

Omicron Post #13: Outlook

Omicron is now the dominant strain, so much of what would otherwise have gone into this Omicron post ended up in the latest weekly post instead, and I’m considering the right way to merge the two streams together.
In addition to some amount of the usual business, the focus of this post will be an explicit attempt to look at what’s likely to happen from here, and give my baseline scenario.
I recently had reason to chart out what I expected that baseline scenario to be around the world, so it makes sense to share it here.
The world can be divided into five (highly unequally sized) parts, with increasing levels of uncertainty, some places are unclear on whether they’re in groups two, three or four:
South Africa and other already-peaked areas.
Uncontrolled spread: Europe, North America, India, Israel, Australia and Argentina.
Without an Omicron wave, or without good data: Third world, Russia.
Previous containment: South Korea, Japan, Taiwan and New Zealand.
Special case of previous containment: China.
South Africa and Other Already-Peaked Areas
This is the easy story to tell. Predictions about the past are often still hard, but they’re a lot easier.
A few African countries have already finished their Omicron waves, and got through mostly unscathed. Since they’re in the southern hemisphere, one can worry that there’s a wave coming in their winter a few months from now, but I would expect any such wave to be mild even if relatively little is done to prepare, given how things went this time, and that those infections are now baked in.
Uncontrolled spread: Europe, North America, India, Israel, Australia and Argentina.
This is where most of my readers live, and where I live, so it’s been my main focus. There is now a very clear baseline scenario.
Infection rates increase exponentially until they hit a peak. In major cities, this plateau will usually be quite high, with more than 1% of people infected each day, and likely 10%+ of the population testing positive at any given time. In rural areas, the plateau is likely going to be somewhat lower, but not dramatically lower.
Once you hit that peak, there will be a short period (a week or less probably in most cases) before the decline starts in earnest, then picks up speed. Once it’s gone down to something that will usually be between 25% and 50% of its maximum over the course of a few weeks, the decline starts to slow in percentage terms as behaviors adjust back somewhat. Then over time, there is a slow decline, which mostly continues until such time as other dynamics (like weather, or another variant) change the game once more, or you stabilize at low endemic levels.
There are substantial disruptions during the peak period, lasting roughly a month, but nothing as scary or severe as early 2020, and no breakdowns of civil order. Schools end up closed for a few weeks to a month in many places, others have to quickly close for a few days due to staffing issues, but some manage to stay open and it’s fine, they don’t meaningfully make anything worse.
As long as the hospitals manage to continue to provide care, there’s a ton of cases, but not that many deaths. The hospitals come under stress about six days after the relevant cases, through a mix of a lack of staffing and a flood of new patients. The question is what the true capacity is, and what happens when you exceed it, and what our ability is to do triage. Even when we ‘get through’ those weeks, life in the hospitals is still terrible during this period.
Once hospital admissions peak and start turning downward again, and it’s clear this isn’t simply hitting capacity limits and turning people away, we can know that we’re going to make it through in a given area.
We do know that London and New York in particular are almost certainly going to be fine, but other areas have lower capacity, sometimes much lower, and are ‘running behind’ in terms of how far along on this map they are, so they are not yet in the clear.
One can talk in terms of countries, but the situation is everywhere a local phenomenon.
Even within New York City, Manhattan has peaked, Brooklyn probably peaked a few days after that, but the rest of the city probably hasn’t peaked quite yet. I don’t know the details in London, but the situation is likely similar, with the center already declining, but other areas still going up along with the rest of the UK. The combining of local peaks into a region or nation gives a broader curve that looks less dramatic than the local graphs.
Who gets there when?
New York and London (or at least their central areas, and their aggregates) are the two places we can confirm have already hit peak. San Francisco has the hospital data that shows something similar, so it’s likely many major cities are also in this group.
Most other places are running somewhat behind that. The more rural you are, the slower things are to develop, and the decline will likely also be somewhat (although not as much) slower.
A lot of Europe and North America are on remarkably similar timelines. The United States, United Kingdom, France, Spain and Italy are all in this group.
I expect the peak for this group to be something like January 19. Exponential growth happens fast, so there’s less uncertainty in the timeline than there might appear to be, but being a week off in either direction would still be inside my 80% confidence interval. If the group hasn’t broadly peaked by month’s end, that would be very surprising.
