

Covid 7/15: Rates of Change

Cases rose by over 60% in America this week, and we’re seeing large jumps in cases around the world. I am highly suspicious about the jump in the rate of increase, but Delta certainly seems to be the real deal, and this was well above my expectations.
I worry that recently I’ve lacked sufficient skin in the game. Everyone I personally care about is vaccinated or young enough that they don’t need vaccination, so the real sense of danger is largely gone. The worry is about the reaction to Covid, rather than about Covid itself. But that’s a very real danger, and I have back that sense of ‘oh no, things could go very wrong’ because there’s the danger that we really will blow up our way of life over all this, and go into a permanent dystopia of sorts. That’s what we need to ensure does not happen.
Thus, the bulk of this post is a numbers analysis trying to figure out what we know about Delta’s transmissibility and the effectiveness of vaccines in reducing that transmissibility, using data from a variety of sources. Others are encouraged to continue this analysis and try to get to the bottom of this.
So let’s run the numbers.
The Numbers
Predictions
Prediction from last week: Positivity rate of 3.3% (up 0.4%) and deaths increase by 7%.
Result: Positivity rate of 4.8% (!) and deaths increase by 15%.
Prediction for next week: Positivity rate of 4.7% (down 0.1%) and deaths unchanged.
The null prediction is always an option, here two distinct null predictions with distinct reasoning. For deaths it’s clear that there was a reporting gap as predicted, so I do not think the death rate last week represents things getting worse, but they likely should start to get worse given Delta is deadlier and cases have stopped dropping within the required time window, and it doesn’t seem like last week’s number was too artificially high.
The case number is trickier, as there’s good reasons to think the data is distorted, either by July 4 or otherwise:

That giant spike represents going from an average of 2.6% to an average of 5.0% over two days. That’s not a thing that should happen to seven day averages. If it does, then the next five days things should continue to rise as old data cycles out for new, but that didn’t happen so far.
Perhaps July 4 was truly a superspreader event in the way that previous holidays were almost always underwhelming, as much as the previous holidays make that seem unlikely. Perhaps it’s a giant delayed data dump that didn’t include negative tests. It is hard to say. What I do know is that either things were worse than this before the jump and the low number wasn’t fully real, or the jump and new number are not fully real - one of these two numbers is misleading.
Thus, we have the standard question when a number seems to clearly overshoot, where it’s unclear where the ‘real’ number is and how fast it’s moving, so it’s unclear where it will end up. In this case, substantial real growth seems almost certain, and I definitely feel like the null prediction here is ‘chickening out’ but I’m not sure which direction to go, although I notice I’m more comfortable predicting a small reversion than an increase, while noting that such a decrease wouldn’t be ‘real.’ Thus I’m choosing a very small decline, with discussion continuing in the cases section and the Delta section, but this data doesn’t make sense.
Deaths
DateWESTMIDWESTSOUTHNORTHEASTTOTALMay 27-June 252783811704562991June 3-June 97208179154312883Jun 10-Jun 163686119613142254Jun 17-Jun 235294438312632066Jun 24-Jun 305504597061861901Jul 1-Jul 74593296121281528Jul 8-Jul 145323986891451764

Cases
DateWESTMIDWESTSOUTHNORTHEASTTOTALMay 20-May 2633,89034,69448,97324,849142,406May 27-June 231,17220,04433,29314,66099,169Jun 3-Jun 925,98718,26732,54511,54088,339Jun 10-Jun 1623,70014,47225,7528,17772,101Jun 17-Jun 2323,85412,80126,4566,46469,575Jun 24-Jun 3023,24614,52131,7736,38875,928Jul 1-Jul 727,41317,46040,0317,06591,969Jul 8-Jul 1445,33827,54468,12911,368152,379

Cases are up by 66%, and the positive test rate is up by 65%, which implies the number of tests was constant.
The more I think about this, the less sense it makes.
If cases were up by anything like 66%, why aren’t we running more tests? Aren’t people testing in large part based on whether they suspect they have Covid, and whether they have symptoms or known exposures, which both should be up a lot? Are we somehow supply constrained on this, despite no observations of difficulty in getting testing done on demand? How do these numbers make any sense?
Thus, I come to the conclusion that the numbers don’t make sense, and don’t belong in the same universe. If cases double test counts should rise a lot, and that not happening is super weird.
For now, I’m going to mostly ignore the test percentages and act as if the raw positive test counts are more accurate, because if there’s one thing I definitely don’t believe, it’s the reported number of negative tests. That doesn’t make any sense no matter how bad things are.
One possible way for this to kinda sorta work is that perhaps there are people who get tested in order to show a negative test, whose tests get reported every time, and people who get tested because they want to actually know if they have Covid, who mostly only report when they’re positive. Then, doubling the size of the second group doesn’t change reported test counts much? That’s the best I can come up with.
What should we make of the 66% rise in cases? How much of it might be timeshifted and in what ways? Is this a fully real rise, and should we expect it to continue? If so, what happened?
Discussion of all that will continue in the Delta section, where I attempt to reconcile all the various different data points.
