I wouldn’t have explained or modeled it quite the way Paola does here but the principle seems right to me. If people don’t trust you, or don’t trust people in general, that usually you can’t trust them either.
Paola: I feel like a lot of human morality works like a prisoner’s dilemma in that you can only trust others to behave morally to the extent that you believe they trust you to do the same. Due to this, I’ve come to view people with a bunch of social paranoia, distrust, etc. as *quite* dangerous to be around.
And to be clear, I generally feel a decent bit of sympathy towards people like this. I think *I* am perhaps more than average prone to this paranoia cluster. But I do really think it’s a thing to strongly avoid letting yourself fall into or being near in any way.
Naked Capitalism considers The Hypersociality Hypothesis, which is the latest take on the cluster of things that includes Moral Mazes and The Inner Ring, with link back to my old post from 2021 about Why I Am Not In Charge of the CDC.
This variation is that there is everywhere a clique of people who are:
Exceptional at sending and receiving social cues.
Intelligent but not interested in complex or abstract analysis.
Exceptionally willing to conform to surrounding social cues.
These people then form what I have called The Implicit Coalition, the alliance of all of those who are focused on advancing in the hierarchy (which he calls Pursuing The Main Chance) and rewarding alliance membership and punish all non-members, or what C.S. Lewis calls The Inner Ring. By default any organization gets increasingly taken over and run by this group over time, and they control many social perceptions including most shifts in various versions of the Overton window.
I think of these descriptions as different Fake Frameworks grasping at the same underlying elephant.
Wolfers suggests better price transparency, up front in the process, and especially on markups. I can get behind that, to reduce search costs, although on average it won’t save customers money because prices will adjust.
The reasons we check the prices anyway are primarily two-fold.
Good virtues and habits. You want to cultivate not wanting others to price gouge you or take unfair advantage, or letting the little extra fees add up.
You’re investing in knowing how to get the best price, and many orders will be effectively repeated, at which point you can lock in your method.
JD Vance, the person most likely to be our next president, is loudly being rather ignorant and terrible on economics in his new book, outright calling to not think economically. Given what we know about him, this is a conscious decision by Vance. To be fair, the book’s main topic is Catholic conversion, and the Pope while good on ethics is far worse than Vance on economics, although in entirely different ways.
Good Advice
Use air conditioning and also heating. The exact optimal number doubtless varies by person and task, but we can easily simplify it by ‘not super hot and not super cold.’
Jonah Goldberg: The human brain works best at 68 degrees Fahrenheit. That’s why offices need to be cold.
Rob Henderson: “For every degree above 25°C (77°F), our cognitive performance declines by around two percent. And if synapses suffer, so does economic activity. At 30°C (86°F), office performance drops by almost 9%.”
If you are very intelligent, beware getting caught too permanently in some worthless rabbit hole. You have to pick a useful rabbit hole.
BlockHead4000: The smartest guy I’ve ever known (real legit 150IQ+ unlike all the liars on Twitter) spent his time on history forums and working on a YouTube channel where he found every bug in the Vanilla Skyrim map and documented them. It got 0-50 views.
Casey Handmer: My impression is that our society has no idea how to metabolize curve destroyers, and a lot of them end up either with niche obsessions or extremely grumpy (or both).
A lot of them were streamed into math for essentially salience reasons and the lucky ones became researchers, teachers, or quants.
But now there is another way. You can build the Dyson sphere.
Zac Hill: More people would do well to study the biography of Claude Shannon and his decadal obsession with what were essentially yard ornaments.
I heartily endorse grocery store tourism and enjoy it far more than most of the traditional tourist activities.
Don’t invest your political capital in sketchy people, as Nate Silver says, for a broad definition of both political capital and sketchy. If you know someone is sketchy, there is more sketchiness, and yes the leopard will also be inclined to eventually eat your face. It is almost always worse than you know.
New York versus San Francisco as something similar to sexual orientation. One might say that if you care more about things other than vibes, and focus on vibes vibes you the wrong way, then the San Francisco vibes will be off.
Tyler: Can anyone articulate why the vibe is so off in California and the Bay Area in particular even though it seems like everything is amazing? (beautiful weather, interesting culture, etc)
Aella: i love the vibes here. maybe they’re just not your vibes
The best way I know how to describe it, as a pure New Yorker: I am safe in the coven of Lighthaven, but when I step outside of it I am attacked by paradox spirits.
GiveWell expects to direct >$800 million in 2026, more over time, and is hiringprogram officers at $200k-$300k, remote, US and international.
