

Covid 9/23: There Is a War

The FDA, having observed and accepted conclusive evidence that booster shots are highly effective, has rejected allowing people to get those booster shots unless they are over the age of 65, are immunocompromised or high risk, or are willing to lie on a form. The CDC will probably concur.
I think we all know what this means. It means war!
Don't get me wrong. The FDA has been hard at work for decades ensuring people die or twist their lives into knots from a lack of access to medicine. Refusing to acknowledge that there is a war doesn't change the fact that there is a war.
What changed this week was that the FDA gave us an unusually clear proof that there is a war, which side of that war they are on, and how far they are willing to go.
The good news is that, because of the exceptions, anyone who wants a booster can still get a booster, so on reflection this is a win-win. We know exactly what is going on, and it didn't cost us all that much.
The CDC is now meeting to consider who should have the ability to get booster shots, not withstanding the FDA already having made that same decision. And they are being explicit that the point of vaccination, according to the CDC, they are now claiming, is to prevent hospitalization and death and NOT to prevent infection.
Let me say that again. The CDC explicitly claims that it does not think it is an important goal of a medical intervention to prevent Covid-19 infections that don't result in hospitalization. Or, by implication, to prevent you from spreading the disease to others.
Tell that to all the people who see a mild infection somewhere vaguely around them, and quarantine for two weeks or shut down their office, and freak out. Tell that to all the people at the CDC mandating such behaviors. Tell that to all the people saying vaccinations are a social responsibility, or requiring it to engage in ordinary life activities. Tell that to everyone, at the CDC and elsewhere, warning us about 'Long Covid,' or suffers from it. Tell that to everyone who simply gets Covid-19 and has a really bad time for a week. Tell that to everyone around you deciding whether they can live their lives.
There. Is. A. War.
(As a weird aside, did you know their name is short for "Center For Disease Control"?)
Executive Summary
There is a war to preserve or destroy our way of life.
The FDA and CDC are on one side.
They have made it even more clear than before which side that is.
Despite their best efforts those who care will get booster shots. Technically the rule is six months after your second shot, and you have to be either over 65 or otherwise high risk either in terms of health conditions or your job.
Despite their best efforts 5-11 year-olds will get shots in a month or so.
Let's run the numbers.
The Numbers
Predictions
Prediction from last week: 900k cases (-5%) and 13,000 deaths (-1%).
Results: 815k cases (-14%) and 13,822 deaths (+7%).
Prediction for next week: 750k cases (-7%) and 13,800 deaths (unchanged).
It turns out the death jump was mostly real, while the small bump in cases mostly wasn't. It's odd that the errors here were in different directions, since that means it's unlikely both were primarily caused by holiday issues. I interpret this as a new normal of steadily declining cases (but not at this week's pace, because I think some of that was catching up to trend), which I expect to continue for a few months, after which Winter Is Coming and we may have an issue. Deaths should start dropping soon as well but there's no reason to think the peak will be sharp.
I heard on the radio that the CDC is speculating there may not be a winter surge this time due to background immunity levels, and I agree that it could go either way, and I'm not sure which is more likely so I must have this close to 50%.
Deaths
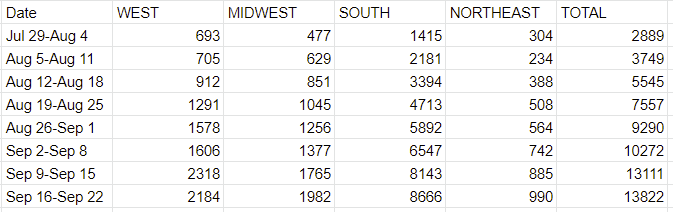
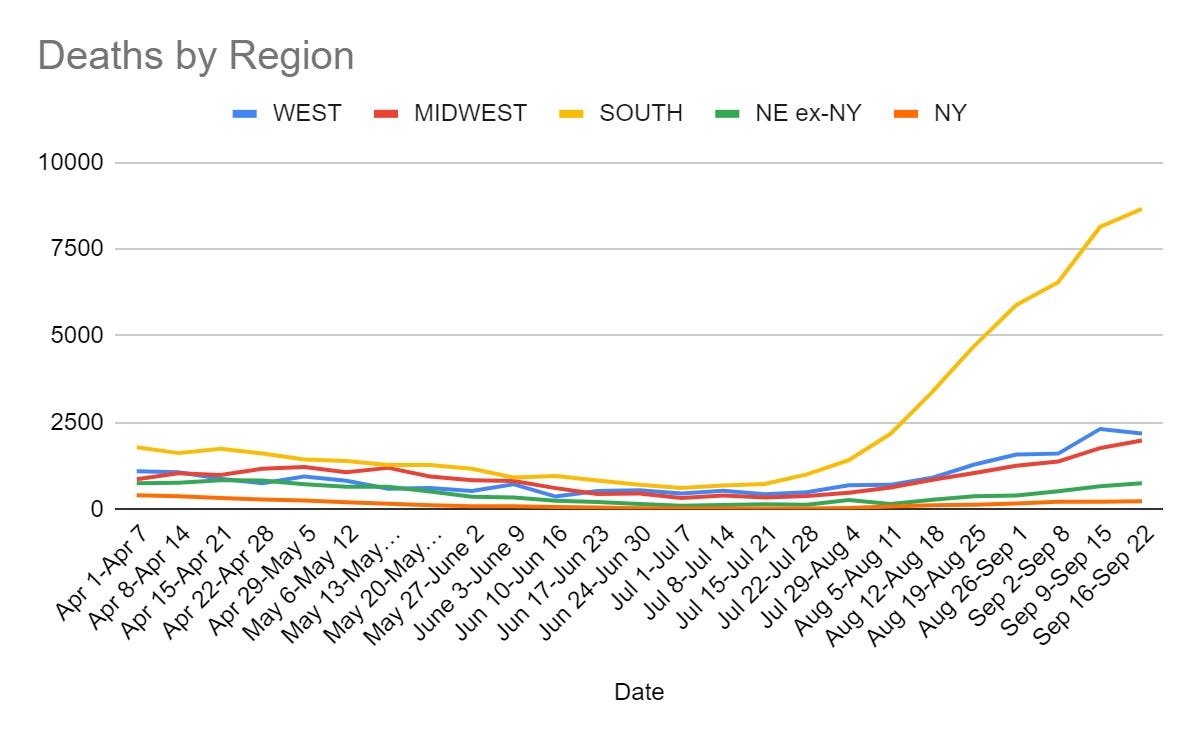
Cases peaked three weeks ago, so we should see this start to decline soon.
Cases
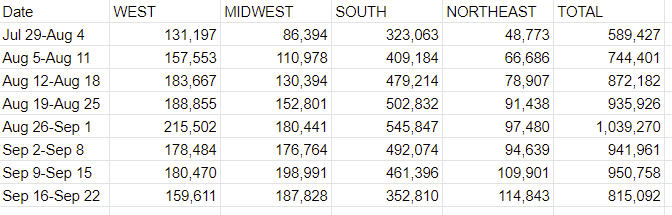
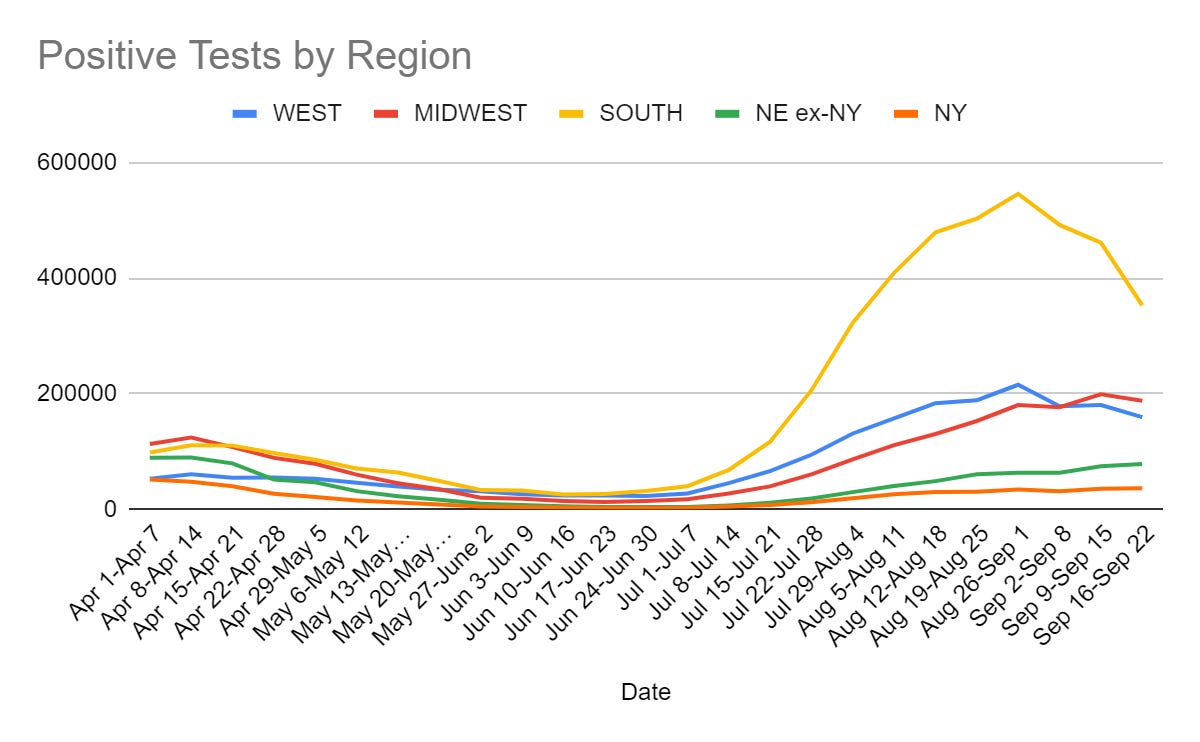
Cases still increased this week in the Northeast, but only a small amount and I expect that to reverse soon. Clearly this wave is now headed in the right direction.
Vaccinations
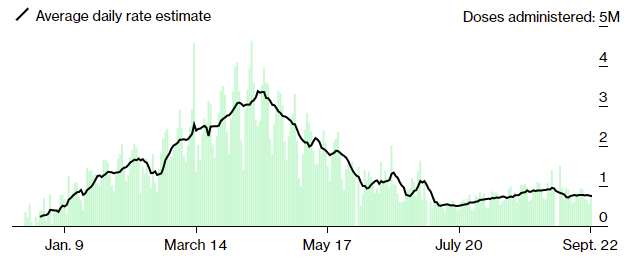