Vaccinations
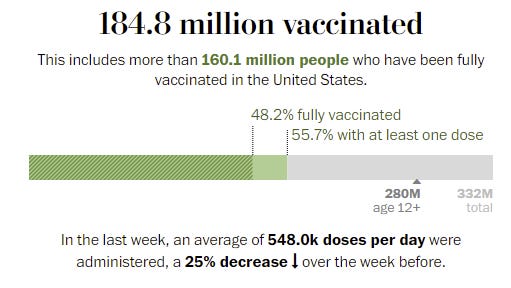
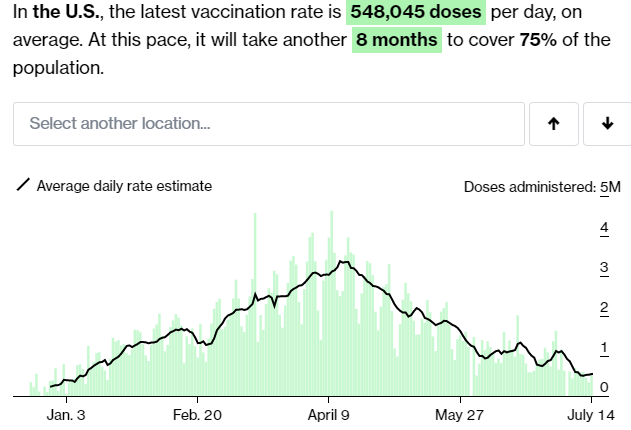
Given no attempts to halt the course of events, this is a strong result.
There’s a new warning on J&J shots (WaPo), because there were about 100 detected cases of an autoimmune disorder out of 12.8 million shots. There was one (1) death involved, again out of 12.8 million shots. It will be an interesting control group for the previous experiment where J&J got suspended. If we take a side effect that doesn’t matter, and treat it like it exists but doesn’t matter, does that have an impact? Versus treating it as a huge freaking deal and freaking out everyone and suspending the vaccine, which we are pretty sure had a fairly large impact the last time there was a side effect of magnitude epsilon.
New paper says that neither ‘give people fact box’ nor ‘explain how mRNA vaccine was developed and that it wasn’t too fast’ impacted vaccine hesitancy. Kudos for publishing the negative result. Why aren’t we seeing a lot more studies like this of various things one might do?
Then there’s the question of what is happening in Tennessee (news article).

The explanation I found was that in Tennessee teenagers can get vaccinated without ‘parental consent’ and this was creating problems. Which does not seem like much of an explanation, as there’s no reason why such consent should be required or even relevant. And certainly does not explain why this applies not only to Covid-19, but to all vaccinations period. Or why they think it makes sense to strip teenagers out of lists for reminder postcards if they’re scheduled for their second shots, but focus on the other vaccines part of this, if you’re considering that this all might have a perfectly logical explanation.
Perhaps we can at least partially salvage this by taking advantage of the ‘natural experiment,’ and observing what happens to vaccination rates. Do the reminder postcards do anything? What about the other things that got suspended? What happens to the vaccine rates for other diseases? If you can’t go with ‘prevent people from getting sick and dying’ you can at least upgrade your world models.
Genius in France: Incentives Matter!


The second day exceeds the first, so those 2.2 million appointments are likely only the beginning. It’s one thing to pass up a vaccine, it’s another to pass up the ability to participate in many aspects of life. Make no mistake. If implemented, this will work.
If America’s Delta problem gets sufficiently worse that they start bringing restrictions back, and they don’t start requiring proof of vaccination in such situations but instead once again halt life for the rest of us, I call upon all of us to find this completely unacceptable, the same way I find permanent child masking unacceptable.
In such a scenario, there are two sane choices. You can either let people do what they want, or severely restrict what the unvaccinated can do. Ending life as we know it, presumably indefinitely, shouldn’t be even potentially on the table, nor should we have any tolerance for such proposals.
Delta Variant
A post entitled Delta Variant: Everything You Wanted to Know does make a real attempt to be exactly what it says on the tin. The graphs are rather cherry-picked to make things look as bad as possible, as are a number of other discussions, but the data is all legitimate. The question of the day is now exactly how bad Delta is and making sure our models of it are right to figure out what is to come. There’s a bunch of superficially contradictory data that must be reconciled, as there usually is.
Taking stock of those data points is the logical first step.
Israeli Data
Israel offers the scariest data point, suggesting greatly reduced vaccine effectiveness.
I’ve seen the Israeli data presented in slightly different ways but this is basically what they’re reporting there. I’d like to note that the story doesn’t make sense, even on its own.
For previous strains, this is saying that vaccination wasn’t protective against hospitalization, and mostly wasn’t protective against death, once someone was infected (93% reduction vs. 93% reduction), or at least once someone tested positive. We knew even then this wasn’t remotely the case.
Then with Delta we get this gigantic drop to 64% protection against infection, but then protection against hospitalization stays at 93% and protection against death rises? So conditional on infection, this is saying hospitalization protection went from ~0% to 80%? Really?
Even the 79% number seems very very strange when looked at this way alone.
You could tell a story that justifies it. In that story, vaccine protection works 96% of the time (and there’s measurement errors), and if that happens you’re protected against severe outcomes no matter which variant you face because that wasn’t a close call, but being infected at all is a lower threshold. Before, if you were successfully vaccinated you basically never got infected (in this model), whereas now if you are vaccinated you sometimes do still get infected, but it’s never serious whereas before it never got that far in the first place. Then there’s the 4% of people for whom the vaccine doesn’t work properly, who are still at real risk. Or something like that.
As a sanity check, what happens if we ignore the reports and attempt to back out the answer from the raw data on infection numbers?
