Omicron Post #4
The possibilities narrow.

Previous Omicron updates: #1, #2, #3. Last weekly non-Omicron update.
An introductory word: Thanks to Dominic Cummings, I have a lot of new readers, many from the United Kingdom, so I want to welcome all of you, and I hope at least some of you will stay when I turn to non-Covid questions. I am American so these posts focus on the United States, but I keep an eye elsewhere too, and mostly we’re all in this one together and the same conclusions apply. If you have good news sources and follows to keep a better eye on the UK or Europe for Covid purposes, or data sources anywhere I may not have noticed, I invite you to share them in the comments.
The constant refrain from all sources is ‘we will know more soon.’ Soon is continuously arriving. The new information we are learning hasn’t completely ruled out many possibilities, but it is broadly consistent with Omicron spreading fast and having a high degree of immune erosion/escape in terms of infection but not protection against severe disease.
Thus, to headline the core takeaways at the top, here’s broadly where I’m at as of now (probability estimates at the end, as before). I’d be surprised if any of these were wrong.
Omicron spreads far more rapidly than Delta and is going to take over.
This will come at us fast. Omicron will be the majority strain by the end of January. This happening by end of year is on the table.
Omicron re-infects those who have already been sick, or breaks through to those who have been vaccinated, much more than Delta.
Previous infection continues to protect against severe disease, hospitalization and death.
Omicron doesn’t cause substantially more severe disease than Delta when it infects you, but we don’t know if it causes less severe disease yet, our evidence is ambiguous.
Omicron cases on average are much more mild because there will be a much higher percentage of re-infections and breakthrough cases, which are highly protected against severe disease.
The big peak is probably within a few months, so you don’t have time to wait for an Omicron-targeted shot. The current shots will still work against severe disease, so strongly consider getting vaccinated or boosted if you can.
The best thing we can do to minimize the harm Omicron causes is to ramp up production of therapeutics, especially Paxlovid, as rapidly as possible, along with the necessary tests and other logistics to get the treatments to people in time to matter. The goal is mitigation at this point, not prevention.
There is going to be a period early in 2022 when there are quite a lot of Omicron cases, such that it will be difficult to remain uninfected and it will likely be difficult to get any kind of medical treatment at a hospital. Be ready.
Also be ready in case of lockdowns and other government restrictions, especially if you live in Europe where they’ve shown a willingness to use them. And if you’re immunocompromised or otherwise at high enough risk you need to be sure to not get Omicron, then the price of success is getting super paranoid soon and lock down hard, for at least several months.
In Search of Bayesian Evidence
How rapidly does Omicron spread? How far has it spread already?
Any given infection or reported group of infections, or even piece of data, is unlikely to be conclusive. But each one does have a likelihood ratio of how common it is to witness it in worlds where Omicron will spread extremely rapidly in the West, versus worlds where Omicron doesn’t do that. Similarly, they have ratios for how often how much of that comes from immune escape versus baseline infectiousness, how much protection remains against severe disease and death, and what the baseline severity of Omicron is.
Then we need to consider what we saw relative to what we expected to see. In general, no news is good news. If ‘nothing happens’ regarding Omicron, that continuously makes us less worried, whereas most news will make us more worried. Getting a constant string of bad news is expected, but how much of it did we get, how fast and how bad?
A lot of that depends on the extent to which various jurisdictions are looking for news. Taking a Trump-like approach of ‘if you didn’t run the tests you wouldn’t have that many cases’ does successfully postpone the bad news for at least a few days, and sometimes several weeks. All reports need to be adjusted for the amount of effort being put into finding data and generating reports.
The South African Study
Title and link: Increased risk of SARS-CoV-2 reinfection associated with emergence of the Omicron variant in South Africa.
This preprint was the first study about Omicron, and it doesn’t hold back. Author has a thread here.
Here’s the results section.
35,670 suspected reinfections were identified among 2,796,982 individuals with laboratory-confirmed SARS-CoV-2 who had a positive test result at least 90 days prior to 27 November 2021. The number of reinfections observed through the end of the third wave was consistent with the null model of no change in reinfection risk (approach 1).
