Mandatory Post About Monkeypox

It’s 2022, so of course enough people are worried about an epidemic of Monkeypox that it feels like a necessary public service to do a post about Monkeypox. I didn’t get to it especially fast exactly because I am not all that concerned, but I’m not entirely not concerned, so here we are.
Sarah Constantin has a basic facts post. Basic facts if nothing has changed:
The smallpox vaccine is 85% effective at stopping spread, but it uses live virus and leaves a scar. It is not generally available but we have a strategic stockpile that is sufficient for the entire United States (like we should aim to do with all possible pandemic viruses, but congress is refusing).
There are claims of both a 2.1% and a 3.6% case fatality rate from this version of monkeypox. Most deaths are in immunocompromised individuals. Can also be dangerous for pregnant women or children.
Most cases historically come from animal-to-human transmission.
Person to person transmission comes from prolonged social contact, sexual contact, living with the infected, saunas or contact with infected clothing or bedding.
Most cases in the outbreak are men who have sex with men, but that’s not true of cases in Africa.
Historical R0 estimate of 1.0.
The WHO is treating this as a standard outbreak and following standard procedure. Link includes diagnostic criteria.
Except that it looks like it has changed 50 SNPs, so maybe things changed.
This is a link to a spreadsheet of cases.
This thread also has a version of basic facts. This thread also covers the facts. This thread is excellent and has a bunch of facts. I go over that one later.
This thread contains links to 10 scientific papers, none of which I have read. I haven’t reached the ‘read all the papers’ level of dive yet, which tells you I’m not that worried.
Here is an OurWorldInData monkeypox data explorer. As of writing this cases are continuing to climb.
I have more hope that the WHO will respond reasonably to something like this, that has been around for a while, as opposed to Covid-19 which was novel. That doesn’t mean I’m counting on it.
I am not overly concerned, but I would describe the current situation as ‘concerning’ and would be much more concerned if no precautions were being taken or if people were generally acting as unconcerned as health officials are urging us to be.
The situation does not seem all that analogous to the situation with Covid. This is not a new virus. It is a virus that has been around for a long time. There is the concern that as our vaccination campaigns against smallpox fade into the past the population gets incrementally more vulnerable in a way that might require countermeasures, but it seems highly unlikely those countermeasures would need to be onerous or even include vaccination. The pattern of spread only makes sense if this is not that easy a virus to catch.
One thing that does make me worry is that the worst-case scenario, if things do get bad, is not that everyone gets vaccinated. That would be the worst-case scenario for a saner civilization. In ours, there is every reason to expect widespread resistance to such a campaign were it to prove necessary, and for this and other reasons a widespread reluctance to pull the trigger on the campaign. And of course, because of the insanity of our healthcare system, unless and until we’re ready for a major vaccination push it is unlikely that the shot will be generally available at all. So the more realistic worst-case scenarios are either that we end up having an epidemic without the vaccine because of these factors, or we have the vaccine but few people choose to take it.
The good news is I do not expect things to come to that unless the genetic changes are a big deal.
The bad news is there is some chance the changes are a big deal.
Don’t Panic
The public health authorities are saying ‘Don’t Panic’ in large friendly letters. As readers of the guide know this is good advice, but not if it crosses over into not reacting to potential problems. Even if everything is probably going to be fine, the expected value of the problem could still be in ‘buy very out of the money puts’ territory.
And when experts say monkeypox does not pose a serious risk to the public, and ‘caution against comparing it to Covid-19,’ how do you instinctively react to that? How do you update? After all that we have seen these past few years, those are not reassuring words.
Nor are these:
At least 17 infections of the rare disease have been confirmed in non-endemic areas such as the United States, United Kingdom, Portugal, Sweden and Italy, and dozens of possible cases are under investigation in those nations as well as in Canada and Spain.
If we don’t have a problem, why are cases showing up in this many different countries at once?
Once again, as with Covid-19, we have few cases so far but we also have confirmation of community transmission. And you know what really doesn’t make me feel better?
Health experts stress the risk to the public remains low and most people don't need to be immediately fearful of contracting the illness.
What are the words ‘most’ and ‘immediately’ doing in that sentence? If they’re needed in that sentence, then it does seem like some amount of slight panicking might be in order. When something is on an exponential growth curve and you are told it isn’t an immediate problem that is not reassuring.
Also, where have we heard this before?
The disease can also spread from person-to-person via large respiratory droplets in the air, but they cannot travel more than a few feet so two people would need to have prolonged close contact.
We even got a mistaken (or at least totally premature and completely irresponsible) claim that monkeypox is likely to be airborne, from a known unreliable source.