Other places got started slower, but are still in the same boat. This is a combination of less international travel causing things to start slower, and slower spread once things get started. If there’s a place that has a lot of travel but hasn’t taken off yet, it’s probably developing slower, and its timeline will get further behind over time. Whereas places that have less travel are likely equally fast.
Here’s some of the key members of the group.
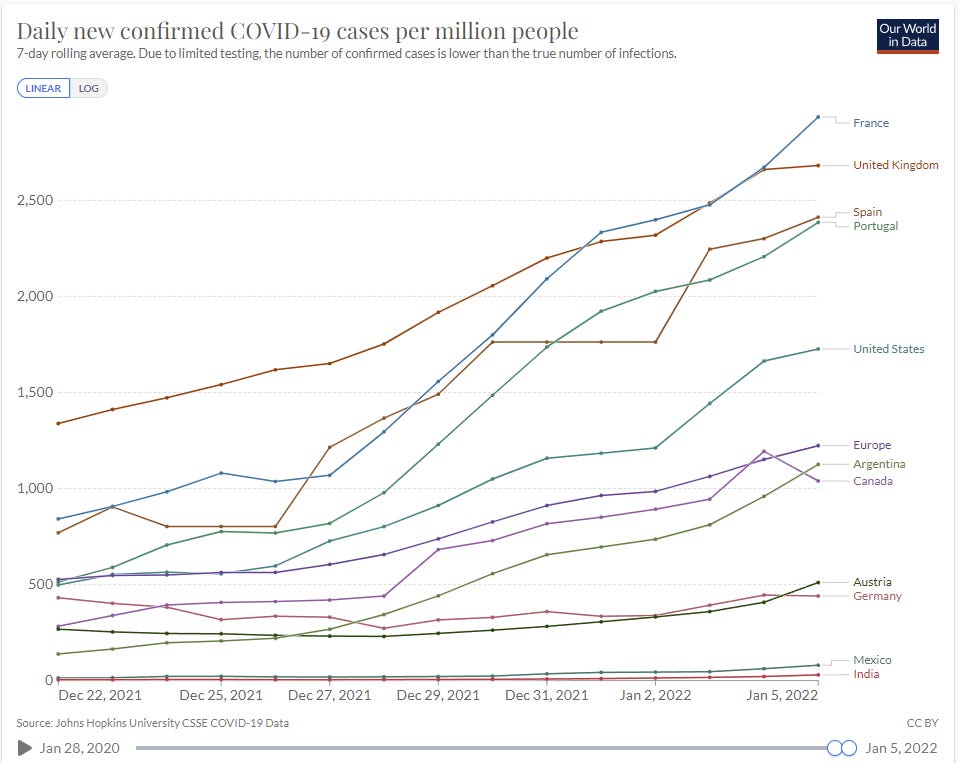
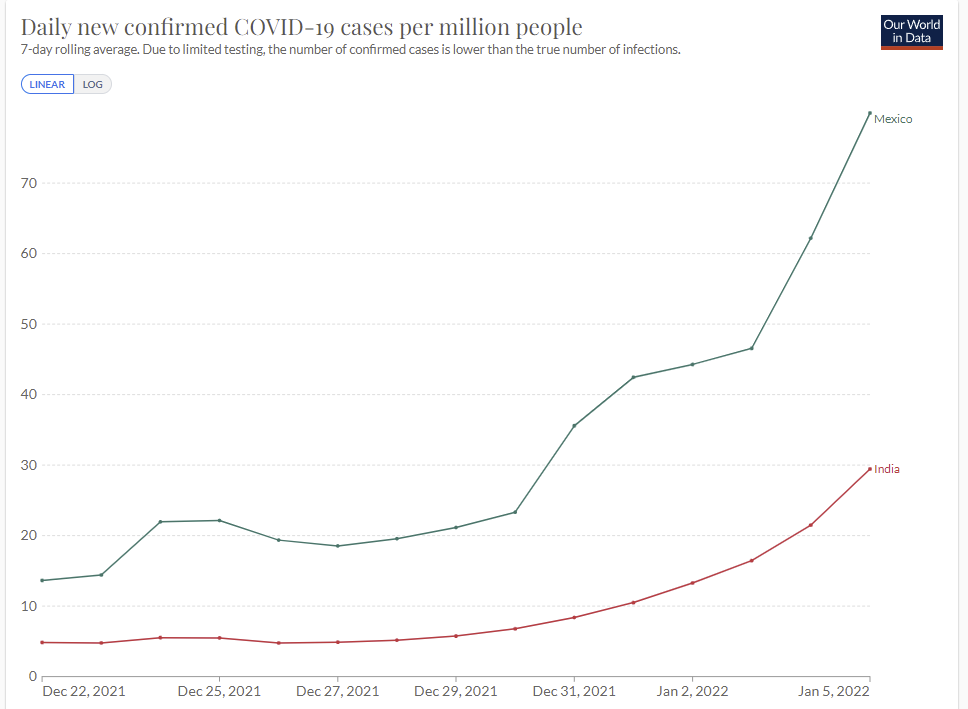
And here’s only the ones that have low case numbers.