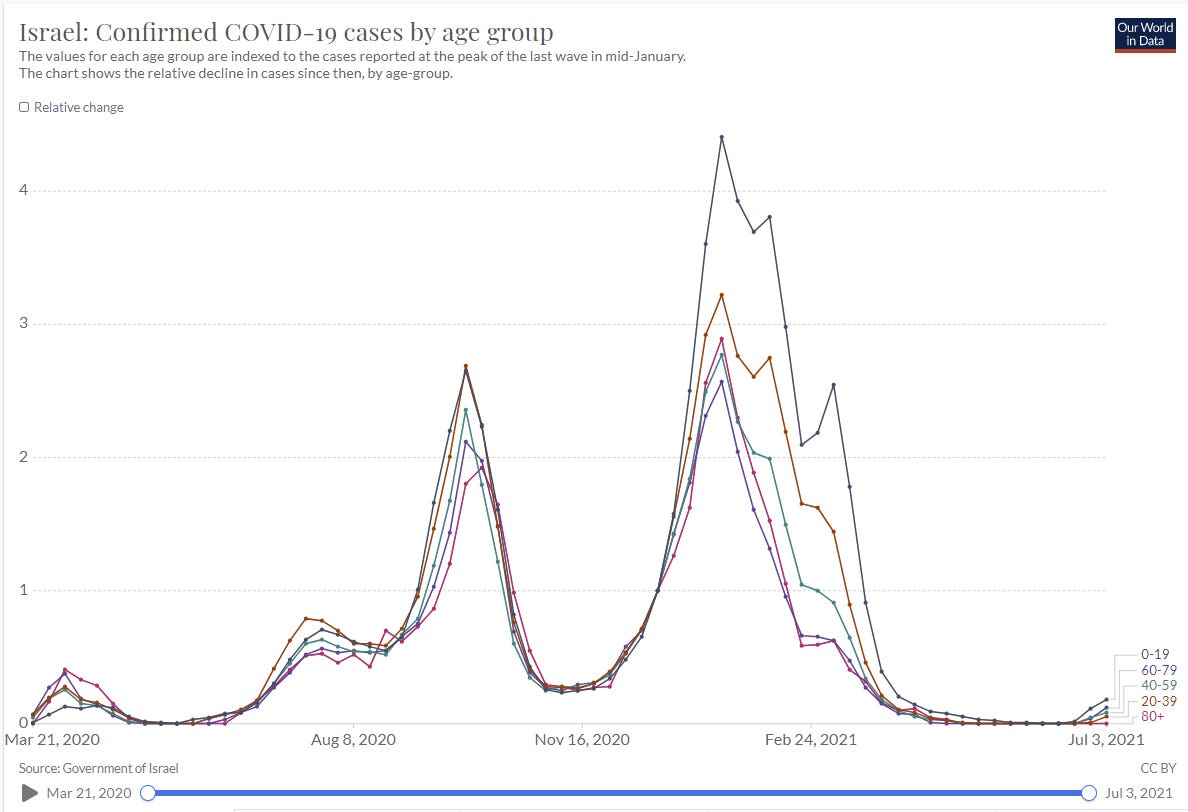
That’s not a picture one can easily read, so click the link if you want to examine it.
Reminder:
There are a lot of confounders, but let’s start with the pre-vaccine comparison.
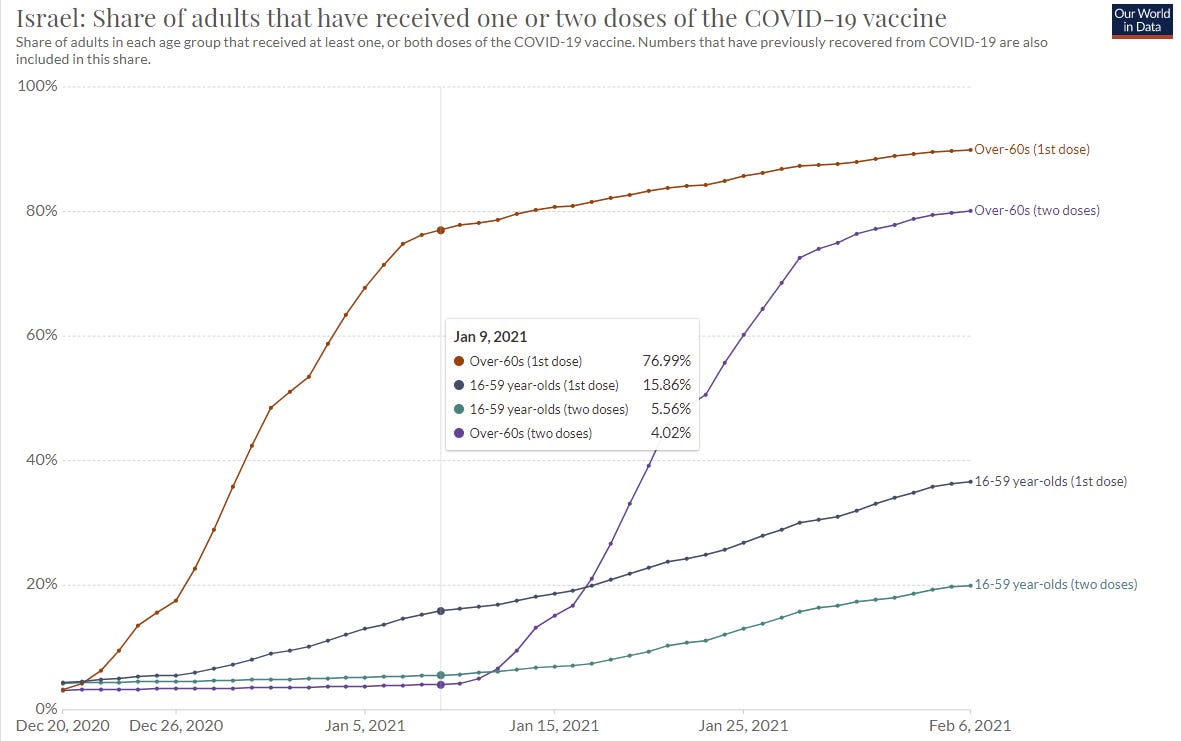
Next, let’s do a pre-Delta comparison, from when the numbers were very low, but people were mostly vaccinated:

Consider this a ‘post-vaccination’ equilibrium. Many of the young aren’t vaccinated, whereas most of the old are, so the ratios change, but almost entirely for the youngest group. Things were mostly level before otherwise, and remain mostly level now, in roughly the same order.
Now let’s look at the last day they have data for here:
It’s unfortunate we don’t have the July 10 data, but we go with what we have. This still has to represent almost all Delta cases, and gives us apples-to-apples comparisons. What can we infer from these numbers?