There are two things to say about this, other than the reminder not to listen to Eric Feigl-Ding.
One is that underneath it all he’s actually right about the precautionary principle here. This might be airborne (newly or otherwise) and it is damn well worth checking to be sure and until then not assuming that it isn’t.
The other is that there’s another easy-to-jump-to conclusion here, based on the fact that wait, we at least kind of did WHAT?
Gain of function research continues. Even assuming nothing has gone seriously wrong yet, it’s only a matter of time.
On the core question of whether monkeypox is safely not airborne, I’d say I do not actively disbelieve it, but it rhymes somewhat too much in too many ways to believe and not verify even if nothing has changed. If I had to guess how likely it is to be airborne I’d have to say at least ~5% in my current epistemic state. Which is kind of a lot.
She added this transmission route is different from that of COVID-19, which is spread through small aerosols that can hang in the air for several minutes.
"Aerosols are not subject to gravity but large droplets, they get pulled to the ground," Doron said. "Also, monkeypox isn't an illness that is transmitted during the asymptomatic phase, which is what made COVID such a formidable foe."
Early in Covid-19 we were told no asymptomatic transmission. We were told it wasn’t an aerosol. So, again, at best, need to verify - ‘expert’ claims don’t cut it anymore in 2022. I share most, but not all (I’m definitely not at ‘pretty sure’), of Divia’s skepticism here.

I applaud Nature for the careful wording here, emphasis mine. Post is a good overview.
Unlike SARS-CoV-2, which spreads through tiny air-borne droplets called aerosols, monkeypox is thought to spread from close contact with bodily fluids, such as saliva from coughing.
I also do put substantial weight on the ‘this doesn’t rhyme as much as you think it does’ arguments.

Also Nature brings up the possibility something changed beyond fading inoculations.
Answers to those questions could help researchers to determine whether the sudden uptick in cases stems from a mutation that allows monkeypox to transmit more readily than it did in the past, and whether each of the outbreaks traces back to a single origin, says Raina MacIntyre, an infectious-diseases epidemiologist at the University of New South Wales in Sydney, Australia.
Although I did chuckle a bit at this attempt to pretend obvious things aren’t obvious.
Another puzzle is why almost all of the case clusters include men aged 20–50, many of whom are men who have sex with men (MSM).
What is reassuring is monkeypox has been in a form that looks like this for a long time.
"It's important to note this is not a new virus," said Dr. John Brownstein, an epidemiologist at Boston Children's Hospital and an ABC News contributor. "This has been around for a long while. It's mostly endemic in parts of western Africa but you will occasionally see it in other parts of the world."
People are typically infected by animals through a bite or a scratch or through preparation and consumption of contaminated bush meat.
The first case was observed in 1970 and in Africa it is considered endemic. If something can be long term endemic in a large region and neither get completely out of control there nor spread to other regions, then for it to suddenly break through quickly either it is a short term blip based that will fizzle out or something must have changed.
Also somewhat reassuring is this description which I trust a lot more than the claims on transmission.
Monkeypox generally is a mild illness with the most common symptoms being fever, headache, fatigue and muscle aches.
Patients can develop a rash and lesions that often begin on the face before spreading to the rest of the body.
"It starts out as spots, then small blisters like you'll see with chickenpox, then pus-filled blisters and then they scab over," Doron explained. "It's a long illness. It lasts a few weeks, but you can be contagious for several weeks and contagious until the blisters scab over."
A few weeks of this state, while being infectious, is definitely no fun and would suck quite a lot, but there are worse things. The death rate from the last recorded outbreak was 2.1%, which also sucks a lot, but four of the six deaths were in immunocompromised people with AIDS. And again there are worse things.
Also it’s possible we are dealing with a worse thing. And even within the cluster there have been some changes?


More variation than we should randomly expect in a given time is, in some sense, to be expected, but it is at least weak evidence that something substantial may have changed. Here is Scott Gottlieb speculating that it could be (slightly) more contagious.
Here is a link to actual sequencing from Portugal for those looking to deep dive. These guys are also helping with tracking sequencing.
Despite those changes, the protein coding sequence appears identical, which indeed argues against evolutionary adaptation, but isn’t definitive on its own.

This next part confused me - 9% seems like a pretty low attack rate?
The other evidence also suggests things have not substantially changed, since it is all consistent with what we knew before, but this is far from definitive.
Another problem is identification. Since monkeypox is so rare outside of Africa, it makes sense that it’s not high on anyone’s differential diagnosis. This links to the contact tracing guide.