This represents only 272k first doses per day, which isn't much, although every little bit helps especially once we're already this far along. What's clear is that on top of FDA approval not doing much directly, the new mandates and pressures also aren't getting the job done, all they're doing (at most) is preventing a faster decline.
Then again, it turns out vaccinations aren't that important, if we were to listen to what the FDA and CDC have to say when thinking about booster shots, so by their accounting it should all be fine.
Vaccine Effectiveness
Vaccines work for 5-11 year-olds, with a reduced dose of 10 micrograms. Everyone is so excited they hope to get this approved by the FDA in a month, maybe six weeks if it slips a bit. There's nothing that's going to happen to kids during that month due to everyone freaking out about them not being vaccinated, so it's fine. Zero cases in the trial of any serious safety concern, which makes sense given there were only a few thousand kids, so I don't really know what anyone was expecting or learned there. Here's hoping this is accurate, combined with the booster shots anyone who cares enough will find a way to get:
I'd post a Padme theme about partial doses in adults, but I grow tired.
Two doses of J&J are 94% effective against symptomatic infection. So this whole time we've literally been stopping after one shot of J&J but doing two shots of mRNA, and that was the entire difference the whole time.


How old are these studies? They're old enough that they're explaining the 94% vs. 79% difference by pointing to the American arm not involving Delta cases, as the data came from June and July. Which is confusing to me, because the majority of the cases in June and July in America were Delta, and 94% represents fully robust protection, so if Delta knocked this down to 79% then there wouldn't be room for much Delta at all. This is a rather large difference to explain, so I looked at the paper via the stat article on this. Looks like the period measured started on the day of vaccination, whenever that was, so the bulk of cases included periods stretching back months, and in America there weren't that many cases in June and July versus earlier in the year, so the whole thing does mostly makes sense except for the part where we're only hearing about this now. Oh well.
This was the most convincing piece of evidence I've seen so far, by a wide margin, that vaccine immunity is indeed substantially lower against Delta. The differences here are large, it's in a properly done study with every incentive to find the opposite, and I don't think it matters that it' the J&J vaccine here rather than mRNA. I'm much more confident the drop-off here is real, and that for mRNA we're looking at levels in the low 80s without a third shot.
That's distinct from the question of waning immunity over time, which I mostly consider to probably be a statistical artifact.
But no matter in either case, because luckily, those booster shots are on their way as soon as the FDA approves them, and our lives won't be thrown into chaos once more as everyone freaks out about all this.
Oh. Wait.
FDA Recommends Technically Banning Most Booster Shots
When there is a war, it is the good and honorable thing to declare war. Then all involved can respond accordingly. Before I get to the details of what happened, I want to thank the FDA for properly following the formalities. The FDA is remarkably good, once it can be bothered to examine the evidence, and to the extent that it considers such evidence to be 'admissible' in its court via being in the proper form and done with the proper permissions, at presenting that evidence fairly and drawing the correct logical conclusions.
Which is great. I really do appreciate it. I'd much rather they honestly analyze the evidence and make their decision anyway, rather than manipulating or misinterpreting the evidence to justify their decisions.
Anyway, last week a commentator took on the time and mental health burdens of observing the FDA meeting so the rest of us didn't have to, and created this excellent summary of what happened. I want to stop and say: Thank you.
It's quite long, but it's pretty great, so if you want further detail, please look there. I'll hit the parts I consider most relevant.
Before we look at what happened, since the linked post mentions it up front, it's worth tackling the question of the booster shots given here taking shots away from people in other countries. I have two responses to that, which are essentially:
They aren't doing that.
That's none of the FDA's damn business.
It's a policy question, not a regulatory one. It's none of their damn business the same way that this is most definitely none of their damn business, but is such people's favorite thing, scaring people and especially kids, while avoiding their least favorite thing, letting people have medicine.