Also, how does this reconcile with this graph?
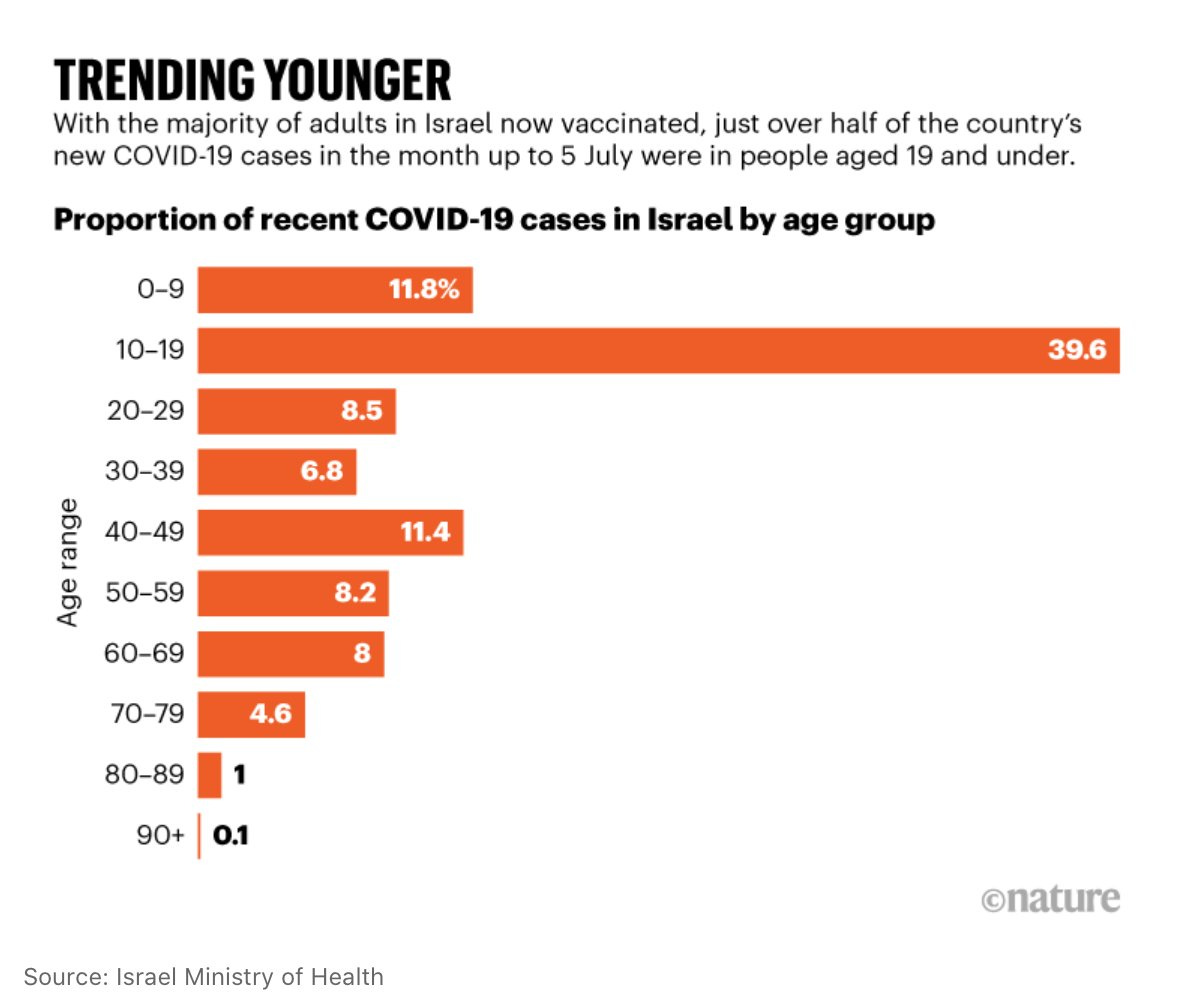
Israel is young, but it’s not that young, and my response to the above graph is more like ‘those sample sizes are all absurdly small because Israel didn’t have Covid that month.’ Still seems difficult to reconcile in the details, but easy in the bigger picture.
My conclusion is mostly that this is muddled enough that I can’t draw a fixed conclusion. Especially weird is the 60-79 range. One possibility is that the vaccine needs a threshold of effectiveness to prevent infection, and it’s still mostly good enough to hold off Delta, but those with weakened immune systems are in a different situation and they are mostly very old? But the share of vaccinations in such groups is still super high compared to younger groups, and the order of these groups still seems really odd. It would, however, explain how 20-39 could be the lowest major group while 0-19 is the highest, perhaps - The kids in their 20s can still largely get vaccinated, and their immune systems are still strong, so it’s highly effective? Whereas with the 40-59s it’s less effective especially on the high end, and so on.
We should also look at case counts in Israel. On June 18 they had 1.92 cases per million, right before things started rising, on June 14 it was 65.09, for R0 = 1.97. From previous data, we can presume that when Delta was a very small portion of Israeli cases, the control system adjusted things to something like R0 = 1, so we’ll keep that number in mind.