Although increases in the hazard of primary infection were observed following the introduction of both the Beta and Delta variants, no corresponding increase was observed in the reinfection hazard (approach 2). Contrary to expectation, the estimated hazard ratio for reinfection versus primary infection was lower during waves driven by the Beta and Delta variants than for the first wave (relative hazard ratio for wave 2 versus wave 1: 0.75 (CI95: 0.59–0.97); for wave 3 versus wave 1: 0.71 (CI95: 0.56–0.92)).
In contrast, the recent spread of the Omicron variant has been associated with a decrease in the hazard coefficient for primary infection and an increase in reinfection hazard coefficient. The estimated hazard ratio for reinfection versus primary infection for the period from 1 November 2021 to 27 November 2021 versus wave 1 was 2.39 (CI95: 1.88–3.11).
Extending the period back to 1 November is going to decrease the magnitude of this effect somewhat, although case numbers in the earlier pre-mostly-Omicron period of November were low.
The study notes that it is studying reinfection risk rather than vaccine breakthrough risk, but the two should be highly correlated.
It looks like the study’s method was to match IDs of current infections to previous infections.
One worry is that this might fail to control for immunity declining over time since infection, beyond the 90-day window where reinfection risk is assumed to be zero. Given that they calculated no additional reinfection risk for Delta up through October, presumably this effect can’t be anything like big enough to explain the results.
Another note is this only counts infections that were detected on both occasions, which could have some interesting effects. Mostly I think this should undercount the rise in reinfections, because more of the control group were actually previously infected without knowing it, which is effectively a multiplier effect on the real odds ratio.
Here’s the key chart:
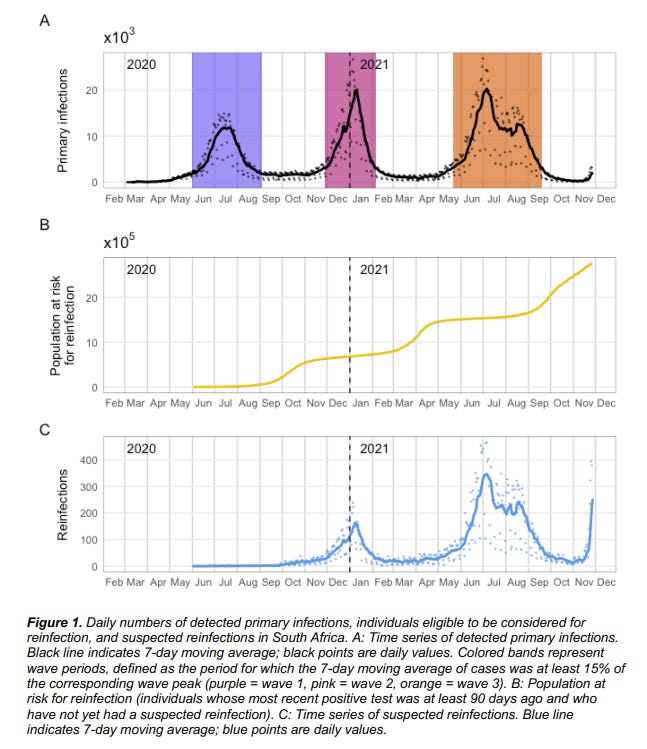
This is naked-eye obvious. The population at risk for (known) reinfection is roughly double what it was before, yet the ratio of reinfections to other infections is clearly much higher than that.
Also note that this finding rules out the possibility that most South Africans were already infected. If that was true, then being known to have been infected wouldn’t provide much additional protection.
They give us numbers that should be easy to work with, file under Huge If True:
The mean ratio of reinfection hazard to primary infection hazard decreased slightly with each subsequent wave, from 0.15 in wave 1 to 0.12 in wave 2 and 0.09 in wave 3.
The mean ratio of reinfection hazard to primary infection hazard for the period from 01 November 2021 to 27 November 2021 is 0.25.
Note that protection from an Omicron infection, for a future second Omicron infection, would probably still return to previous levels.
I am inclined to mostly believe this result, as it is broadly consistent with other findings.
Denmark
Link is to Washington Post report on Denmark’s huge jump in sequenced Omicron cases. Denmark does a lot of sequencing, so them finding a lot of cases first is a sign things are far along.
The number of confirmed cases in the country rose from 18 on Friday to 183 on Sunday, reflecting both the speed at which the variant has spread and the sensitivity of Denmark’s virus surveillance system.
