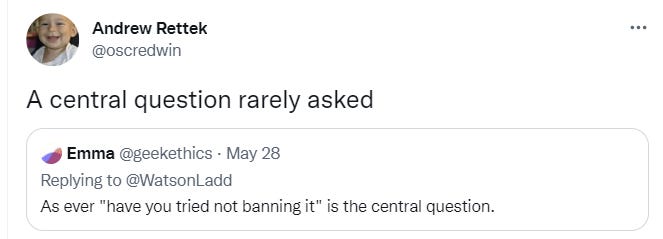
Nope. Can’t say we have.
Fund Anti-Aging Research
The beatings will continue until morale and/or survivability improve.
Aging is bad. It leads to being old, which leads to all sorts of bad things like loss of one’s various facilities and also it kills you. We should get to work on that. However, aging is not considered a disease, so attempts to treat or cure it don’t count. Most people have rationalized that the thing that slowly destroys and kills every single human is ‘natural’ and fine actually, using a variety of time-honored rationalizations. Even on the voyages of the USS Enterprise they risk the ship to save an innocent old person’s life then give that person a stern lecture about not wanting to then die on schedule.
So yeah, this battle’s been a tough one. Lost a lot of good men. All of them, actually.
However, aging is also the primary risk factor for Covid-19, so perhaps we can market our anti-aging solution as a Covid-19 treatment?

Covid-19 is far more likely to kill you if you’re old. One reason is that aged immune systems struggle to cope with infections and recover from them. So why not try drugs that make bodies young again? That’s the bold idea now being explored in clinical trials around the world, which are testing drugs that reverse the impacts of age on the body, rejuvenate the immune system and clear out aged, worn-out cells.
This does not appear to be satire. Now that Covid-19 is around suddenly we have this bold idea to solve the problem, which is to cure aging by making people younger. And no, there is no hint of noticing that maybe we should have been trying to do this anyway? Cause you know what age is a risk factor for almost exactly the same amount as for death from Covid?
Other than violence, accidents, drug overdoses and infant mortality?
Death. It increases risk for death.
Imagine if this was true not in the pandemic.
Most of the cells in our body divide up to a certain point. Once they reach this limit, they should die and be cleared away by the immune system. But that’s not always the case—some cells linger on. These cells no longer divide, and some instead churn out a toxic brew of chemicals that trigger damaging inflammation in the surrounding area and beyond.
Cells that do this are called “senescent,” and they accumulate across our organs as we age. They’ve been linked to an ever-growing number of age-related diseases, including diabetes, heart disease, osteoporosis, cataracts, Alzheimer’s—the list goes on. They also appear to play an important role in coronavirus infections.
Yes. Please do work on that. Thank you. I will totally pretend not to notice the skulls, except by the skulls I mean look at everyone who ever lived because they are skulls now, they are dead, I am going out on a limb and saying I do not like this.
We might come out ahead from this pandemic yet.
One More Note About That Long Covid Study
As I said on Twitter, every now and then they still manage to surprise me.
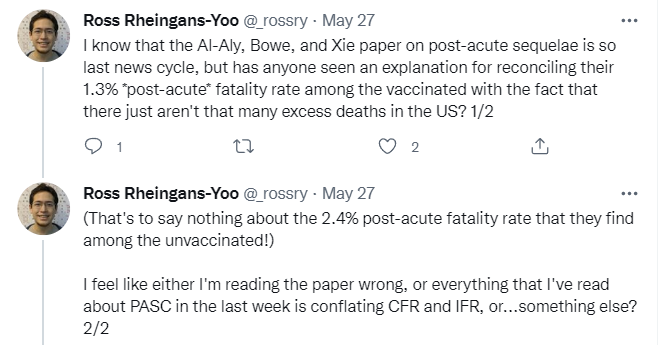
Whether or not this is something otherwise worth taking seriously, if the mean age in your study is 71 years old that’s an important point when deciding how to use the results of that study.
The Future
This was another light week for Covid news, and what news there is seems like it is largely repeating itself. If this continues, my current plan is to emphasize other things and also to start doing post-mortem analysis on prior posts, ideally starting back at the beginning - pulling out evergreen things to create reference posts, analyzing mistakes and things I got wrong, that kind of thing.
For now, I intend to keep doing the weekly posts as a public service - I keep an eye on things so you don’t have to.
Planned next post is a review of Talent, by Tyler Cowen and Daniel Gross. There’s a ton of specific detail there to talk about so it’s getting long, but I want it out there in the next few days one way or another. I had another thing planned for this week, but turned out I’d already written a version of it back in 2010, so no need to write it again.
Thanks again for writing these up. Between you and Naked Emperor one can save an absolute fuck-ton of crap to sift through, and I really appreciate it.
Honest question: Do we have any reason to read "COVID deaths" as "Deaths caused by COVID" instead of "Deaths with COVID?" if it is not explicitly written out in the report in question? I ask because I haven't seen any reason to do so from the beginning of the pandemic, and things like the "Total COVID-19 patients in acute care or intensive care" graph immediately jump out at me as saying "This isn't necessarily because they have COVID, but they just happen to have COVID and be there for whatever reason, including having COVID." Maybe I have just been an academic too long and cynically assume that if they could say "They are there because of COVID" without lying they absolutely would, but instead word it so you could be mislead to make it seem like a more important result than it is. (That's about 90% of conference paper presentations, right there.) Is there some reason to believe it is not just misleading with statistics and language?
Kristen Fortney (the CEO quoted in that article about aging) is Good People and the absurd journalistic framing is not her fault. It's just good sense to use COVID-19 as a timely application for the geroprotective drugs you've been developing anyway since before they were cool.
The COVID-19 drug they're working on is a prostaglandin receptor antagonist. https://en.wikipedia.org/wiki/Prostaglandin_DP1_receptor
Very roughly, this blocks the "bad kind of inflammation" (more allergic-like, Th2-ish, mast cells, eosinophils) that becomes more common with age and chronic disease and makes old sick people less able to fight off infection. It's totally plausible that targeting PTGTR1 would be good for COVID-19, other infectious diseases, and maybe even as a preventative for the healthy elderly.
My guess is that it's not very root-cause-y, and thus might not do much for other chronic diseases of aging or overall lifespan, but infectious disease is a leading cause of death in the elderly so it's pretty high impact even if all it does is keep old people from dying of pneumonia.