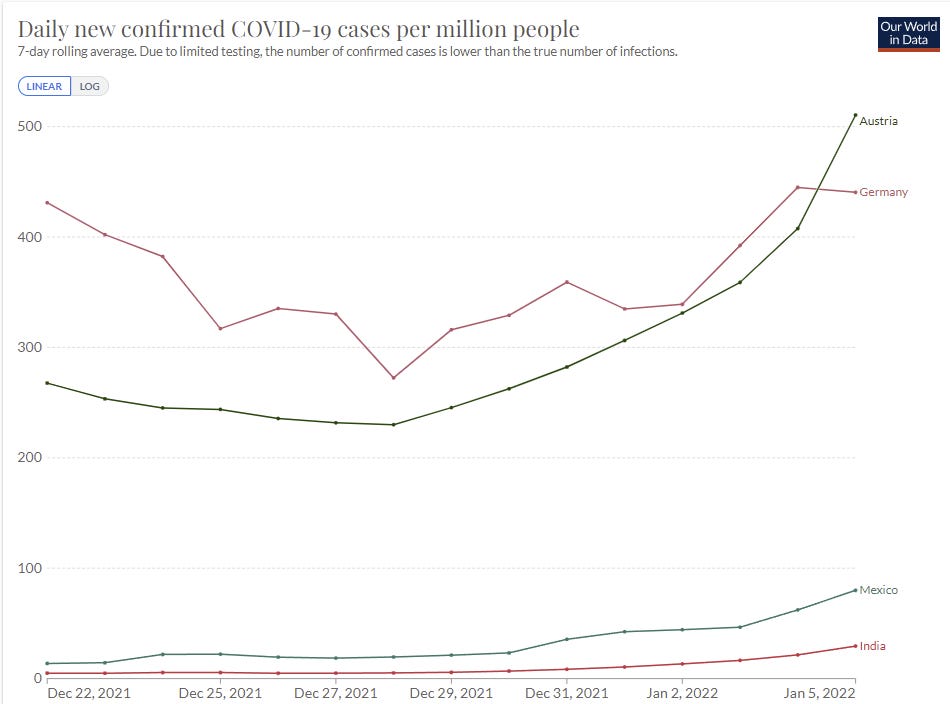
Austria, Mexico and India here all show accelerating growth as Omicron takes over from Delta. Germany is the weird one, where there’s been sufficient prevention to make it close, but looking at the Omicron-specific graphs makes it clear that the same thing is going to happen eventually, it’s simply going to happen slower, and that extra time seems unlikely to be put to good use. There won’t be that much of it. I’m still confident they belong in this category.
Canada is doing a more reasonable thing, and instituting prevention measures when they get in danger of exceeding their hospital capacity, to try and flatten the top of the curve. Flattening the curve on the way up doesn’t accomplish anything, you need to flatten the top. I don’t expect it to accomplish all that much or be worth the trouble, but at least it’s not automatically doomed. The last day of data is likely a reporting delay there.
Mexico and India are a few weeks behind the USA and Europe, but they’ll get there soon enough. Note that deaths in India have been severely undercounted. When things get bad in India, that is the place I am most worried will get quite bad, and we should be thinking now about how to use aid to get mitigation efforts in place.
The fundamental insight is, either you can contain this thing, or you can’t. For a while Mexico didn’t look like it had a problem, but there was no reason to think they could contain it, so all that did was delay things. India was the same, and now we are seeing the same rapid exponential growth there we saw elsewhere, and getting to 1000+ from 30 is not that many doublings. They’re only two or three weeks behind.