UK Data
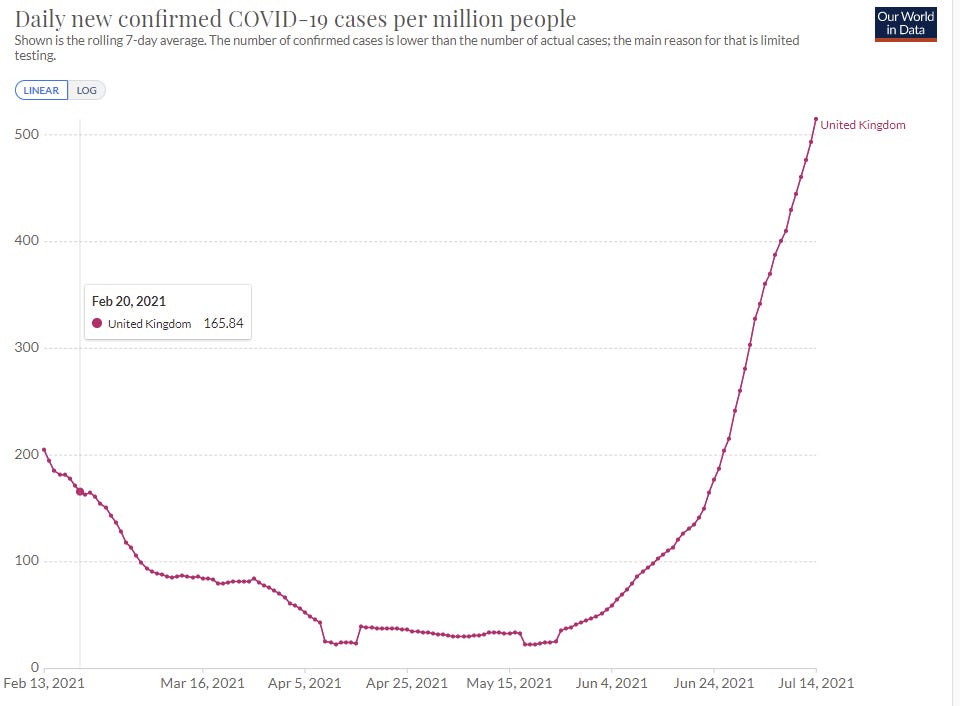
We can presume that Alpha hasn’t increased its absolute numbers, so at this point UK is almost all Delta. On May 25 there were 35.7 cases per million. On July 14 there were 512.9, On July 4 there were 361, so the two-week R0 = 1.19. From May 25 to July 4 we get R0 = 1.32, despite a bunch of Alpha early on, so the control system has been adjusting, but also we never see a period with an extreme R0 in the UK. In April, they had Alpha and things were stable (R0 ~ 1). For an extreme situation, let’s look at relatively early lift-off of Delta and assume a base of about 30 Alpha that doesn’t count for growth rate, and start when total cases are at double that, or 60, which is June 4. Over the next 10 days things went to 107, so let’s say that this represents Delta going from 30 to 77, before much adjustment has been made, over two cycles. That would give an estimate of R0 ~ 1.60, on the high end of the range for increased base transmissibility. It doesn’t leave that much additional room. One more cycle gets us to 131, which would be R0 ~ 1.31 for Delta alone, so presumably there were adjustments being made already then.
Transmissibility
There’s the question of how much more deadly Delta is than older strains, but I’m mostly going to ignore it because it doesn’t impact the path of the pandemic much. The question is containment versus lack of containment. If Delta is twice as deadly, that’s quite bad, but it’s an isolated question. As commentators have pointed out, the data supporting the increased deadliness is not that solidly grounded. The extra viral loads are suggestive, and the early data does look like it’s more deadly for a given unvaccinated person, but our data remains not great.
The much more key variable is transmissibility of Delta versus Alpha or the original strain. I’ve been using a 120% increase, or 2.2x (220% of original infectiousness) for Delta, and a 1.4x (140% of original) for Alpha, which continues to match estimates I’ve seen. Those all presumably refer to transmissibility among the unvaccinated and ignore the vaccinated population, and I’ve been treating the numbers accordingly. I see no reason to change that methodology, but that means that we need to reconcile our numbers with the case counts that we see.
An open question is how tight the bounds are on such numbers. If we have a model where things were previously going fine and then you ‘multiply by Delta’ then the bounds are reasonably tight. However, if you think that behaviors are adjusting in real time and seasonality causes ‘random looking’ ebbs and flows naturally, then there’s room for the data to look highly misleading, and my position at this point is if anything is closer to that second view.
Either way, your model has to make predictions whose math checks out, and that’s a good place to start.
Let’s say we accept that Delta’s ‘multiplier’ is 2.2, versus the old baseline, and Alpha’s is 1.4. Now let’s suppose vaccine effectiveness is reduced from 95% to 65%. What happens? Given current vaccination rates, with an adjustment for children, that’s about another 50% increase in the rate of infections.
That would mean that Alpha to Delta is a full effective +120% increase in the rate of infection, on top of the increase from original to Alpha, or a final factor of around 3.3. Or, alternatively, it would have a ‘base’ R0 of something like 6, with a vaccine that only reduced that for the vaccinated to 2, which would mean that even in fully vaccinated populations this would double every five days under pre-pandemic behaviors.
Set aside for the moment the question of what we would want to do about that. How does it line up with the data?
In the UK, where the Delta problem is currently largest and we are confident Delta is essentially the whole pandemic (using Our World In Data as my source), we had 36 cases/100k on May 25, and 494 on July 14, 52 days later, or just over 10 cycles, and R0 ~ 1.28. During April and the first half of May, we saw the number of cases stay roughly constant within a factor of 2, so R0 > 0.9. We could factor in some increase in vaccinations, but if Delta taking over sent R0 from 0.9 to 1.28, that’s only a 42% increase, similar to what we’d expect from Delta taking over from Alpha, minus some existing more infectious strains and some extra vaccinations, give or take behavioral adjustments and seasonality.
None of this matches the greatly reduced effectiveness hypothesis, unless you presume that behaviors are substantially adjusting during this period, but the shape of the curve isn’t suggestive of that either.