Cevik’s thread ends with links to additional resources, some of which I’ve incorporated into this post.
This thread claims they ‘ran a simulation’ recently of a monkeypox outbreak and got a ton of deaths, which is worth what you think it is (and several tweets have been deleted) except that this is certainly a possible outcome. Again, precautionary principle.
Should We Vaccinate Now?
Vaccination for Covid-19 will often knock you on your ass for a day or two, but otherwise it is an exceptionally easy sell. Vaccination for monkeypox is not so simple. One can say ‘vaccinated everyone now’ but the vaccine contains live virus and leaves a visible scar.
That’s different from saying we should produce and verify the vaccine now. That is a much better proposal, and we are indeed ramping up production at least somewhat. We should absolutely be getting our defenses ready. What stocks we have should be checked to confirm they’re still good and will work on what we are seeing in the wild. If we don’t have enough vaccine for everyone we might need to vaccinate worldwide, which we don’t (we used to at least have enough for all Americans but don’t now) we should get production started. I can’t imagine having that around is a bad idea in any case, especially given the Russia situation.
Sarah recommends the following package, which seems right:
Record suspected cases of monkeypox, test them with PCR and record their contacts.
Order enough smallpox/monkeypox vaccines for the whole population if necessary.
Order stockpiles of tecovirimat and brincidovofir, the only FDA and EMA approved antiviral drugs for monkeypox, cowpox, and smallpox.
Approve and purchase PCR tests for monkeypox. (Currently I don’t see any commercial manufacturers, but some research institutes like the Institute for Tropical Medicine in Antwerp conduct PCR testing.)
I would add to that we should verify that the vaccine still has its full effectiveness given the changes we have seen. I still expect it to fully work, but this is not the kind of thing we leave to chance.
We are not at the stage where challenge trials make sense here in terms of the virus, but we are absolutely at the ‘vaccinate some people and check their response, and their antibodies against the virus in the lab’ phase.
Well, actually, we are totally at a place where actual challenge trials make sense if one can do the math and live in a sane civilization. It only takes a tiny chance of a big problem to be worth endangering a few people to better understand what you’re up against, those few people can be well-compensated in money and also honor and status and would happily volunteer and so on, all the usual arguments. Worth noting.