There are doubtless some places I’m missing here. For example, when I started writing up the model Peru wouldn’t have been included, but it probably goes here now, and Brazil could join soon as well.
Without an Omicron wave, or without good data: Third world, Russia.
Some such countries show some signs of a potential wave, but many flat out don’t, as you can see here.
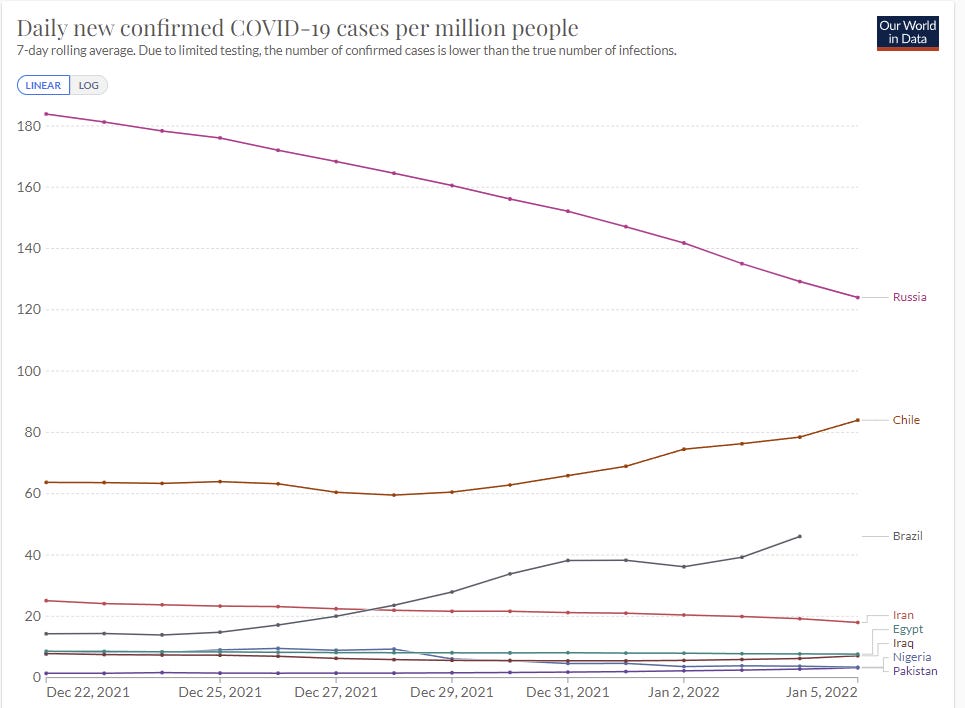
Many of these places have had much higher rates in the past, so it isn’t a pure testing issue for them. Some of these places are sufficiently unnatural places for Covid-19, at least at this time, that it’s possible waves will not arrive, or that once they get to moderate levels moderate behavioral adjustments will stabilize things at a level they can handle.
The key distinction between this and the next category is that these nations didn’t take extreme measures to get containment, which gives potential for more slack to solve the issue or contain the damage.
Previous containment: South Korea, Japan, Taiwan and New Zealand
If Australia was on the graph it would destroy the y-axis. That’s what happens when procedures that previously were sufficient become inadequate. Here South Korea is still doing a similar thing, levels are very different.