American Data
In the last week, America has seen a 66% increase in cases. As discussed above, going +10% then +20% then +66% is extreme, and can’t be explained by Delta alone. The share of Delta cases can only rise by about 30% in one week, even under extreme assumptions (e.g. from 35% to 65% or something like that, would be the theoretical limit) so a +46% effect in seven days off a 30% rise would mean Delta was at least twice as transmissible as Alpha. It also means the numbers in previous weeks would have shown a bigger problem, since the displacement of Alpha by Delta has to be gradual - there’s no way there was three times the growth in Delta this week that there was last week, because math.
Overall, though, the number isn’t crazy - if we presume that the control system had already adjusted for our vaccinations and for Alpha. If we take the +66% number seriously, and compare it to the pre-Delta situation, it’s safe to presume that we had previously stabilized under a full-Alpha situation, then +66% in a week represents a 43% rise in transmissibility from Delta versus Alpha minus any extra vaccinations, so 50-60% total, which doesn’t even leave room for the vaccines to lose effectiveness since that’s our estimate range for Delta already among the unvaccinated.
Under such assumptions, we can backchain, and it matches up with the sample data claiming that by percentage there wasn’t much Delta running around in early June, despite Delta now having taken over and now being 85%+:
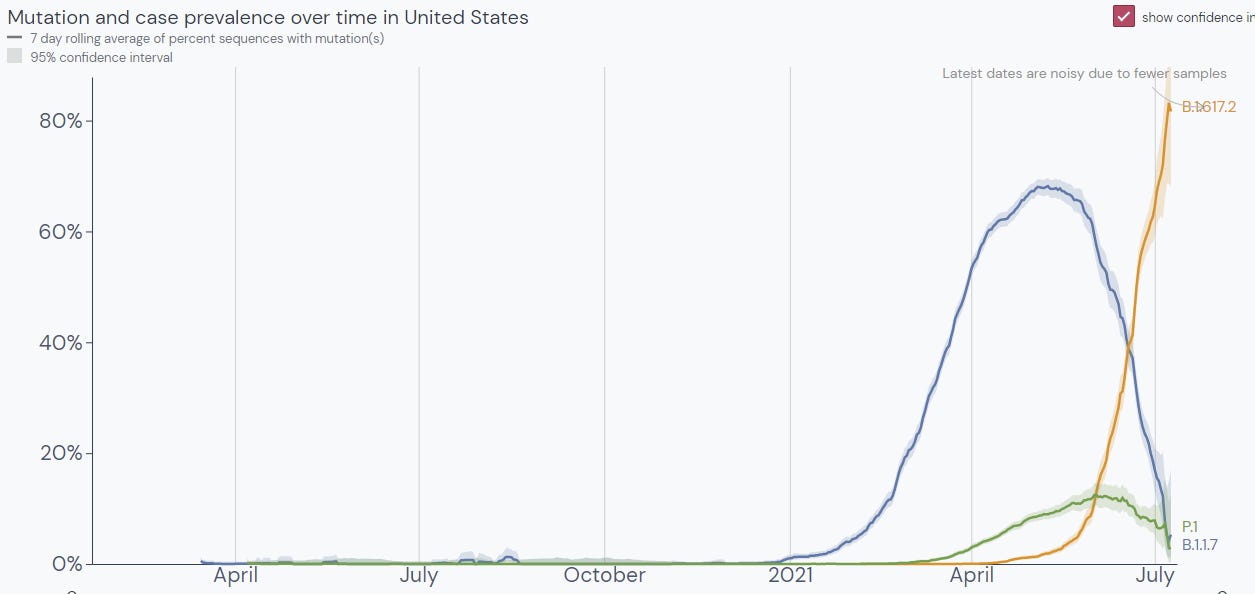
An alternative calculation would be to look only at Alpha, or to compare Alpha to Delta. We have a percentage for it, so we can back out its growth in absolute numbers. It was something like 60% of cases on June 15 by this graph, and is now down to 5%. Whereas Delta went from roughly 4% to 85%.
From June 15 to July 15 is thirty days. Thirty days allows for six serial intervals. So if all of that is accurate, we get a ratio of 2.5:1, or +150% increased infectiousness, which is even higher than the +120% estimate for the full effects previously measured. We then look at absolute numbers, and see Alpha having an R0 = 0.75 over this period, versus R0 = 2.25 for Delta. Which would mean that both we’ve taken a lot more precautions recently than we did before to get things that low, and also that Delta should be doubling every four days, yet cases over the last week only rose by 66% despite starting off with the majority being Delta.
Thus I don’t believe the chart above is a representative sample - the math doesn’t add up.
One can have a hypothesis that strains crowd each other out in some sense but I don’t think the base rates are high enough for that effect to be big right now.
Then again, as I’ve been noting, if you take the numbers too seriously (as in, you don’t think there are big hidden factors and random distortions) then none of this adds up.
So where does that leave us? Can we put bounds on things?
Our lower bound should presumably be that Delta is 50% more infectious than Alpha, but that vaccine effectiveness is mostly unchanged.
Under Israeli conditions, it seems mostly safe to say that Delta is at most twice as infectious as Alpha, but that about twice is possible. This is the scariest data set.
Under UK conditions, it seems mostly safe to say that Delta is at most 75% more infectious than Alpha, and it would be difficult to get to a doubling.
Under American conditions, it seems mostly safe to say that Delta is going to be less than twice as infectious, given everything we know - the math starts to fold in on itself if we get above 75% or so, in the sense that things need to look much worse than they do. I’d put a soft bound around 75%.
We could also look at any number of other places. Israel and UK are especially picked because they’re well-vaccinated and having trouble.
Now let’s look at vaccination rates. Using Bloomberg’s ‘enough for X people’ metric, Israel is around 60%, the UK is also around 60%, and the USA is at 52.4%. That’s out of the full population, which includes children, so effective vaccination rates are somewhat higher especially for Israel (which has a younger population), and one dose is more than half of two doses, so the USA is effectively closer to 60%, and we can put Israel and the UK closer to 67% in terms of our effective percentage.