The northern European country is a leader in the sequencing of variants, acting as an early-warning system for the continent.
…
Health authorities in the country of 5.8 million perform more than 200,000 polymerase chain reaction, or PCR, tests per day — one of the highest rates of tests per capita in the world. Positive tests are submitted for special PCR tests that detect variants. For those that come back positive, scientists sequence the whole genome. Denmark sequences 25,000 strains per week, Lillebaek said.
…
Danish media reported that some of the infections were traced back to a concert in late November and a Christmas lunch involving 150 guests.
Britain also reported a sizable uptick in omicron cases: 86 new cases on Sunday, bringing the total number there to 246.
Attempts to trace Omicron cases are helpful, but in terms of knowing where we stand they can also corrupt the data. If Denmark was about as likely to catch an Omicron case of a given severity as a Delta case, and was sequencing all its 4300 tests a day (its 7-day average of positive tests), and got back 183 positive cases in a day, that would mean 4% of cases were already Omicron, and given what that would be saying about exponential growth, we’d expect to cross 50% within two weeks.
The question is, if we hadn’t been doing this extra tracking of Omicron cases, how many of the Omicron cases we did find would have been missed? If we don’t discount those, we’re going to get an overestimate, and of course Saturday could have been an outlier due to timing of data collection. If we catch every Omicron case, then we’d have to discount by the percentage of Delta cases that get missed, which is unknown, in addition to adjusting for exact timing. Even with a lot of testing I’d presume 50%+ of cases are missed, and plausibly 75%+. Denmark’s cumulative case rate is only 8.8% for the entire pandemic, so this ratio could be quite high.
What we do know is that up until a few days ago, they sequenced every positive test and found zero Omicron cases. Now they’ve suddenly found 183 in a single day, 4% of average daily positive tests.
Superspreader events are a thing, so it’s possible that this is luck, but there aren’t a bunch of other Denmark-like countries that also do all this sequencing, so there was only one ‘shot’ at this happening in this way. It’s a sign of very rapid spread.
Hopefully we will also track outcomes from the group, to help us learn about severity. The numbers are starting to get big enough that they’ll tell us something, but that still requires time for cases to develop.
Anime NYC
The Omicron timeline needs to be moved up substantially, because the case that we found in Minnesota was a case of community spread, probably at a large Anime convention in NYC, and on November 19-21, which predates the identification of Omicron.

The case was not only vaccinated but boosted, and a majority of the friend group later tested positive. Things are escalating quickly, and we’re not making that much effort to find cases. This was identified as Omicron as part of a random sampling rather than any reason to suspect the case, which is also worrisome, and there was still an 8-day delay involved. Ouch.
Our awful mayor issued this statement afterwards, along with others who urged those in attendance to get tested.

But look at the timing. They’d all already been infected over a week ago. What’s the point?
Boston
This is a graph of the amount of Covid found in the wastewater in Boston. If you have links to similar other measurements taken regularly, share them in the comments.