My model strongly says that if boosters aren't allowed at this time, we're not going to take the booster shots we would have given and ship them overseas. We're instead going to let them sit around until the expire, on the hopes that we'll find a way to get boosters approved, or that enough people realize they can mark a box on a form and get a booster anyway. Prove me wrong, kids.
But even if I'm wrong about that, that is, as I said, none of the FDA's damn business. The FDA's damn business is whether the booster shots are safe and effective or not.
All right, enough on that question, on with the show. There was a bunch of data presented. Here's the first thing he notes.



I didn’t scrutinze each of the 53 pages, but it seems they wanted to draw 2 major conclusions:
A Kaiser Permanente of Southern California study showed vaccine efficacy waning (Figure 1, p. 12, makes this point, but slide CC-13 of their presentation [6] makes the point better and is reproduced here: the right plot shows sustained efficacy versus hospitalization). I’m glad they honestly say that efficacy against hospitalization and death remained high (mostly > 90%). So that’s sort of wanting to have things both ways: yes, efficacy against any infection might decline (though they don’t seem to be aware of Simpson’s paradox!), but the efficacy we care about is still robust. Hmpf.
A 3rd dose does indeed boost the geometric mean titer of antibodies, against both the wild-type and B.1.351 (Beta) variants (Figure 2, p. 19, makes this point, but slides CC-22 and CC-23 of their presentation make it more graphically, and include Delta). The rise after the 3rd dose is statistically significant, as shown by the confidence intervals. The 3rd dose is the rightmost 2 pairs of bars in each group. Note the vertical scale is a log scale, so these are really huge differences.
So… yeah, it works. But the evidence of need is slightly sketchy.
The FDA slide deck makes substantially the same points. [7] There’s some slightly subtle foofraw about noninferiority criteria according to the 97.5% lower confidence limit of the difference of… something or other. But the details here are unlikely to be of broad interest: the game is to make sure the 3rd dose doesn’t harm immunity, and after that it helps.
Is it that easy? Do boosters clearly work? Yes.
Ignore for the moment the question of waning immunity, and focus on the second point. This boosts your immune response level by an order of magnitude, which is known to have a very large effect in your vulnerability to Covid. That's not comparing to immunity that's faded over time, it's comparing to one month after dose two. So it's clearly much better immunity than two shots alone. It works.
Then there's a bunch of arguments over whether immunity is fading, and I'm confused as to why we should care.
Let's say that the two-shot regime was still considered a full 96% effective versus infection and 99.5% versus death. And let's be conservative and say that the third shot boosted that to 98% and 99.8%. In what way would that not be effective? How are we not moving on to discussing safety?
If your answer is '96% is good enough' then please, I beg you, take a look around. Look at what the people who are vaccinated are still doing in the name of prevention. Look at the things they're being told they have to do, and the worry and stress they go through each day. We can cut all that in half here, with one shot, far less than half as obnoxious as all that other stuff, and also stop the general spread that much more. These are the same people who talk endlessly about how awful it is to not save every life you can, no matter the cost. How is this even a question?
These people are telling us to suspend our way of life indefinitely to get extra protection, while simultaneously telling us that we don't need additional protection from a booster because what we have is good enough.
So what's the question? This is the question:
Question to the Committee
Do the safety and effectiveness data from clinical trial C4591001 support approval of a COMIRNATY booster dose administered at least 6 months after completion of the primary series for use in individuals 16 years of age and older?
Please vote Yes or No.
Somehow the difference between 16 and 18 years old is a really big deal to these people. As he notes, there were 4 "No" votes on the original vaccine over this, people who were willing to stop the vaccine over this question.
The justification of this is that 'there were no 16-17 year olds in the testing group' as if 18 were a magical number that made everyone below that threshold a different physical magisterium rather than us having a social convention about being 18.
Here's an interesting bullet point from the introductory remarks.
Everybody thinks spacing the doses out further than the initial 3-4 weeks would have resulted in better immunity, but at the cost of slowing down vaccinations. So we chose faster vaccination in the face of a pandemic, but might want to reconsider that in the future.
I'm sure we'll get to that 'reconsider in the future' real soon now.
And also this:
We know a boost will work; the question is whether that’s the best thing to do versus, say, vaccinating everybody else.
So, since that is none of your damn business, we're done here, right?
Another “elephant in the room”, as Branswell put it, is the rare instances of myocarditis and pericarditis that sometimes happen in young men, and whether a 3rd dose will raise that frequency. Nobody knows, because the clinical trial here was too small to be powered to see such a rare event.
However, Israel has boosted 1.2 million people and seen exactly 1 case of this sort of heart inflammation. So that’s potentially a good omen if not exactly the RCT statistic we’d like to have in the best of all possible worlds. The acting chair of VRBPAC, Arnold Monto, cautioned that Israel is doing the oldest first, so their data under-represents males under 30 who are most at risk for myocarditis/pericarditis. So… the risk looks low, but really nobody knows.
That really, really, really gives us enough information, along with the 1% of the United States that has had a booster, by comparing it to the rate of such cases in a similar group from the first two shots, realizing that compared to Covid these risks were always absurdly small, and moving on with our lives.
I did love this:
Another slightly cute detail: Pfizer’s presentation ran long, and when they attempted to review the Israeli data that had already been discussed, the chair cut them off. I admit that as a former pharma scientist, it’s a gleeful fantasy of mine to be able to tell a senior VP of a pharma company to sit down and shut up. (Perhaps I am a bad person. But it’s hard to resist the cravings for a teensy slice of schadenfreude pie.)
So the conclusion was that they 'failed to resolve' the question of waning immunity, because it turns out that the FDA is smart enough to find the problems with the Israeli data.
But as I was worried about last week, they didn't consider at all the data that the rest of us are actually using as the basis of deciding whether or not there is waning immunity, which is the data coming in all around from everywhere else.
Thus, we have a situation in which the public health experts, when deciding precautions, act as if immunity is waning a lot. And when talking to the public they say immunity is waning a lot. Except when they're trying to tell someone to get vaccinated, in which case they mumble for a while. And of course, in that context, the answer of maybe it's waning and maybe it's not means it is waning, because you have to average out the possible worlds when deciding what to do, and guard against the 'risk' that waning is happening.
When you turn that around and consider a booster shot? Suddenly the 'risk' is that maybe immunity isn't waning. That would be terrible. There's a 'risk' that we might have given people life saving medicine when there weren't enough lives being saved, so we have to withhold the medicine until we're damn sure that isn't the case. Instead, people should be constantly stressed out, wear masks everywhere, socially distance and otherwise cripple their lives indefinitely, for the same reasons that weren't good enough evidence when it counted.
The concern with myocarditis/pericarditis really isn't any less stupid, and even if you decide it isn't stupid, it is confined to young males, so if we wanted to be stupid in a reasonable way we could let such people make a choice without taking it away from everyone else, or even approve for, say, men over 35 and women over 18, or whatever made everyone stop freaking out over nothing.
If you considered a pandemic that caused the symptoms and side effects of Covid-19 prevention we'd damn well have approved at least the third shot, and likely the fourth shot to be safe.
So we start with the first vote, which did not go well.
At 3:30pm, the vote on the question above came out negative: 3 Yes, 16 No, 0 Abstain. Interestingly, that’s 19 votes out of the 18 committee members! There was one accidental vote, apparently by a speaker; their choice was unclear, but it could not have changed the outcome. (This will be a subject of gossip in the months to come: who barged in and voted without the right?)
Now they’re discussing changing the question, to see if they can endorse boosters for some subgroups of people, if not the entire population. Remember my prediction above, that this would be the sensible outcome? Maybe, just maybe…
It wasn't unanimous, which is a good sign. That's still a lot of no votes, but I suspect they are weakly held. Last time, the move from 18 years old to 16 years old got 4 no votes. It stands to reason that at least 4 votes would probably flip here if we'd moved from 16 to 18. If we assume we had an accidental no vote (because probability and because the committee would likely notice the extra yes vote if it happened here) we go from 15-3 to 11-7, maybe better, so it would make sense to take a minute and check? And then check, say, Over 25? Or a split of men over 35 and women over 18, or something? Or ask people what they'd support?
What they did next instead was to check a very limited case, those over 65 or who are immunocompromised, or at high risk for exposures or comorbid conditions:
And yes, we've been through this before, and yes almost everyone has a plausible 'comorbid condition' or 'high exposure' if you think about it long enough, so one doesn't even have to lie. And yes, that would take care of the bulk of the real 'risk in the room' if everyone treated this as a personal puzzle to solve. Except for those who got Moderna or Johnson & Johnson as their first shot, of course, but screw them, at least for now. They seem to have 'not gotten a decision' which means they could get a decision later, at least.
There was no third vote. There was no attempt, once it was established that everyone supported some boosters, to find out how many boosters a majority did support, and go with that.
The President of the United States arranged for life saving medicine to be available to Americans who want it, and announced a program to get it to them. The FDA advisory committee agreed it was safe and effective life saving medicine (at minimum in everyone but young males) and decided that it would exclude those without an Officially Valid Excuse from getting access to that medicine indefinitely. They made it clear that part of this was resentment of the President arranging for life saving medicine without getting their approval first, part of this was their general principle of not preventing people from getting medicine being their least favorite thing in the world, and part of it was because in some hypothetical other world those vaccines had a fixed supply and now that fixed supply would go to the third world instead of sitting idle waiting for their approval, and if that turns out to be true I'm going to be glad I don't own a hat I'd then have to eat.
I'm going to quote The Grumpy Economist and Marginal Revolution in full here, who summarize the situation well. From MR:
My first reaction upon hearing that boosters were rejected was to ask the same thing: would these same “experts” say that, because the vaccines are still effective without boosters, vaccinated persons don’t need to wear masks and can resume normal life? Of course not. They use the criterion “prevents hospitalization” for evaluating boosters (2a) but switch back to “prevents infection” when the question is masks and other restrictions. What about those that are willing to accept the tiny risk of side effects to prevent infection so that they can get back to fully normal life? The Science (TM) tells us that one can’t transmit the virus if one is never infected to begin with.
Also, one of the No votes on boosters said that he feared approval would effectively turn boosters into a mandate and change the definition of fully vaccinated. So, it appears that the overzealousness to demand vaccine mandates has actually contributed to fewer people getting access to (booster) vaccines, thus paradoxically contributing to spread. A vivid illustration of the problem with, “That which is not mandatory should be prohibited.”
The biggest problem with public health professionals continues to be (1) elevation of their own normative value judgements — namely that NPIs are no big deal no matter how long they last — which have nothing to do with scientific expertise, (2) leading them to “shade” their interpretation of data to promote their preferred behavioral outcome rather than answering positive (non-normative) questions with positive scientific statements, (3) thus undermining the credibility of public health institutions (FDA, CDC) and leading to things like vaccine hesitancy.
And from Grumpy Economist:
What happened to the idea that the FDA's job is to proclaim only whether a vaccine is safe and effective? Then if you want to take it, that's up to you? (And we could argue about even that, i.e. whether "safe" is enough, whether FDA should have authority to make something unproven illegal, etc.)
I want a booster. Pfizer wants to sell me a booster. The data say it's safe and effective. Way more effective than masks. Period.
They hypocrisy on masks vs. boosters is amazing.
Indeed. Mandatory masks, banned boosters. There is a war.
Then the FDA decided to string us all along for five days, giving hope that perhaps they were going to disregard the recommendations, because what else would be taking so long?
Something was causing an unusual delay, which was getting so bad that the CDC was about to have to potentially postpone their meeting until the FDA makes up its mind. The suspense was killing us.
Then, last night, the FDA went with the recommendations. You'll need to find an Official Excuse to get your booster shot, or convince someone to give you one without one.