While I Cannot Condone This
Stolen fries taste better, and the more risk you take to covertly steal them the better they taste, up to 39% better. This included perceived saltiness, crispiness and intensity. Guilt was positively associated with enjoyment. Love it.
Yes, regular people really are bizarre enough that these questions are worth asking. Often they just go with pretty much anything.
“Have you ever shifted in your chair unnecessarily”
“Do you have trouble starting tasks you think are stupid”
There’s also “do you not have focus except for the times you do have focus”
Gillian Branstetter: My favorite one on the autism questionnaire is “do you struggle to accomplish tasks without knowing the reason why the task must be done” because what do you mean the rest of you are just doing tasks without asking why
Kenshin9977: A fitness coach once said he starts with his clients with the absurd exercises just to see what type of person he deals with. The kind that needs to understand or the kind that don’t care at all? So no, the need to understand doesn’t seems relevant for everyone
I do understand how to be in the ‘don’t care at all’ mode, and turning your brain off like that has its advantages, it can be thrilling and I definitely don’t kink shame, but maybe it shouldn’t be a 24/7 experience with no safe words?
There are quite a lot of places you can live without ever getting bored, and relatedly also many places you can indefinitely visit or hang out in. The idea that one would spend a week and think ‘oh I guess that’s all Tokyo, Osaka, London, Rome, Paris or York City (or pretty much anywhere a lot of people father) has to offer since I’m not a niche food traveller’ is rather absurd. You might run out of ‘completely standard high-level non-food tourist activities’ but if that’s your measure you are Doing It Wrong. My pick is still to stay home, but that’s largely because I can hang out indefinitely and oh look, I am already here.
Everything Price Sufferer (but especially eggs): It’s too bad “your boos mean nothing to me I’ve seen what makes you cheer” comes from Rick and Morty because it’s a perfect summation for how shaming, as a tactic, requires a certain baseline moral credibility from the shamer.
Jack: it’s too bad that reputation effects exist, because now I can’t use the best quote I know about reputation effects without adding caveats or people will mistake me for a fan of something low-status.
If you’re not willing to embrace ‘low-status TV’ on the level of something as cool as Rick and Morty, you’re not going to make it.
An argument for Substack as a valid place to Do Philosophy rather than purely relying on journals. As you would expect, I approve. Journal-based philosophy seems entirely unappealing. I especially buy the argument that our best and most influential works of philosophy all look super different from a journal article, and different from each other.
How does a high decoupler deal with a community of low decouplers? The answer involves engaging with such people on their own terms, and knowing what moves absolutely will make the situation worse. You can and must both be a high decoupler, and still notice the couplings that others will draw. Sometimes that means you can’t get the central thing done, and you need to be okay with that.
One way to catch a remarkable amount of fraud is, as Patrick McKenzie suggests, to ‘sort by amount received’ and forward that to the fraud department. Allowing pension spiking and other ‘technically legal’ cheats is also everywhere a policy choice.
Patrick McKenzie: Payroll department sends top payees annually to local equivalent of office of inspector general with a “Hey FYI.”
Ukraine allocates ‘e-points’ to brigades based on casualties and damage they inflict on Russia. Those points can then be cashed in to purchase new systems directly from manufacturers. This is in addition to the many other changes discussed in the article. America’s military takes a decade to fill a precise purchase order, whereas Ukraine has each brigade act like a scrappy startup that ships. One problem is, if you are not in a shooting war, then if you order up a bunch of drones or other things now then by the time you use them they are probably obsolete.