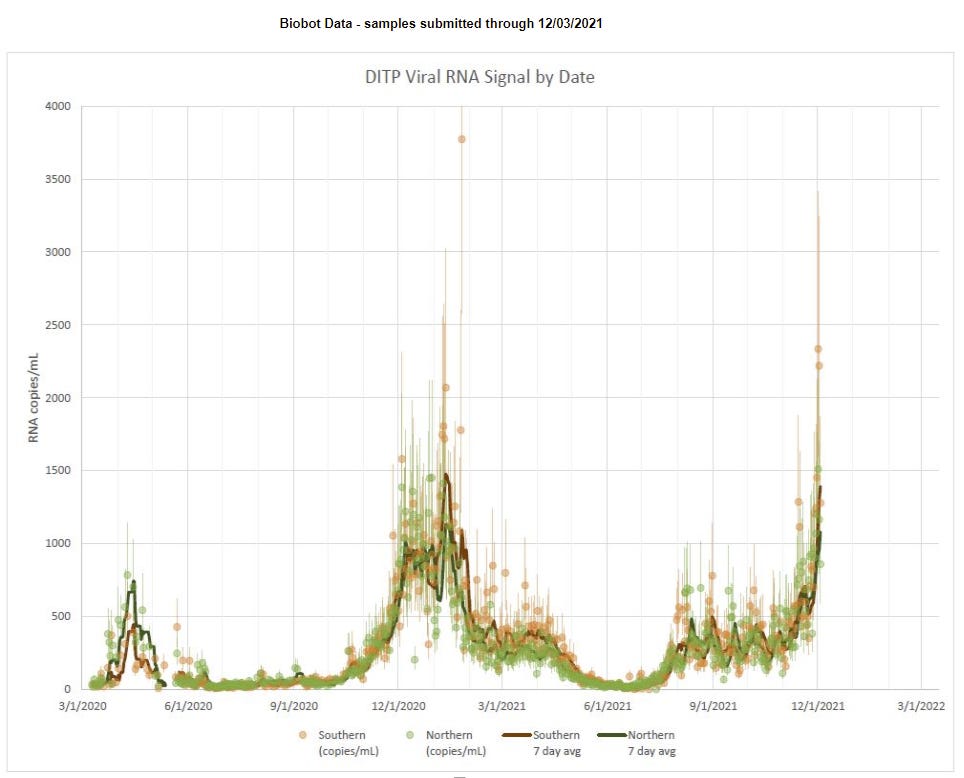
That spike on the right has two of the three highest single-day measurements, and they were the last two days of data reported. This can’t represent Delta cases alone unless it’s a data error, because the rise is too rapid given what we know about conditions. If it’s Omicron and the measurements are what they superficially look like, it means Omicron is already primary in Boston, and there’s a huge spike in infections already, that hasn’t been matched with a surge in hospitalizations or positive tests.
There are other outlier measurements on the graph, so probably these are outlier measurements. But if they hold up over the next few days, then what would that mean?
If they hold up and there isn’t a wave of new hospitalizations quickly, then this is the best of all possible worlds. Omicron would be spreading like wildfire, but be much milder than previous waves. We’d be able to get through it quickly, and have no realistic way to prevent it, so all we could do would be to shield the vulnerable to the extent we could, use what treatments we have that we can get to be legal, and come out the other side.
If they hold up and then the hospitalizations follow then things are quite bad, it’s hitting us now and we’re in a crisis situation. There will be pressure to do very foolish things to try and stop something that will be utterly impossible to stop, and Paxlovid will arrive too late to make much difference.
If they don’t hold up, that’s mostly what I expect. Either it’s bad or weird data, or Omicron somehow puts a ton more virus into the wastewater, and then there’s nothing to see here. That’s what I mostly expect, but note that the measurement happened in both the north and south sections, which didn’t happen on the previous big fluke measurement.
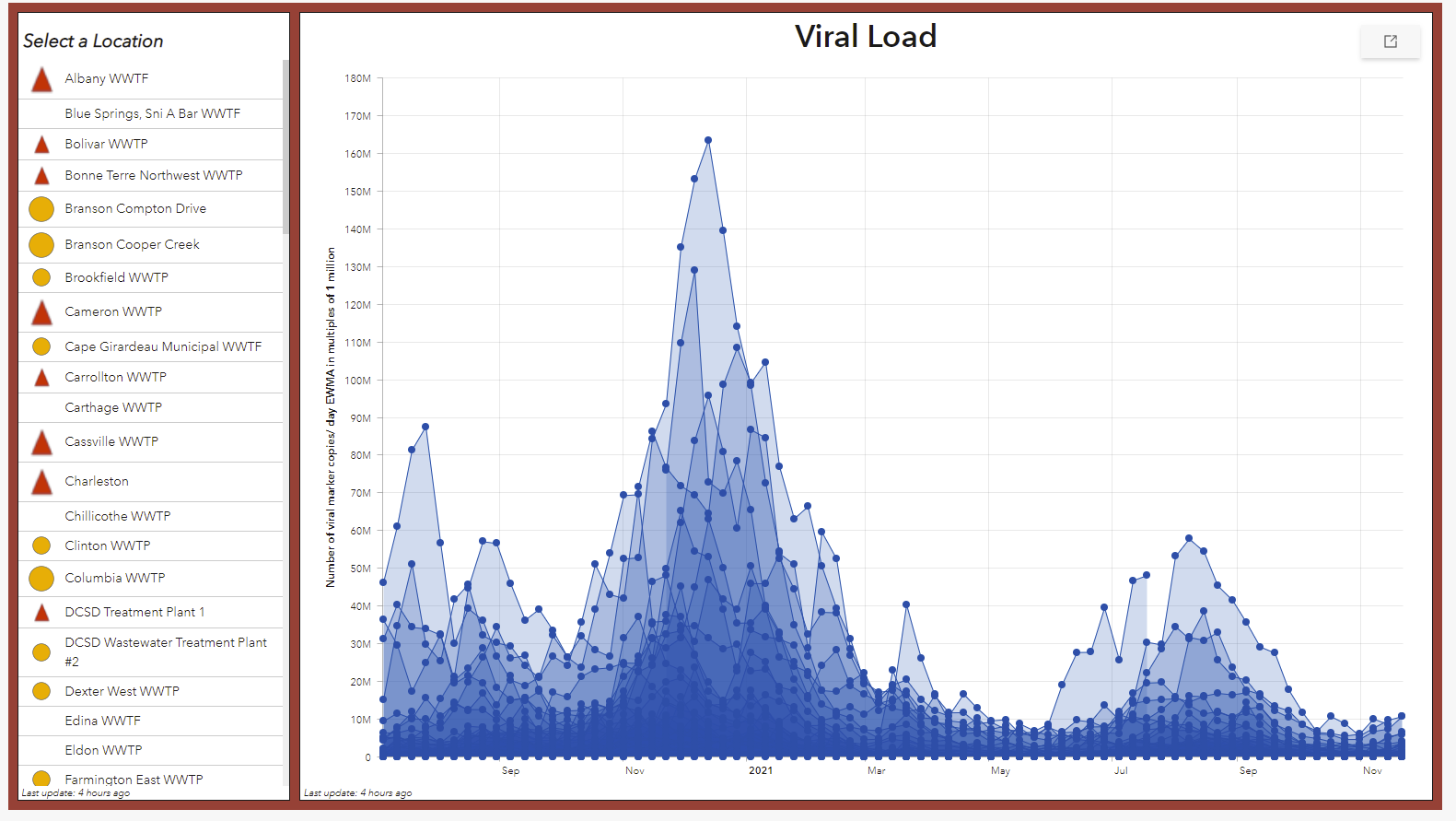
Here’s a graph in Missouri that doesn’t yet show a similar spike, but is updated less often and is from a less internationally connected area. As you’d expect, no spike.
There’s also this Dutch source, which shows no spike yet.