It's up to you if you want a booster. If you do want one, whether or not you are officially supposed to be on the list, go get one.
In seven days, it will be six months since my second shot, and I will get my third.
The CDC Tries To Respond
For the CDC meeting I'm going with a Twitter thread from Helen Branswell, who I've found to be a reliable source. Lots of interesting stuff.
The CDC has to decide what to recommend in light of the FDA's decision, so they scheduled a meeting for yesterday and today, and, as noted above, whoops.
Some good news made more explicit, which fits my priors:


Mixing and matching vaccines continues to be obviously a good idea, and the regulatory bodies are going to keep not allowing it due to 'lack of data' despite no theory of why there would be a problem, and the companies involved will continue not to study it because it's not worth it to them to do that. Which in practice means that even for those who would otherwise qualify, we're going to continue banning even second shots for those who got J&J for at least a while longer, and third shots for Moderna, although in practice this is something people can work around.
The trick is, there's data about a lot of things, but if you slice what counts as relevant data finely enough, you can claim there's no data whenever you'd prefer that there was no data. You want to worry about 16-17 year olds? Say that 18 year olds provide no data. If you wanted to, you could then say that people were the wrong gender, or the wrong race, or the wrong health status, or the wrong lifestyle, and keep doing that until your sample was small enough that there was 'no data.' Or you could realize that all data is data, and do something reasonable, but reasonable is not the watchword here.
Meanwhile, there's a non-zero chance that we'll get the even-more-perverse response that, well, it's not like this is urgent or anything, let's wait until all three booster shots are ready before we allow anyone to get one.