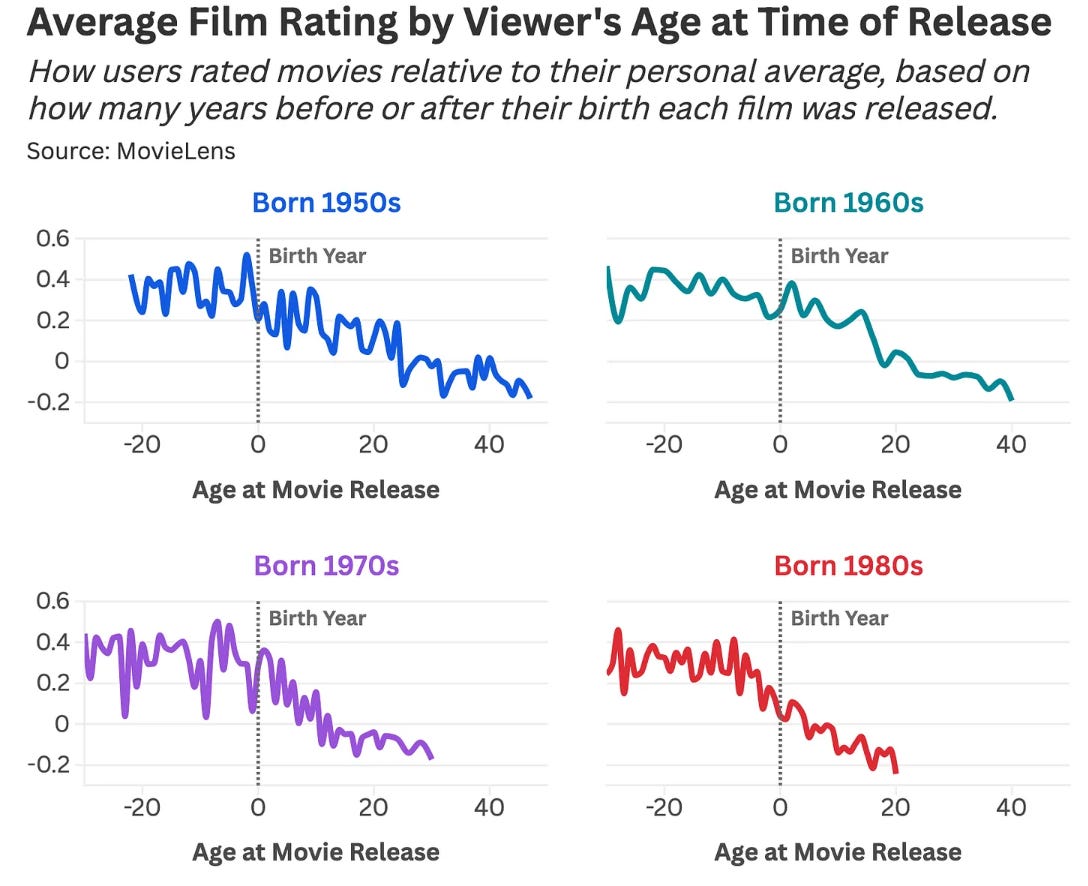
Daniel Parris: Using the MovieLens dataset, we can compare movie ratings by the number of years between a film’s release and the reviewer’s birth. The results suggest that movies were best before you existed, declined around the time you arrived, and have been getting worse ever since—a sentiment consistent across generations.
My hunch remains that a lot of this is selection effects. If you’re watching movies many years after release, you’re selecting the good movies. And these graphs only have a range of about 0.6 on a 0-5 scale, so the effects are big but not out of line with that.
My ‘top rated decades’ on Letterboxd, where I started logging in December 2023, are 1990s (3.91) and 2000s (3.72), then 1980s (3.14). Recent years do worse: 2024 (3.10), 2025 (2.95) and 2026 (2.96), and I’m confident a large portion of that is selection effects.
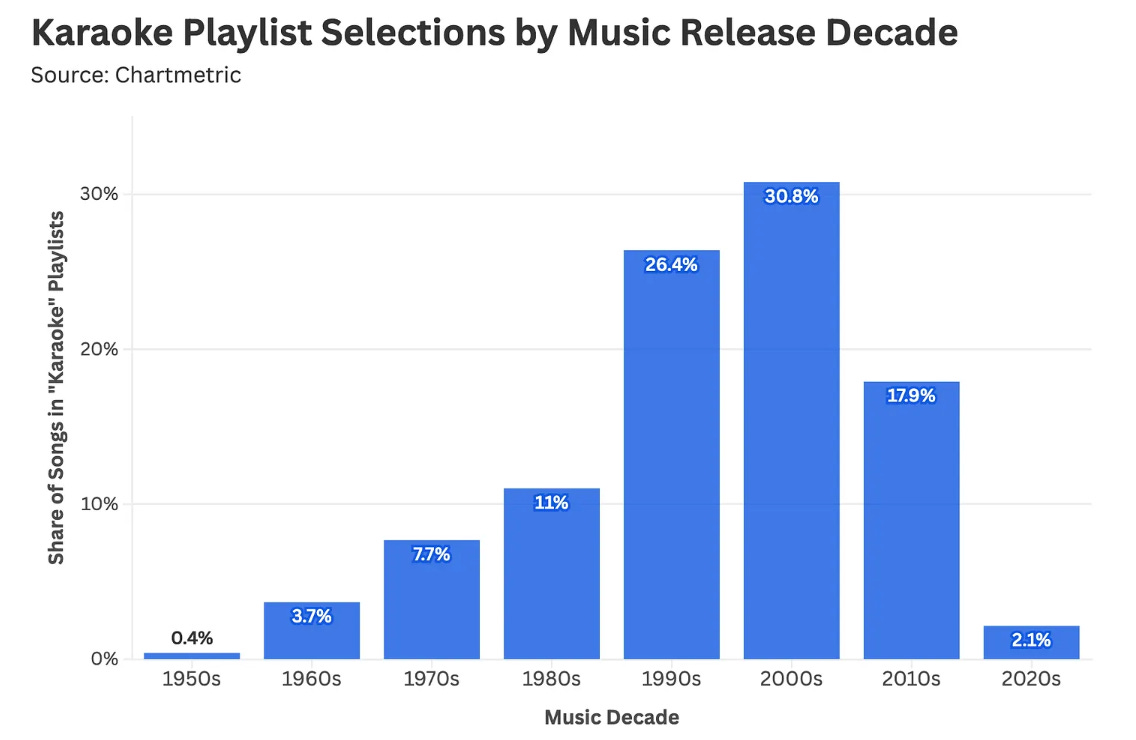
Karaoke tastes have shifted forward to focus on the 2000s, which seems like a clear mistake in general. I definitely underproduce, and underconsume, karaoke, but I would hope we could more often travel further back into the past.