Unfortunately that was the only other ones I found so far. There’s implications in the next section’s threads that such data is available for the UK but I’m not sure where to find it.
SGTF in the UK
Oops. As of December 3.


Too Little, Too Late
Scott Gottlieb warns us not to act prematurely, despite it already being too late:
Noting that companies, including Pfizer, were doing so, Gottlieb said, “This is going to be a really critical decision because what we've seen in the past, for example, when we engineered a vaccine to specifically target 1351, the old South African variant, was that vaccine worked well or appeared to work well against 1351 but didn't appear to provide as good coverage against all the other variants.”
“And there's reason to believe that as you develop vaccines that are very specific to some of these new variants, they may not work as well against the full complement of different variants that we've seen. So you wanted to try to stick with the ancestral strain, the Wuhan strain, in the vaccine, I think, as long as possible,” Gottlieb continued.
I don’t want to pick on Gottlieb because he’s better than most, but this is emblematic of a system that never acts in time when it matters. Given the logistical timelines involved, even if we made a full best effort starting today, we'd largely be too late getting the new Omicron vaccines to those who need them. Waiting until Omicron is already dominant or far enough on its way to make it the kind of obvious being looked for here is a way for exponential growth to laugh in your face every single time.
Exponential growth doesn’t permit one the luxury of being exactly on time. Either you’re too early or you’re too late. You either move now and have some chance to do some good, or you’re way too late.
Here’s another Washington Post headline showing the extent to which we will get there too late and with too little.
New coronavirus vaccine may eventually be needed for omicron variant, BioNTech CEO says
…
“I believe, in principle, we will at a certain time point need a new vaccine against this new variant. The question is how urgent this needs to be available,” CEO Ugur Sahin told a conference hosted by Reuters.