Given what we know, it's sufficiently clear that longer dose intervals are vastly better. The original intervals were chosen to get the studies done faster and get shots into arms faster, and were guesses. In the UK it is a scandal that the officials aren't 'doing enough' to inform people to avoid the horrible mistake of not spacing out their doses longer, and there's widespread speculation that the differences are big enough to explain differences between countries. So how's it going on that?
This graphic seems right and pretty great, a lot of people remain confused about this:

I always find it interesting when I disagree with my source's interpretation of the information they're sharing, such as this slide:

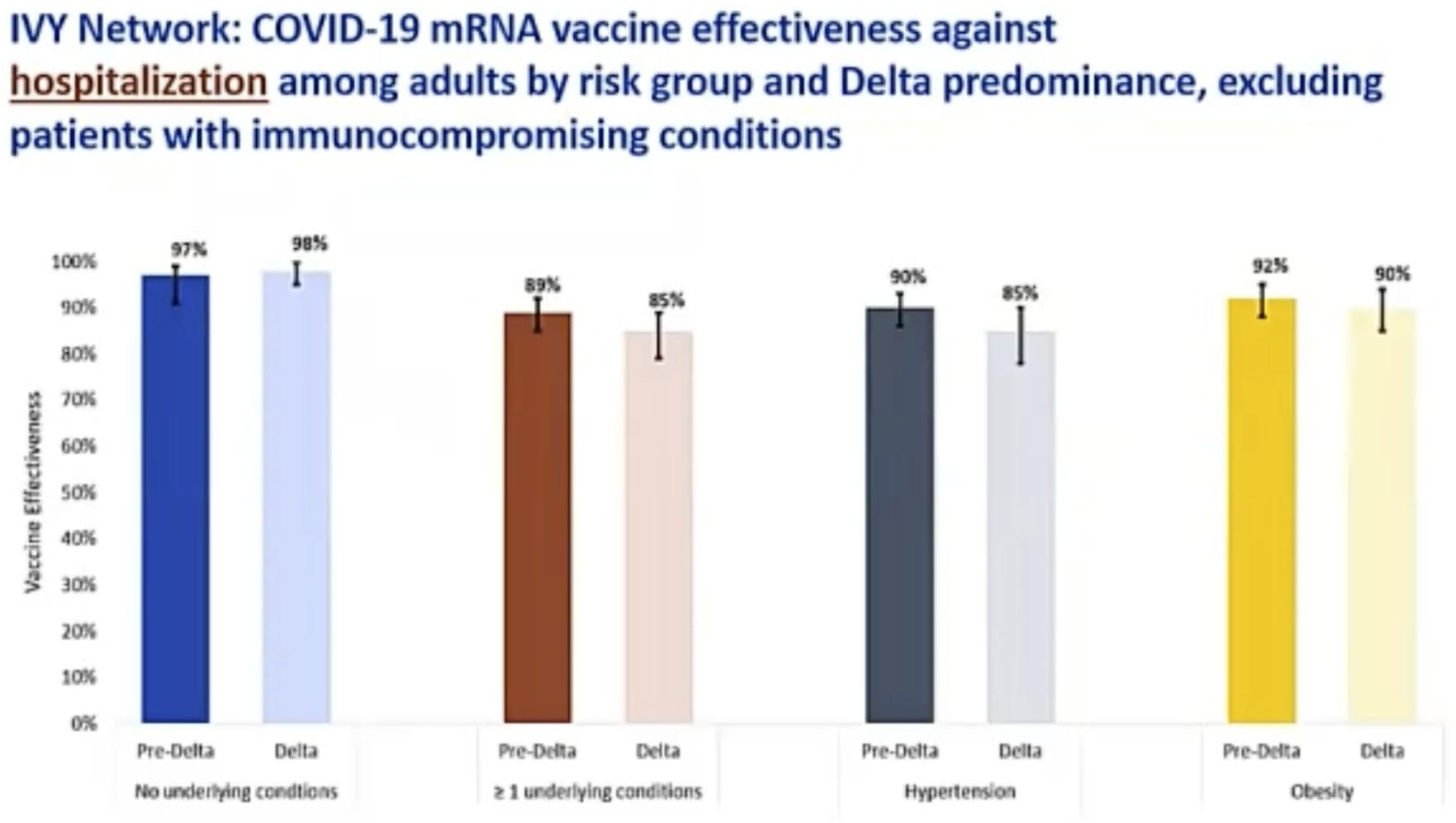
The effectiveness is still very good, but to me the difference between 90% (or 85%!) and 98% is a really big deal. That's a factor of five or more, on top of already being higher risk to begin with. In practical terms I do see this as 'a lot lower.'
The other thing this slide is doing is claiming that there's no substantial reduction in vaccine efficiency against hospitalization under Delta.
Given they have this slide, I'd be skeptical we're going to get a good ruling:
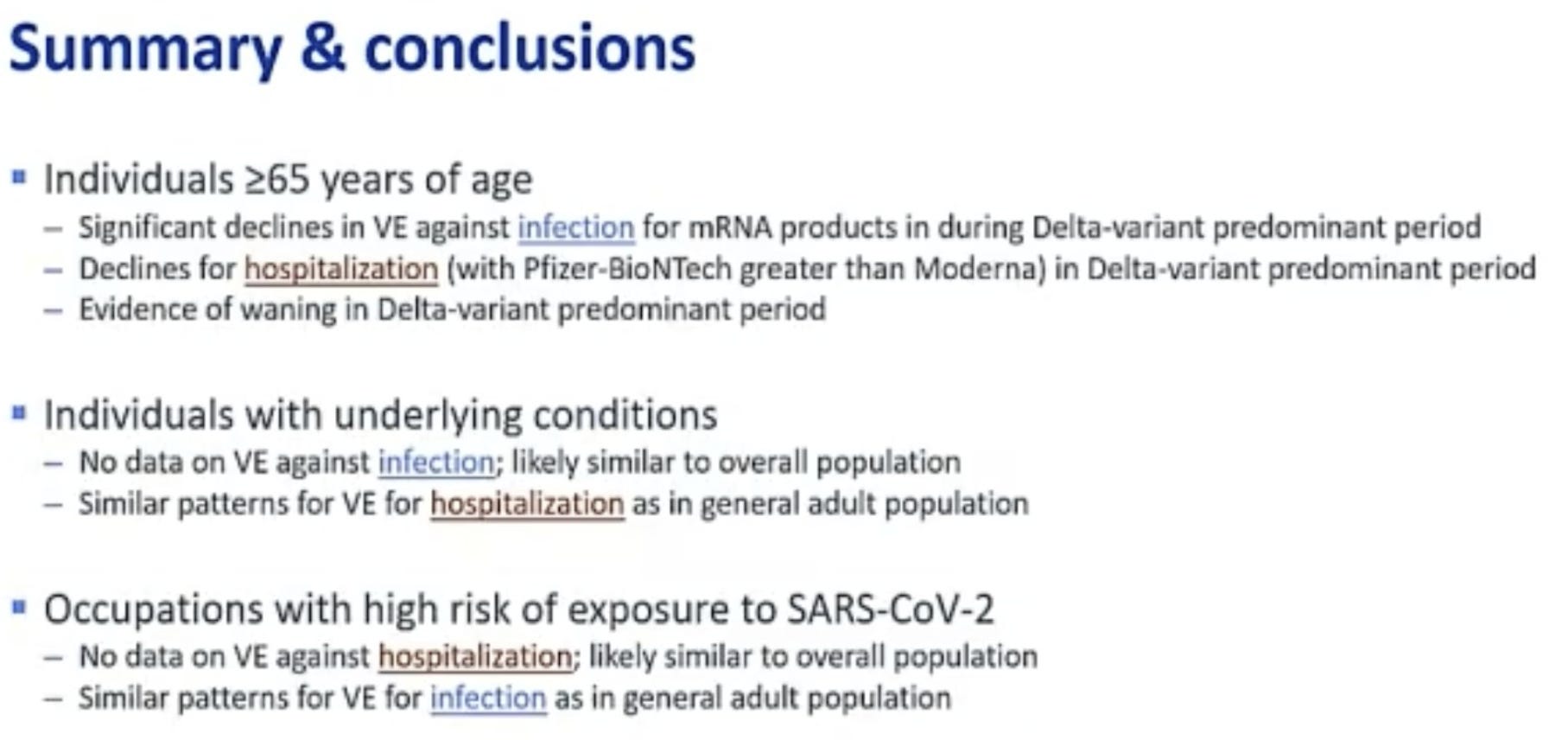
If they're grouping people like this, it shows how they're thinking. People are living their lives with one set of concerns. NPIs are being considered and mandated at great stress and expense with another related but different set of concerns. Then the booster is being considered with a much narrower set of concerns that treats the previous concerns, and the actions taken in response to them, as illegitimate things to worry about, and places the burden of proof entirely on those claiming there's an issue, despite the same people treating the issues as huge in other contexts, once again.
Yes, we don't have data on one specific super rare and not important side effect, so it's possible that the third dose will suddenly do ten times as much of that as the second one, in the sense that a lot of things are possible and many things do come to pass, but if the other side effects are at slightly lower rates I can't think of any reason to think it's plausible. Would happily accept wagers on that (unless someone has actual data).
We somehow need to keep saying this over and over, but a reminder:




Vaccine Mandates
At least one of the FDA "no" votes on boosters justified their decision by saying that approving the booster would amount to a de facto mandate, because once it was no longer forbidden it would of course be compulsory. They did have a point, and it was driven home rather quickly when the next day Pfizer announced that they'd proven their vaccine safe and effective in 5-11 year olds, because partisans have a principle that no time should ever be wasted in such situations:
This seems to be the consensus, that the moment the vaccine is permitted in children it should also be compulsory. No middle ground, no period of 'we think this is a good idea but it's up to you.' Zero to sixty in 3.5, hand over the keys, shut up and let us drive.
Of course, it's not your fault that the other half of the calculation is doing dumb things, like imposing mandates in minute one or withholding the shot that's a ticket to a normal life without all the extra daily trauma for months on end for no good reason. If anything, you'll need to move even more in the other direction, since things have already gone too far. So, whoops, and the cycle continues.
There is a war. You may not be the baddies, but let's say you're probably not the purely goodies either.
NPIs Including Mask and Testing Mandates
You know that whole thing about six feet apart? Well...

“The initial recommendation that the CDC brought to the White House … was 10 feet. A political appointee in the White House said we can’t recommend 10 feet. Nobody can measure 10 feet. It’s inoperable. Society will shut down. So the compromise was around six feet,” Gottlieb said.
So he's wrong, we do know where it comes from, it's an arbitrary number picked in the hopes people would listen to it. Which is reasonable in context, but important to know.
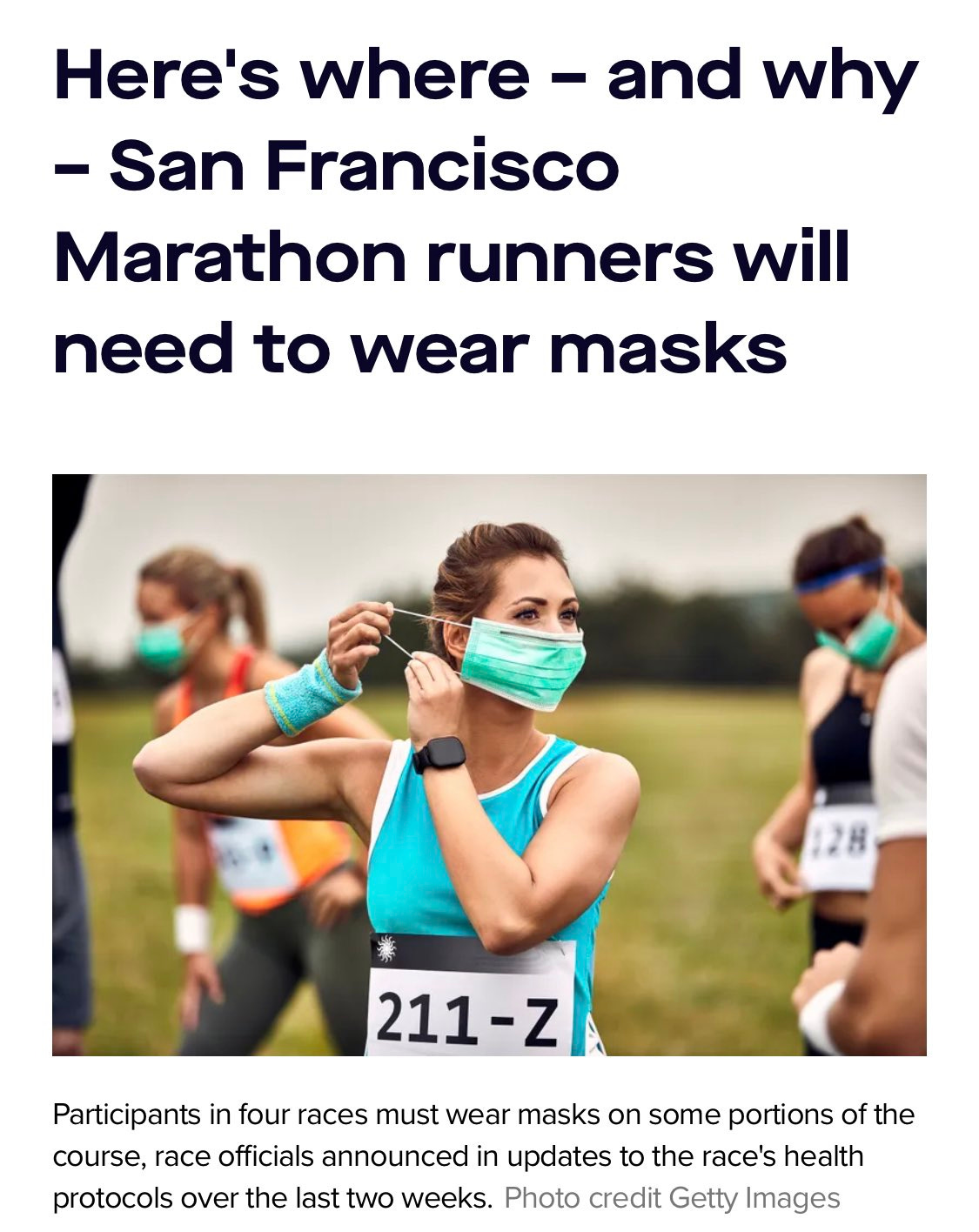
What else is there to say at this point? Here's what things are like in San Francisco.
Unless you are, you know, the mayor.
Link is a six minute interview with her, with gems like this.