Let’s presume that in the base case, vaccinated people are 96% protected in terms of transmission. If we presume that the unvaccinated transmit at a 50% higher rate, but that the effective increase is 100% in Israel, that would give a vaccine effectiveness versus transmission of 67%. If we take the UK and presume 75% increased transmission, that implies vaccine effectiveness versus transmission of 80%. For the USA, a 75% increase in transmission would imply 76% vaccine effectiveness versus transmission.
It is possible, in theory, that this difference could be that vaccine effectiveness against transmission fades somewhat over time, and the difference here would be that Israel vaccinated earlier than other countries did.
If things were instead at our lower bound, by assumption, vaccines would remain at 96% effective.
It’s really hard to put bounds on things given all the factors we can’t account for, including control system adjustments in both directions, seasonality, and so on and so forth.
These are likely not tight bounds. There are likely a lot of behavioral adjustments involved in all of this. But it’s all very noisy, and I haven’t seen other serious attempts to figure this out. I’m encouraging everyone to take a stab at this from various angles and see what you find. There’s tons of data to work with.
If this reduced effectiveness is near those upper bounds, there is a very large problem. Even fully vaccinated populations wouldn’t be able to fully return to normal if you wanted to avoid Covid outbreaks. You’d either accept that vaccinated people and children often get Covid, and it would be fine, or you’d need to impose restrictions forever, or you’d need to get a new more effective vaccine distributed in the form of booster shots. And that’s if you got close to 100% coverage, which is not going to be happening.
Thus, the question would become, if Covid is not done with us, can we decide to be done with Covid and that life beckons, or are we actually going to kill our civilization and way of life over this despite having a vaccine that renders Covid mostly harmless?
In Other News
Fox News has generally not been as anti-vaccine as its customer base likely would have preferred, but some evidence that this may no longer be true. If I have any regular viewers reading this, can you update us?
Reasonable thread laying out different questions surrounding booster shots, which oddly still leaves out the question of whether shots can be modified to work better versus Delta. I’m confused why there isn’t more discussion about that. My presumption is that modifications wouldn’t help, which is interesting in and of itself and seems worthy of mention if true.
Deal between Israel and South Korea where Israel gives Pfizer shots now that it couldn’t use and were going to expire, gets future shots in exchange because selling things for money is evil. Post (from MR) points out that Covax’s quest to allocate vaccines equally is going to end up wasting a lot of vaccine, as many places don’t have the means to distribute the shots they’ll get.
Moderna begins a trial for yearly mRNA shot that would combine vaccines for flu, COVID-19, respiratory viruses RSV and HMPV. It turns out that not only does mRNA allow us to cure a wide variety of diseases, it lets us cure all of them at the same time, because the technology allows the payloads to be delivered together. I’d be a little concerned about short term side-effects similar to the ones with the current Covid vaccine, but my hope is that the problem can mostly be solved by proper dosing.
This is also an excellent way to give people Covid booster shots without everyone freaking out. If one shot, once a year, can deal with a wide variety of problems, that should work great, so long as the misinformation from anti-vaxxers doesn’t cause too many problems.
New Zealand didn’t secure enough vaccine shots, which is unfortunate, but is taking the AZ -> Pfizer booster path seriously, which is great.
You don’t often get to pick your allies, such as in the war on school. Or is it the war on children?

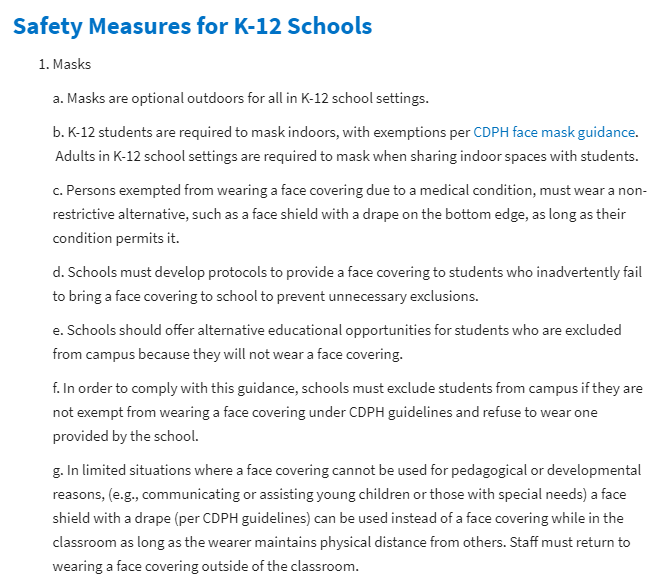
My understanding is this applies even to private schools, although good luck enforcing that. If they’re going to mandate this now, when will it end? Are they planning on keeping things like this forever? Or even going back to the torturous ‘remote learning’ at the drop of a hat?
What would it take to free our children? How bad would it have to get? Shall we run the experiment and find out?
A rant on the quest to establish that the lockdowns were always painless and super effective and that Everybody Knows this.