He also said the current vaccine could be adapted “relatively quickly” if needed to combat the omicron variant, but cautioned that more research was still required.
If that’s the attitude of the CEO of BioNTech, that should both put to bed any rumors that the vaccine companies are trying to trick us into taking extra vaccines to make them more money (which was already absurd, and no doubt will never be put to bed no matter the evidence, but shrug) and also put to bed the hopes that the new doses could arrive in time. This essentially indicates that the serious push will only begin after Omicron is a large share of cases and then it will be far, far too late.
Similarly, here’s the head of the CDC saying true things that complete miss the point and the urgency.
“We know we have several dozen cases and we’re following them closely. And we are every day hearing about more and more probable cases so that number is likely to rise,” Walensky said on “This Week.”
If something is certain, it is also probable.
“We have about 90 to 100,000 cases a day right now in the United States, and 99.9% of them are the delta variant,” Walensky said.
This is probably true, although I think there’s a non-trivial chance Omicron is already over 0.1% of cases, but it won’t stay true for long and isn’t all that relevant.
South Africa

The person linking to this thought it was bad news, but given the rate at which cases are increasing, it looks to me like good news. Not easy to interpret, but the hospitalization rate per infection is what matters here. Note also that positive test rate is now >20%, which means a higher percentage of cases are being missed than before.
Here’s some South African data by province:
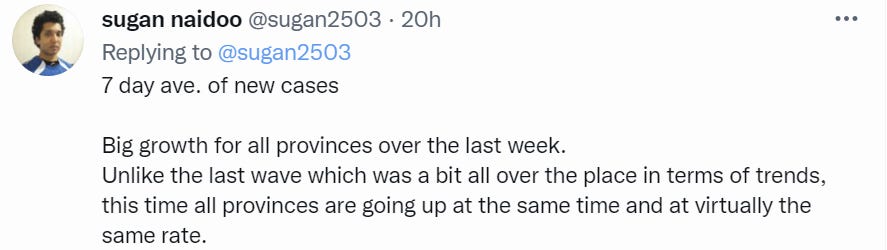

If I’m reading both charts correctly, the ratio here seems quite good, actually.
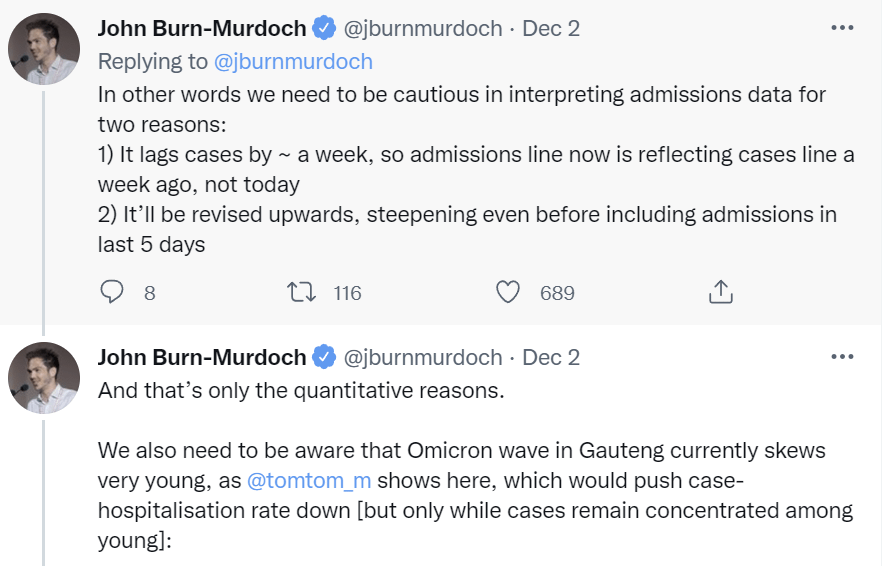
The December 2 version of the summary graph from Gauteng.
The thread that was in gives some caveats on the hospital numbers, they get revised upwards later and lag cases, but still.
Then here’s the chart from December 4.

Preliminarily it looks good, but I still don’t feel we can conclude anything.