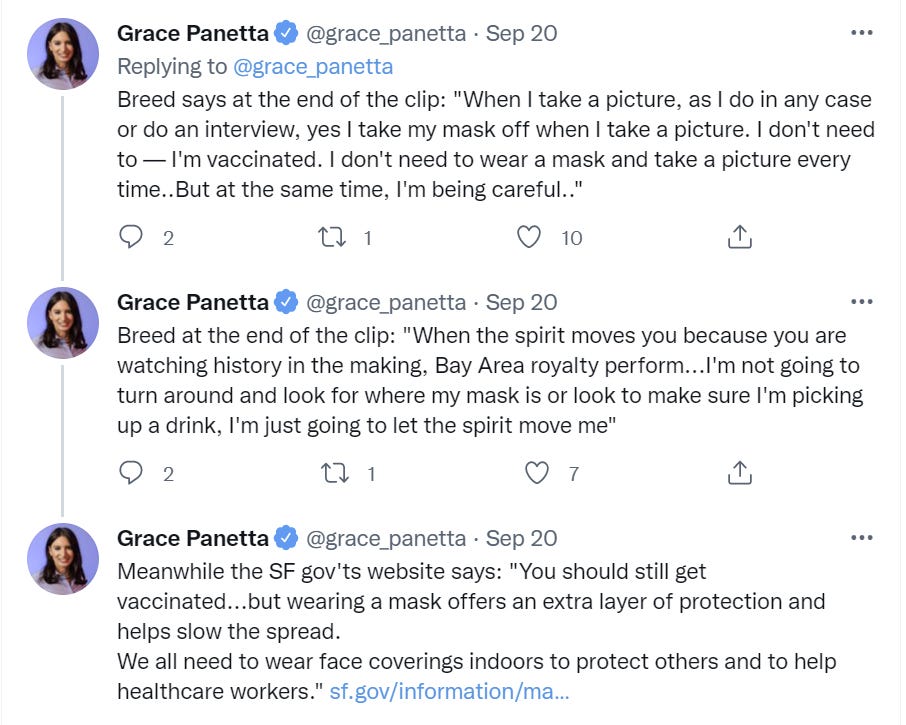
Oh, so it's fine, then. I agree, actually, there are more important things in life, but then why the hell is there a mask mandate?
Is it because you are famous and powerful, and therefore your experiences are better and you have power and thus the rules shouldn't apply to you?
I do thank her for explicitly endorsing this argument. History in the making.
The alternative explanation is that the rules were never intended to be obeyed, and there was always the expectation that no one follows rules so rules are fake. So she's not a hypocrite, you see, because she thinks the rules are fake for everyone which makes it okay? Kelsey sums up one issue with that.


The mask is off in more ways than one. Let's respond accordingly.
In Los Angeles, by contrast, they justified their full red carpet by pointing to alternative procedures to keep things safe, and I'm going to disagree with my source and say that this all looks reasonable to me.

Meanwhile, in Texas: A business owner expelled some customers for wearing masks. I am willing to bite this bullet. The people in question are being dumbasses and assholes, and the solution to 'I'm tired of the government bossing us around' is not to start bossing other people around for the hell of it, but hey. Their call. You can set whatever dress code you want, and customers are free to go elsewhere.
Think of the Children
There was an article in the New York Times about how schools and children are causing the Covid-19 surge and are at terrible risk. I won't link to it, but this appears to be what it claimed, and how that checks out. First, a completely unsubstantiated assumption about schools, because it fits the scare tactics desired:

So here's the thing, in addition to the whole kids-don't-get-severe-Covid thing. Covid is seasonal.
So when do schools reopen? The beginning of September? Here's Covid cases, nationwide, last year by week in that period:
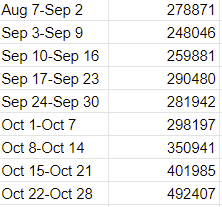
Sure looks to me like it was something that happened in October. What about this year? We peaked the week of September 1?
If your hypothesis is schools are causing Covid-19 to surge, it should strike you as rather odd that Covid-19 cases peaked right before school starts two years in a row, despite schools causing increased testing.
This is one of many data points that suggest that if anything schools prevent transmission, from a thread addressing various issues here:

I've seen lots and lots of claims that various peaks and valleys corresponded to when schools opened or closed and blamed the schools. I'm actually asking here, does anyone care to explain why the obvious test goes the other way?
Anyway, there was something else more concrete.
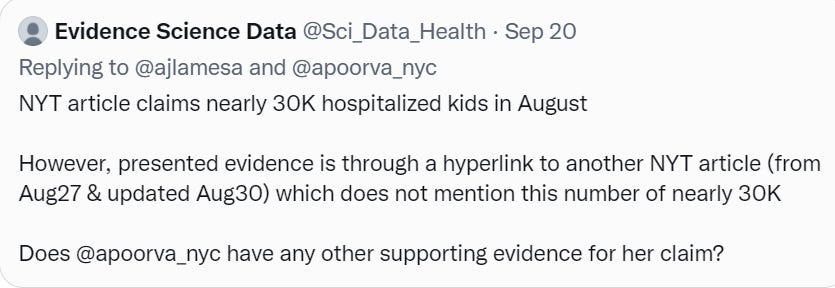
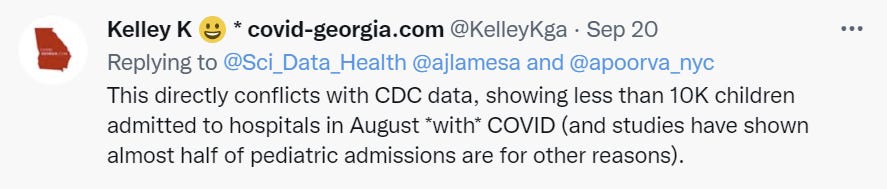
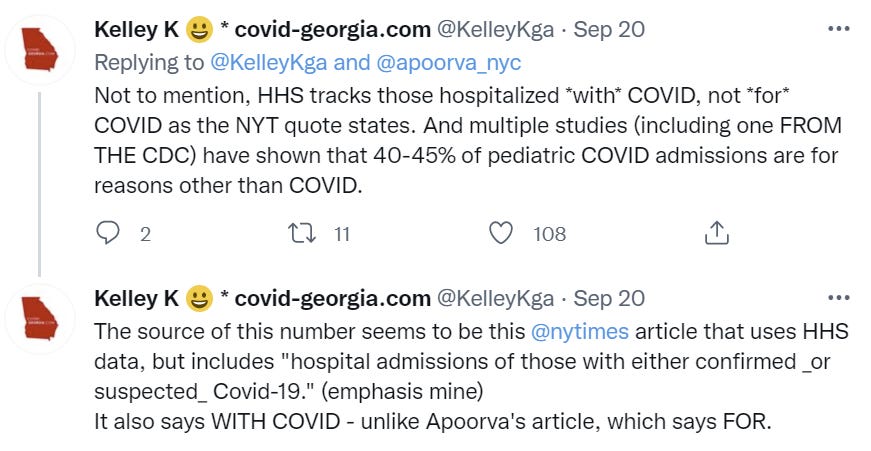
So it seems that the number got inflated by an order of magnitude or so (at least a factor of about six), via taking the number of kids hospitalized 'with either confirmed Covid-19 or suspected Covid-19' and taking that as the number of kids hospitalized 'FOR Covid-19.' No matter what some people might think, an extra zero matters.
Also the article claims that kids are more likely to spread Covid than the elderly, and generally as likely to spread it as adults, with sources that should not have survived scrutiny. I flat out disbelieve any such claims, they don't make any sense.
I don't know if they eventually printed a correction somewhere. Which is the point.
Lest you think this is everyone picking on an unimportant article, a link to it was where I first learned that Pfizer had found their vaccine to be safe and effective in 5-11 year-olds, before I saw any of these issues brought up. Whoops.