And some really are pushing to make the pandemic restrictions permanent. Who would want such a dystopia? (post)

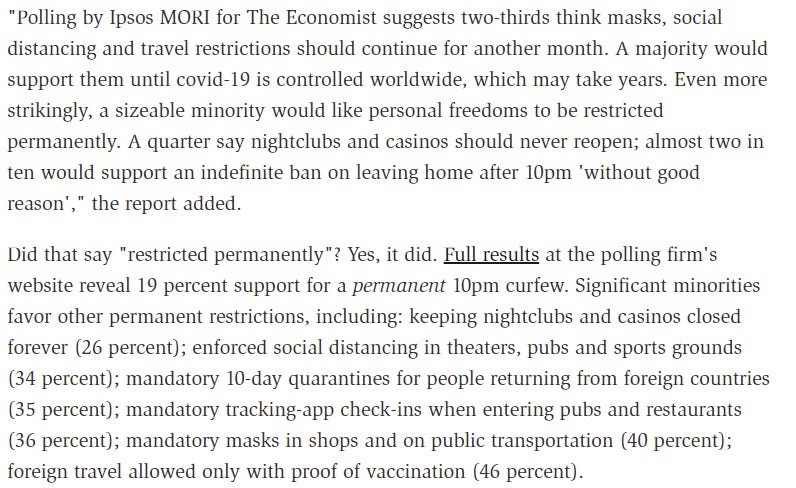
People permanently not being able to leave home after 10pm ‘without good reason’ is the kind of thing hack writers put into young adult novels. Or at least, it used to be. Then again, perhaps there’s always been a 10% share of people who shake their fists at ‘kids these days’ and actually want to be the villains in such novels. How much of this is new?
A quarter of people wanting to close casinos and nightclubs permanently (but again, how much of that has anything to do with Covid?)? A third of people favoring permanent quarantines for international travel? Tracking everyone who enters a restaurant, again, permanently? This is still less than half of people, but a third is a lot of people.
This is the fight that is coming, even if conditions are good. They hate us for our freedom. You gotta fight for your right to party.
One can still party a little too hard, even outdoors. Outdoors is much safer than indoors, but that doesn’t mean one can’t push the envelope too far:
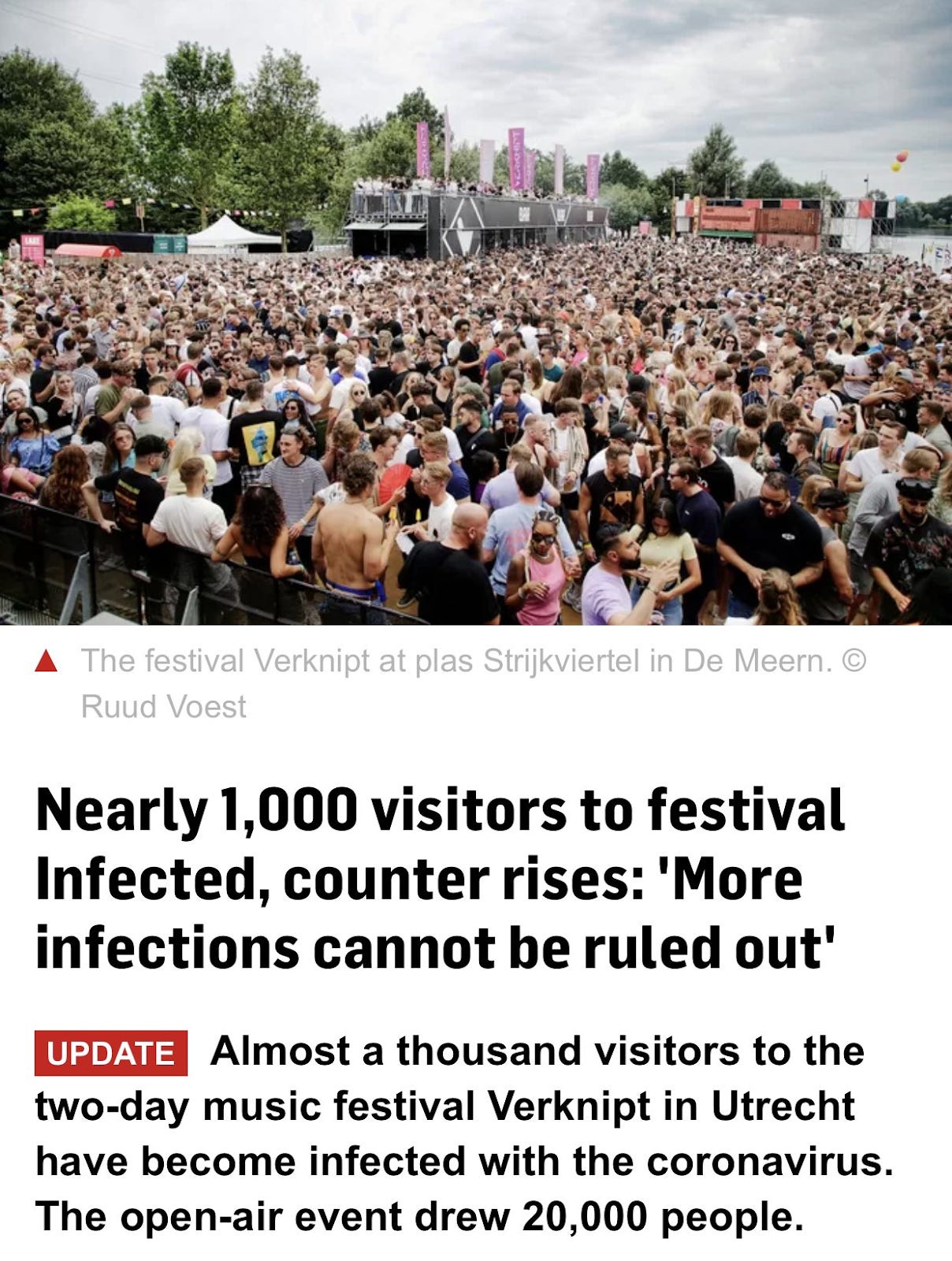
So yes, there’s mass gathering and then there’s mass gathering, might want to not do that second one. Also, ‘cannot be ruled out’ is technically true but I think we could have gone with something a little stronger. A thousand identified cases is not a thousand cases.
Or, alternatively, instead of protesting for left-wing causes, one can protest against a Communist regime, in which case your protest is dangerous:



Remember, whether or not something spreads Covid depends on whether it is approved of by the proper cultural authorities and Very Serious People. And this is what they think about protesting against authoritarian Communism.