Here is a summary of patient profiles from Gauteng. In general, the patients are healthier than one would expect, even accounting for age. I found this especially interesting:
In summary, the first impression on examination of the 166 patients admitted since the Omicron variant made an appearance, together with the snapshot of the clinical profile of 42 patients currently in the COVID wards at the SBAH/TDH complex, is that the majority of hospital admissions are for diagnoses unrelated to COVID-19. The SARS-CoV-2 positivity is an incidental finding in these patients and is largely driven by hospital policy requiring testing of all patients requiring admission to the hospital.
Think about what this implies. If a majority of the cases that have Covid-19 were admitted to the hospital for unrelated reasons, then either Covid is somehow causing all these ‘unrelated reasons’ without making the patients sick with Covid in an obvious way, or the chance of hospitalization in the window when you have Covid less than doubles. You’re more likely to be admitted to the hospital and happen to have Covid, then for Covid to send you to the hospital.
If that’s true, then that seems like a very mild disease indeed. Anyone else want to take a shot at interpreting the data here?
Case Numbers Going Up
There was a superspreader event in Oslo.
OSLO (AFP) - Norway introduced new anti-Covid measures in greater Oslo on Thursday (Dec 2) after a suspected cluster of Omicron cases emerged among dozens of vaccinated people.
Face masks will be mandatory in public transport, shopping centers, shops and taxis when social distancing is not possible.
People will have to work from home if possible and the number allowed to gather at private indoor events will be limited to 100, the government said.
The announcement came after the Omicron variant was detected in at least one of "50 to 60" people who tested positive for Covid-19 after a Christmas dinner in Oslo last week.
That represents about half of the 120 people - all vaccinated - who attended the event organized by solar energy producer Scatec.
Superspreader events are outliers by definition but that’s almost half of the people attending all of whom were vaccinated. I do not believe that is a thing that could have plausibly happened under Delta. They haven’t officially confirmed these were all Omicron cases yet, but it seems unlikely they aren’t mostly or entirely Omicron.
The response of tightening restrictions in the area seems unlikely to accomplish much.
Other Threads and News
Noah Smith’s second summary thread. I intentionally read this last. It’s solid, but doesn’t contain much additional information.
Thread illustrating the range of possible properties of Omicron, and how its infectiousness interacts with its immune escape properties. Correctly suggests that any efforts need to start now to have any chance of arriving in time. Doesn’t think Omicron is likely to be less infectious, but that seems like it was mostly priors.
Jose Caballero thread from December 2.
Poll claiming that Americans are quite open to additional measures against Omicron.
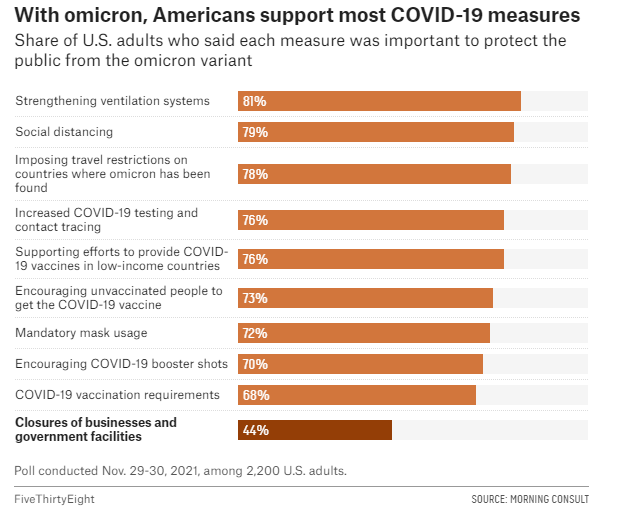
Note how crazy it is that there are 68% of people support mandatory vaccination but only 70% (2% more!) people support encouraging booster shots. There are almost no people with the ‘encourage people to do useful things but don’t force them to do those things’ position. Sigh.
Bad news on monoclonal antibodies (WSJ), but isn’t surprising given what else we know.
An attempt to synthesize what we know while incorporating Metaculus predictions, from December 2. Included for completeness, but nothing new or surprising.
Probability Updates
Chance that Omicron has a 100% or bigger transmission advantage in practice versus Delta: 35% → 65%.
Note that I am interpreting this as ‘in practice in the United States of America,’ or in Europe, rather than the transmission advantage in an immunologically naïve person.