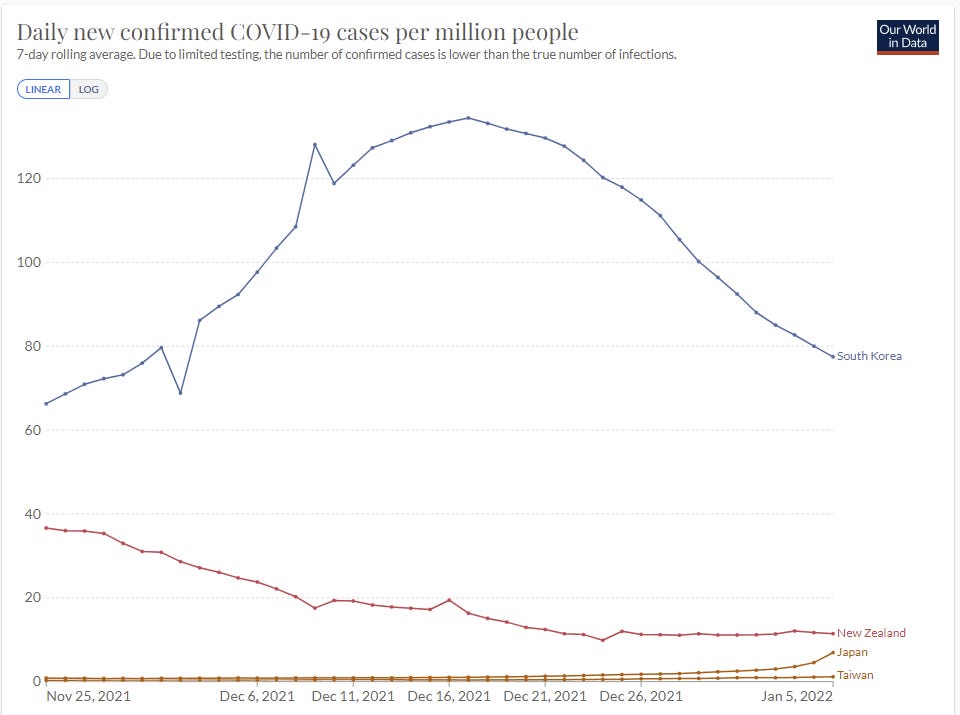
Word from New Zealand in the comments is that border controls are holding for now, but that this is widely expected to fail, and if Delta wasn’t fully wiped out then I agree with this assessment. It may be a bit, but they’re going to be in group one before their winter is out.
The last few days in Japan do not bode well, but it’s probably fine? They’ve gone from under 1.66 per million two weeks ago to 6.91. That’s one doubling per week. My guess is that Japan retains enough slack to continue to contain the situation. Taiwan also seems like it’s got a chance.
For now South Korea is still headed downwards, which indicates they’ve managed to keep Omicron out, but also they got high enough before that I am highly skeptical that they can contain this for that long. I expect them to end up in the first category.
That leaves the big one. China.
China
China is the big question. They managed to maintain a zero Covid policy so far, so almost none of them have immunity that way. The Chinese vaccine was always less effective, and offers minimal protection against infection by Omicron.
Thus, China is facing a much harder problem with Omicron than they faced in previous waves. Measures that previously would have been enough will no longer be enough.
Locking down Xi’an, with 1% of their population, has been frustratingly slow at containing the situation there. My presumption is that China can and if necessary would continue to do things on this level, but that doing that for 10% of the population for long periods is a very different proposition. There is only so much ammunition available.
Thing is, if China can’t get to and stay at actual zero Omicron, then they need a sustainable way to keep it from exploding, or they will lose and nothing they do will matter. Taking extreme measures on outbreaks requires that the rest of your strategy be close to enough on its own. Keeping things out via borders requires that you really mean it, or all you do is slow things down.
Meanwhile, they’re planning to host the Olympic Games, and, well, whoops?
I’ve underestimated China’s containment abilities throughout, and been repeatedly surprised. Once again, I’m skeptical they can pull this off, and once again it’s mostly a Boolean, either the strategy works or it doesn’t. But given their track record I can’t count them out of it, neither result would surprise me, nor could I find any prediction markets that speak directly to this. Where there is a will, there can sometimes be a way, and China has a will in a way that Western countries do not.
I’m going to tentatively put my probability that China keeps Omicron contained at 40%, but I don’t have great knowledge about many details that could update that, including the opinions of others who have thought about it. So I would update quickly, especially if someone offered to wager on either side.
Now a round up of the other Omicron News. Remember, a lot of this got moved to the weekly update.
Vaccine Effectiveness
Third dose holds up at 90% effectiveness against hospitalization for at least three months for the elderly. UK using this to decline to authorize fourth doses.
In this study, we demonstrate both markedly decreased neutralization in serology assays and real-world vaccine effectiveness in recipients of two doses of vaccine, with efficacy partially recovered by a third mRNA booster dose. We also show that immunity from natural infection (without vaccination) is more protective than two doses of vaccine but inferior to three doses. Finally, we demonstrate fundamental changes in the Omicron entry process in vitro, towards TMPRSS2-independent fusion, representing a major shift in the replication properties of SARS-CoV-2. Overall, these findings underlie rapid global transmission and may alter the clinical severity of disease associated with the Omicron variant.