My go to karaoke song, by the way, is Bohemian Rhapsody.
I strongly agree that we need to return to producing TV shows that run 22 episodes in a season and produce a season every year. There is so, so much value in high volume and spending lots of time with the characters, including filler episodes, even if average quality suffers. It encourages building rich worlds that you want to live in, rather than going quickly through a particular story, which also helps build for future seasons.
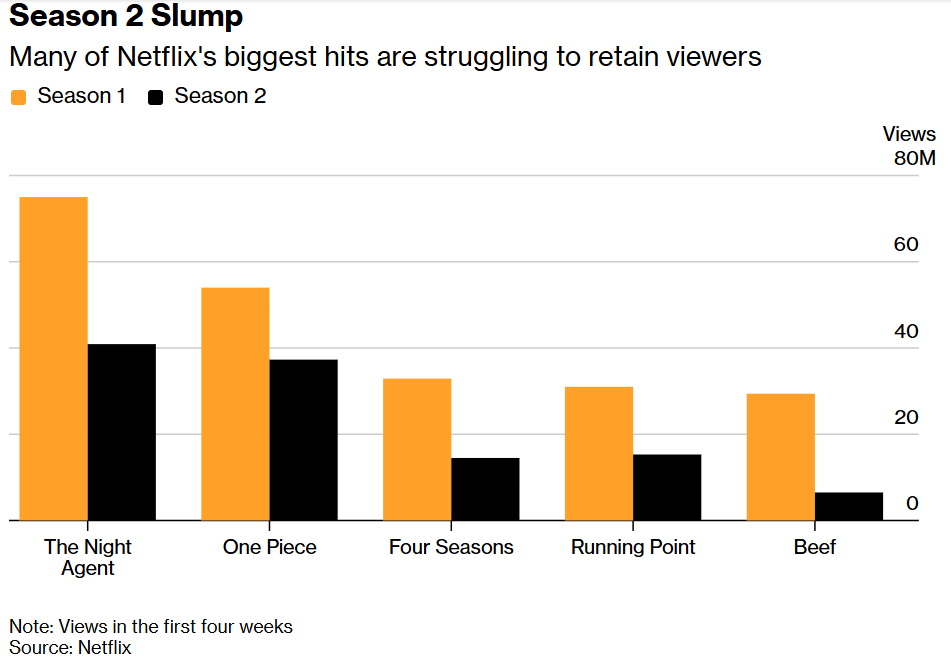
The other problem is that the second season is de facto gated behind the first one, so you’re going to see a big drop almost no matter what.
Lucas Shaw (Bloomberg): One Piece, one of Netflix’s most-watched shows of 2023, lost more than 30% of its audience for the second season. Season two of Beef suffered a drop of more than 70%. The Night Agent shed 50% of its audience for the second season and another 35% for its third season. These figures are all through the first four weeks of a show’s release and come straight from Netflix.
DarkStarTales: Too much of a gap between seasons. You wait 2 years, to see 6-8 episodes.