This is the future (some people) want. A mask, being forced onto the face of a crying two-year old, forever (1 minute video). Yes, you can say there are 'better ways' to do this, but this is frequently what actually happens, until their spirits die enough to yield.
When they grow up, if they're lucky, they get to go to Stanford.

It's not a few isolated places. Colleges are going completely crazy with their restrictions. Maybe we can hope that this will sufficiently ruin college that people stop going. Yet I fear that this is what the students actually want, that they have gone mad with various forms of righteousness and the love of telling others what to think and do, and this is merely the latest symptom of that.
Meanwhile, one of the children in my son's preschool has already tested positive for Covid-19. Luckily, preschool is mostly a myth that does not actually exist and he was going to not have class on Tuesday or Wednesday anyway, so it only cost one day of school. As an illustration of what I think of the testing regime in place, I did make some attempt to get him an at-home rapid Covid test when I found out he had actually gone to school with another positive child, cause the cost seemed so low, but when both Duane Reed and CVS said they and everyone else were sold out due to all the demand for weekly tests, I shrugged and went home rather than considering devoting actual effort to the task.
This seems to be a general problem, for example:

The Chris Rock Probably Cannot Smell What Anyone Is Cooking, Because He Has Covid-19

I wish him well, one of the funniest people in the world, taking time out while he's sick to help others. There's a twist, here's the friendly version of the problem.


Chris Rock got J&J. For some reason, a lot of people did not think 'I did X and then Y happened to me, Y is bad so do X' was a particularly compelling argument, whether or not they support doing X. Those who already opposed X saw it as a Catch-22 absurdist theater, and quite reasonably asked what wouldn't be used as a reason to get the vaccine?
This calls for theory of mind. Depending on your priors and what you already know, this could be evidence vaccination is a good idea, or it could be evidence against that, because it's providing several distinct potential updates.
We learned two things. First, Chris Rock got Covid-19. Second, based on his experiences, he is reporting that you do not want this.
Chris likely had one of two updates in mind.
Frequency and tangibility of Covid-19. If a celebrity you know gets it, perhaps it will feel more real. If there's more Covid-19, the benefits of vaccination go up.
Severity and experience of Covid-19, that having Covid-19 sucks even if you don't die, so again the benefits of vaccination go up. You don't want this, so avoid it.
Those are real effects, both plausibly changing behavior and doing so for mostly good reasons. The issue is that there are several other potential updates.
3. Effectiveness of vaccination. Chris Rock still got Covid-19 anyway, and it still sucked, so what's the point?
4. Effectiveness of J&J in particular. One shot of J&J is less effective, so make sure you get a second shot of some kind.
5. Arrogance of elites and non-relevance and non-trustworthiness of their arguments. Chris Rock was vaccinated, got Covid and then used that as evidence for vaccination, while failing to mention he'd been vaccinated. And That's Terrible.
Which of these dominate, and thus which direction you update, and whether Chris's statement was a good idea, thus varies from person to person, based on what they know and believe already.
In particular, this relates to Agnus Callard's concept of the verdict. To reach a verdict on a question is to consider the matter decided and hold your belief strongly, ignoring future potential evidence to the contrary unless it is sufficiently and unexpectedly strong. In the pure Bayesian sense this should either be a continuous effect (you update but your prior was extreme so it doesn't much matter) or not an effect at all, but in practice humans need to think like this often because we don't have enough compute not to.
The pro-vaccine camp has reached the verdict that vaccines work, because there's overwhelming evidence that they work, but also because there's a social consensus that there's overwhelming evidence that they work. It's unthinkable that they might not. Thus, when they see a statement like Chris's many won't even notice that it's a bit of evidence against vaccine effectiveness, at least for J&J, because who cares? Verdict is in.
Whereas if the verdict isn't in, and you have real doubts, that becomes quite salient. Similar things go on here for the other variables that one might change in response to this information.
In Other News
Kelsey Piper speaks truth about the whole Ivermectin debacle, although none of it should come as news.
An Atlantic article claims that an increasing percentage of those hospitalized for Covid-19 have mild symptoms, rendering the hospitalization numbers misleading. From the beginning I've been skeptical of using hospitalization numbers as anything but a measure of the status of hospitals, exactly because the decisions made in hospitals aren't consistent over time and that makes it hard to interpret the numbers, although things like the second derivative can still be useful.
Looks like the data on PhDs not getting vaccinated wasn't real. If I'd been making substantial updates off this data, I'd question much harder the procedure that caused me not to catch this error. As it is, I still do think I should have been more suspicious than I was, and will update accordingly. It's tough to know when to spend time on such questions, as I don't have enough funding/time to dig deep into every data source.
A reminder that almost everyone, almost everywhere, whether they know or admit it or not, is usually either talking nonsense or talking price.

"There is nothing special about them compared to any other preventive measure," he said. "The great thing about the vaccine for COVID-19 is that it prevents the risk of serious illness. Fantastic. People get to make the choice about what they want to do with that information."
But he said vaccination is not the only path to good health.
"It’s been treated almost like a religion and that’s just senseless," Ladapo said. "We support measures to good health. That’s vaccination, losing weight, exercising more, eating more fruits and vegetables, everything."
I mean... yes? And lots of people are mandating a bunch of other preventative measures that are vastly less effective and more expensive and 'risky' than the booster shots.
And by the way, we're also not allowing most people to get those booster shots.
A very interesting thought, in a great thread discussing supply chain issues:

Slack can take many forms. Wasting a lot of food on a regular basis isn't great, but it ensures the slack remains in the system, since in a pinch we could respond to a shortage by wasting less. The principle can be extended.
Not Covid
Someone finally gets it, and proposes auctions replace the coin toss in cricket. What I'd most like to see is an auction for the football in overtime in the NFL. Where are you willing to start in order to get the ball?