…
Our estimates of protection in the current GG&C cohort, whose median time since most recent dose is 5 months, were notably lower (Fig.4D). This waning of protection was evident for both variants, leading to very low levels of protection against Omicron in double vaccine recipients of ChAdOx1, BNT162b2 and mRNA-1273 (5.19%, 24.39% and 24.86% respectively). Our estimates for current protection against Omicron in recipients of a third booster dose of BNT162b2 or mRNA-1273 were much higher at 59.21% and 64.9%. We next estimated the additive protective effect of previous natural infection. Infection-acquired immunity directed against other VOCs may be broader in nature and may wane more slowly than that induced by vaccines. The level of protection following previous infection was 53.2% for Omicron, and 88.7% for Delta.
Paper has a bunch more detail along with some cool diagrams and charts. These numbers all make intuitive sense to me.
Meanwhile, vaccines in children are ludicrously effective in terms of reducing what risk is left, a 180x reduction, although they are also largely unnecessary in terms of the kids not having been at much risk in the first place.
Testing
‘Ethical rules’ versus the need to f*** around and find out. We are all poorer for it. We should be able to have very good info on relative performance of different tests, in particular. Here’s some new results, which suggest that nasal swabs are slow to start turning positive, in the study median additional time required was 3 days after the PCRs were positive, which is in the range of not being all that useful if you need to confirm you’re not infectious. Suggestion is to use saliva for rapid tests to get that time back, but by the time we do that, I’m assuming the wave will already be over.
Combined with a lot of anecdotal reports I’ve seen, I’m moving towards assuming that while rapid tests are probabilistically very useful, transmission with Omicron is much faster and has outpaced the speed at which the tests turn positive, and this means that if you want to be confident rapid tests are not that useful on their own. And strongly agree with Mina that if you have symptoms, you have to act as if you’re positive unless you’re negative several days later.
As it usually goes when we are scared of public reaction and use price controls rather than ration to those who value something the most, here is the ongoing quest for Binex tests.
Hospitals
Report of hospital telling employees to return five days after first symptoms or positive test unless they have ‘true Covid symptoms,’ and otherwise being forced to work while sick, including with those true Covid symptoms.
Hospitals in DC risk being overwhelmed and going into crisis care mode, but have seen few deaths. They’re bringing back Covid-positive staff quickly, and offering increasingly rich shift bonuses of $1000 or more.
Hospital admission growth rates in UK, London has gone negative and we are clearly past peak growth. The danger is always that if you get close to the edge you start turning people away and then the graph is misleading you.

Report from NHS, seems consistent with previous reports.
Threads and Posts
Your Local Epidemiologist brings us the good news, general summary post. All seems right, good summary, nothing new.
Look at the impact of Omicron on cancer treatment.
Eric Topol breaks down the details of why our immune systems have been dealing with Omicron so well.
An argument moderately against Omicron coming from Gain of Function research, including what new information would move the needle.
WHO being an unhelpful broken record.
Probability Updates
I want to explicitly encourage people to say in the comments which predictions you disagree with, what your probability is, and what your model is that is causing you to disagree. Especially on China.
China keeps daily cases under 50 per million through 2022: ?% → 40%.
I talked about this above, and expect to update this soon more on better thinking and others’ opinions (including prediction markets if we can get one) rather than primarily through new information. We’ll know if this is failing, but in most worlds where this fails it doesn’t fail right away, so short term lack of evidence of failure is only weak evidence of long term success. I’m mostly throwing this out to start a conversation.
Median peak cases day for United States: ??? → January 19, 2022
Mode peak cases day for United States: ??? → January 19, 2022
Daily cases in the the United States have peaked by February 1, 2022: 85% → 90%.
I think this is better than more probability estimates here. Note that the most likely path is that the median updates to somewhat later as we continue to see case growth, rather than me expecting the peak to be the next day as a median and then the next day we get a peak, we get an asymmetrical distribution. The mode is more likely to stay where it is or not move much, and will likely quickly become ‘any day now’ if it doesn’t happen when I expect.
With some areas already peaking we can be more confident the peak will come in January, but not super confident until we see it in more places more definitively. There’s still a lot of error bars.