We have the growth in cases in Denmark and around the world, the paper from South Africa, the continued case growth in South Africa, the wastewater in Boston (even if I’m not sure if this is ‘real’ yet) and the superspreader events in Oslo and at Anime NY. We have cases being found within a few days, in multiples, from nothing, across most countries that checks for cases.
After a certain number of exponential curves, it’s hard to deny what you are looking at. I’m not willing to go super high on this yet because 100% is a very high threshold, and variants often have large advantages when they are first spreading that don’t carry over to later on, but this seems more likely than that.
Chance that Omicron will displace Delta as most common strain: 85% → 95%.
With the extent of immune escape we’ve seen and the rapid growth in cases, I don’t see a plausible path to this not happening. The likelihood ratios this week were very high, and model or systematic error is the reason I’m not going higher than this.
Chance that Omicron is importantly more virulent than Delta: 8% → 5%.
Chance that Omicron is importantly less virulent than Delta: 35% → 50%.
If Omicron were more virulent than Delta that would make our observations so far very unlikely. It’s not impossible that this is the case and the huge number of young people infected and number of breakthrough infections and reinfections are disguising it, but this becomes less likely over time.
With respect to being less virulent than Delta, there’s a bunch of suggestive findings that have cases or implied cases rising without a rise in hospitalization. I am increasingly hopeful that we did indeed get lucky on this and anyone saying ‘no evidence’ here has very little leg to stand on.
However, I still think this is only a coin flip, because the data we have is too confounded by too many factors, as discussed above.
Chance that Omicron is importantly immune erosive, reducing effectiveness of vaccines and natural immunity: 80% → 95%.
Will the CDC label Omicron a variant of high concern before 2022? 15% → 13%.
The data on immune erosion seems very clear. There’s enough uncertainty it’s not fully over (and I am moving fast enough that I admit I’m not being all that principled or accurate in my various 5% chances here in terms of exact percentage) but I don’t see how we get the data we’re getting without this being the case.
As for the label of high concern, that’s a question of how and how fast the CDC works and I grow increasingly skeptical that they will ever do anything with speed, and the prediction market on this has been up for longer as the deadline grows closer.
Chance that Omicron means the vaccinated and previously infected are no longer effectively protected against severe disease until they get an Omicron-targeted booster shot: 3% → 2.5%.
The data doesn’t make sense if this is false but I don’t want to get too confident too quickly.
Chance we will be getting boosters modified for Omicron within 6 months of our previous booster shot: 30% → 30%.
It looks like it will take three months to complete the whole process and get the new vaccine formulations approved, at which point boosters will become available, and by the time any given person can in practice get a shot, it will likely be more than 6 months after their last shot unless they delayed on the booster quite a bit, which likely means they’re not high priority. So my guess is in practice this won’t happen, but the whole thing is odd and ambiguous. I should likely formulate a more precise question that better answers what we care about.
Chance that Omicron is less vulnerable to non-antibody treatments like Paxlovid or Fluvoxamine: 3% → 3%.
No new information.
Chance we are broadly looking at a future crisis situation with widely overwhelmed American hospitals, new large American lockdowns and things like that: 12% → 17%. EDIT: Should have been at least 25%.
I’m going back up on this based on a higher certainty that Omicron is the real deal, and the higher chance it’s a very fast version of the real deal that is likely to peak quite high and overwhelm the hospitals temporarily. If that happens, there’s going to be a lot of pressure for extreme measures. What’s keeping this from rising more is the possibility the cases will remain mild.
EDIT: Commenters pointed out that while this seemed like a big adjustment, it definitely wasn't enough and the other updates implied a bigger change, to at least 25%, depending on the exact definition and how many components need to apply.
Will Omicron be >1% of all cases by the end of the year? 70% → 93%.
The market on this is trading too low. There’s very little chance this does not happen given the new timelines. There’s still some uncertainty here, but it’s declining rapidly, and it’s mostly model uncertainty.
Is there any good evidence so far about Omicron severity for children under 5?
My prior is “about the same as Delta”, but good data for this sub-population is sparse.
Obviously many people care quite a bit about the answer to that - even if the rest of a household is vaccinated, it’s hard not to worry about small children who can’t get the vaccine yet.
I will point out that the fast-food business is more about real estate than food. Getting the best locations for your stores is something of a moat.