Kai reports an official assessment of ‘moderate risk’ for men who have multiple male sexual partners, low for everyone else, and an expectation of more cases before it gets better. I agree that if things start out this way chances are you’re not at or too near the peak yet, especially given we only learned of the problem within a week and the incubation period is longer than that. However, to say ‘moderate risk’ right now seems kind of absurd when you think about it. We’re talking worldwide about less than a thousand cases. The risk literally right now is not yet moderate, no matter who you are. It’s traditional to scare such communities way out of proportion to the actual risks involved, and the tradition is being continued. That doesn’t mean the risk is zero, and the risk will rise - it might well be moderate soon enough. But that seems premature as I write this.
For everyone else, I’d expect it to remain low unless, again, things have changed more than we expect. And by low we mean essentially none.
Metaculus
Now that we’ve covered the information sources it’s time to look at the prediction markets.
Once again Metaculus is giving us a solid baseline so that we can begin our thinking. They have ten markets.
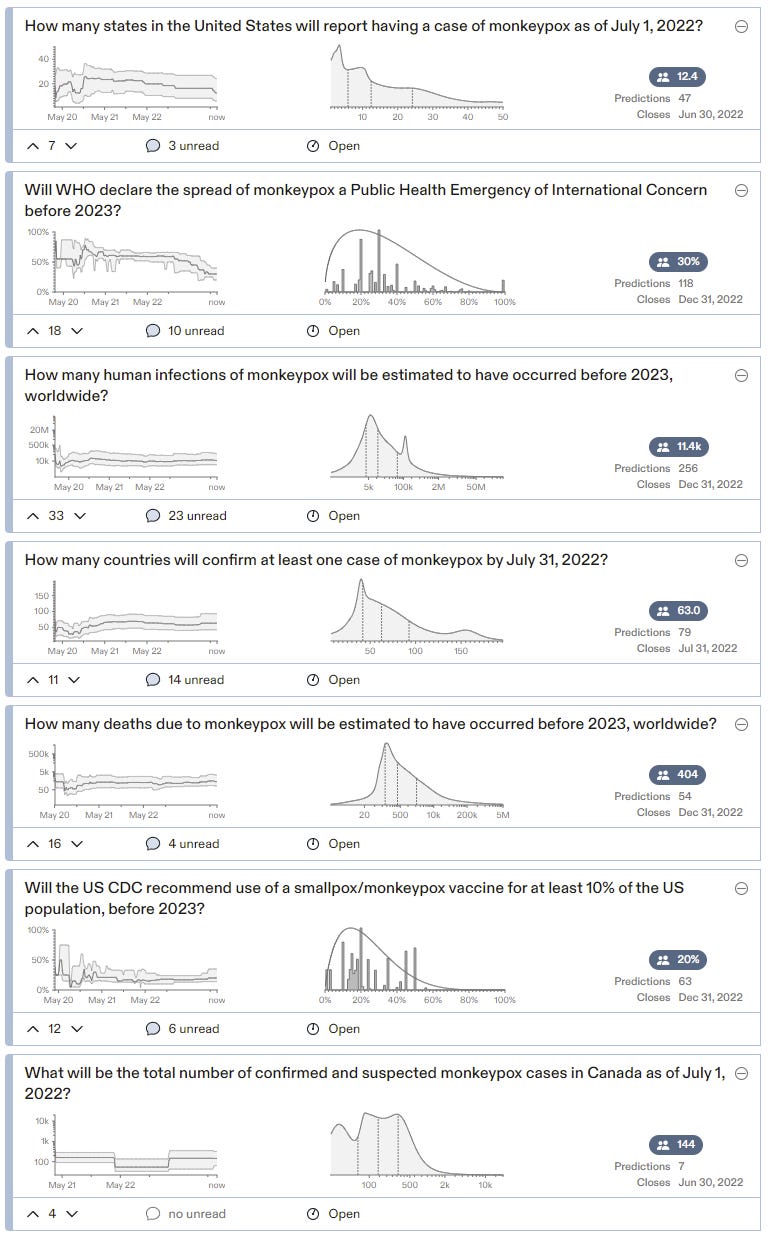
This is a mix of some tangible short-term questions and attempts to represent the most important questions.
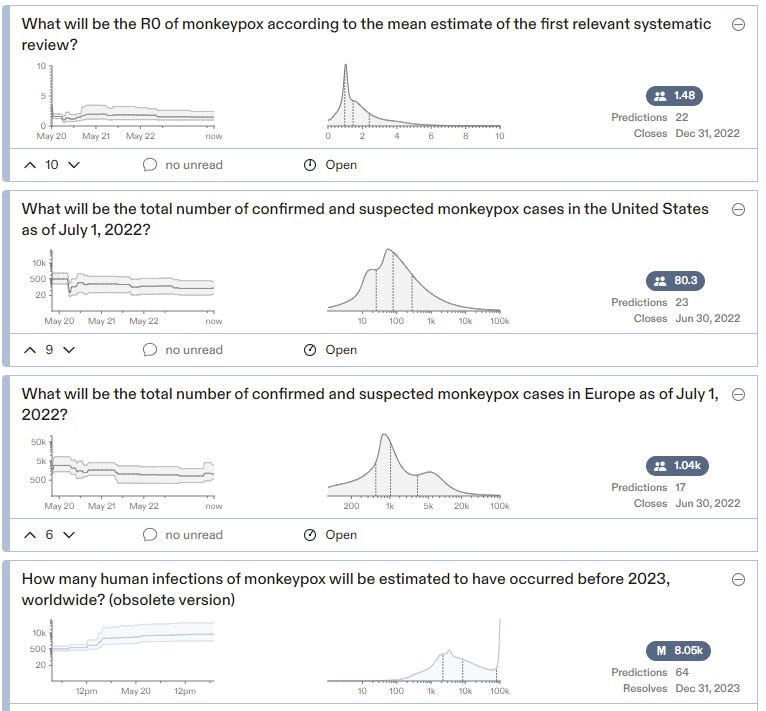
The estimate of R0 here is that it is likely to be well above 1. Yet predictions here do not anticipate either a mass vaccination campaign or a massive surge in cases.
That’s an odd combination.
If R0 is 1.48, given the current level of vaccination, something would have to prevent exponential growth. If it ends up being prior infections then these case expectations are way too low. If it ends up being vaccination, that’s predicted to only happen 20% of the time even for recommending it to 10% of the population. So this doesn’t seem like it’s telling a consistent story, unless the 1.48 refers to a specific narrow subpopulation, at which point it is plausible, and the subpopulation is small and could adjust its behavior, which would allow it all to make sense.
Something like that is my baseline scenario here. The vast majority of the time, almost all of us would have been better off if we had ignored the whole monkeypox thing entirely. But the only way for that to be true is to be in a world where a lot of people don’t ignore things in this reference class. So again, here we are.
My plan is totally not to worry about this again, and for this market to resolve to no.
"The smallpox vaccine is 85% effective at stopping spread, but it uses live virus and leaves a scar."
This description sounds serious, but my scar is barely noticeable, in the axilla region -- I (born 1970) went to look for it after I read this sentence, and I was like, "Oh, yeah! Look at that!"
I hate to be a debbie downer but can we just chill on giant sex conferences for a few months?