Will There Be a Federal Mask Requirement on Domestic Flights as of November 8, 2022? 50% (unchanged, no new information).
Chance that Omicron has a 100% or bigger transmission advantage in practice versus Delta: 55% (unchanged, no new information).
Chance that Omicron is importantly (25%+ in the same person) less virulent than Delta: 90% → 95%.
Chance that Omicron is vastly (75%+ in the same person) less virulent than Delta: 25% → 30%.
Time keeps passing and we keep seeing the same patterns, I think we can safely say that it’s importantly less virulent, I’m keeping the 5% around mainly for model error (e.g. maybe my reasoning is bad). I’m up to 30% on there being a big difference based on the large disconnects in deaths, including in the United States.
Chance we will be getting boosters modified for Omicron within 6 months of our previous booster shot: 20% (unchanged, no new info)
Chance we are broadly looking at a future crisis situation with widely overwhelmed American hospitals, new large American lockdowns and things like that: 5% → 3%.
The big cities, especially the blue ones, are going to get through this, and I don’t see any way big lockdowns happen based on the needs of rural areas.
Generation time (serial interval) of Omicron is 3.5 days or less: 87% → 90%.
Creeping up a bit on reflection and on everything continuing to fit the pattern, especially the reports of rapid tests not picking up on the newly quickly infectious. Pretty confident here at this point, but don’t know we’ll ever confirm this.
It's worth noting that the CCP staked a strong claim to being superior to other governments on their ability to contain the virus they deny having made. Their 50-cent army of propagandists have been incessantly crowing about how great the CCP is for being able to effectively stamp out the virus that brought the mighty US down. There is a lot of face to be lost if this achievement was to fail in a visible way, and in China face is everything. And of course the CCP can also fake almost every number that comes out of China.
Given the above I would not be surprised if their currently low numbers were a stage of denial, when there is already enough Omicron going around but still low enough to pretend that containment works. At some point the mass infection wave might become impossible to hide but even then they might just stop testing and pretend it's just some sniffles, not the big bad Covid.
A lot of strange things can happen in China.
Re. China containment – I would be extremely surprised if daily cases stay under 50p/m this year. I put it at 15%.
I think Australia's experience in 2021 is a reasonable (if imperfect) analogue here. For the first half of the year, it was completely intent on keeping cases at zero. With lockdowns, closed borders, and lots of restrictions, it was able to do this effectively. Then Delta arrived, and everything became much harder. Even with prolonged lockdowns, fairly good contact tracing, and stringent isolation requirements, cases continued to climb. By late August, it hit 50d/cpm (despite most of the country still having no community transmission), and has rarely dropped below since. I think this point is instructive because when Australia first hit 50d/cpm (Aug. 28), it was still very much pursuing something close to a zero-COVID approach; on that date, the lockdowns in Sydney and Melbourne still had another 43 and 54 days to run respectively. Once it became obvious that cases were never going back to zero, harsh restrictions became more difficult to justify, and most people accepted that some form of 'living with COVID' was the only viable approach. Now, Australia is at over 3,000d/cpm.
I expect Omicron to do to China what Delta did to Australia. China mostly managed to contain Delta (which, admittedly, I wouldn't have predicted), but Omicron raises the bar. Delta made everything harder – Omicron makes things near-impossible. Very roughly, I would say that the original COVID strain was a 3/10 to contain, Delta was a 6/10, and Omicron is a 9.5/10. Australia's zero-COVID dreams died at 6/10; I don't think that China's withstand 9.5. From what I've read – and on current form – it does seem likely that the Chinese population will continue to accept containment measures that would be unworkable almost anywhere else, and so that does add a little uncertainty. But even with the toughest of restrictions, I still struggle to see cases staying that low. 50d/cpm is only 70,000 daily cases, in a country that has 65 cities of 1m+ people.
That’s how I end up at 15%. I'm tempted to go even lower, but China is unique in a lot of ways, and I’ve been surprised by it before. Also, by terrifying its citizenry and mocking the West for its COVID-tolerance, the Chinese government has really backed itself into a corner on this. To lose control now would be incredibly embarrassing (particularly in the year of a Party Congress), and so I expect the CCP to do all it can to avoid an about-face.
But I’m not betting against Omicron here.