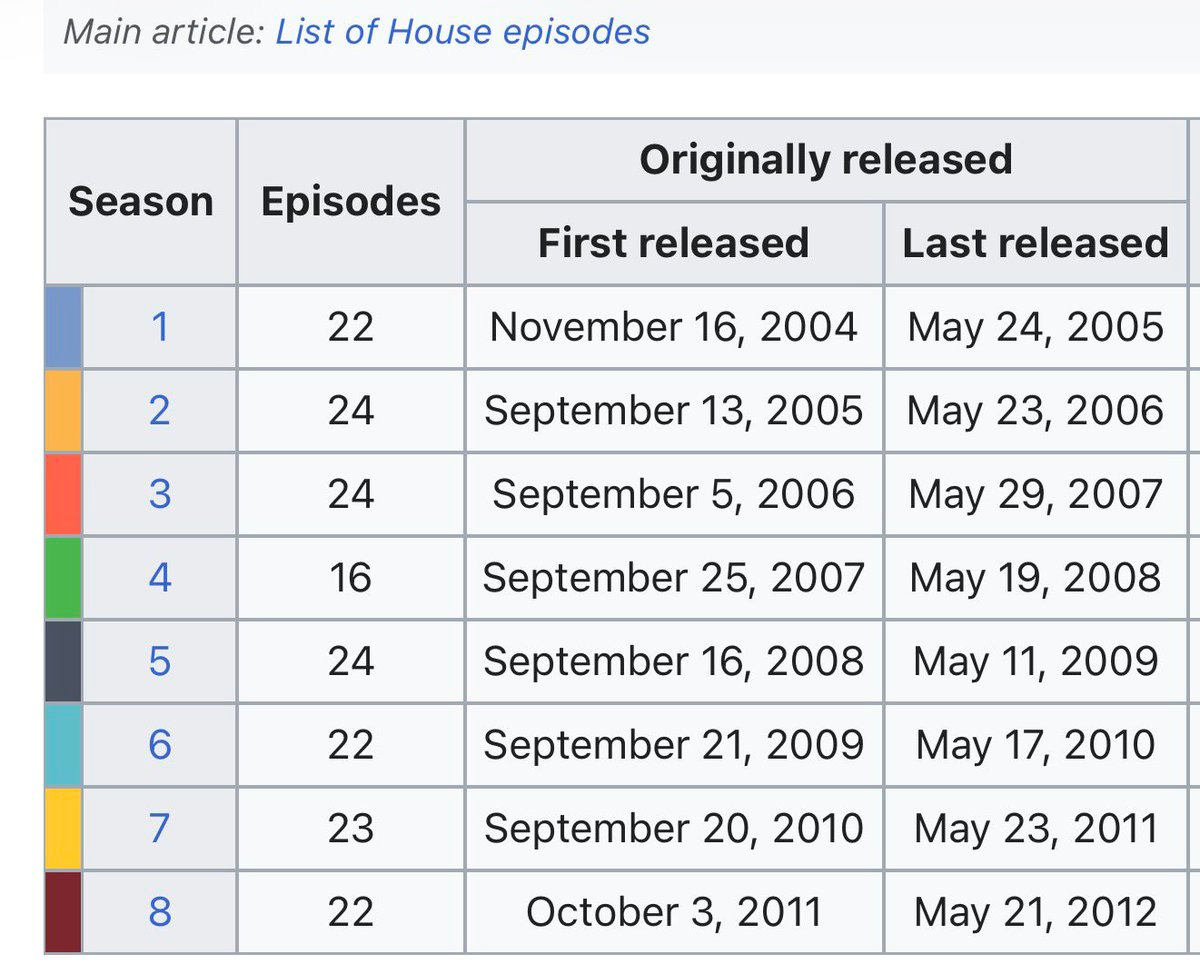
the ghost of groditi’s future: when House aired, you got 20-27 episodes of the big shows and the time between one season ending and the next one starting was like 15 weeks. now its like 8 episodes and then a 5 year wait. for teen/YA content audience has effectively aged out of it by the second or third season
We should very obviously allow, and also encourage, high status people to be weird in ways that bring them joy and other forms of utility, including in ways you would not want to be adopted by the broader culture, or that aren’t for most people including you, or that fail if not done with great care and a lot of work. Indeed, those who pull this off should if anything be raised in status.
There is an amount of scaling of behaviors at which you need to worry about the contagion effects of assigning too much status to behaviors most people should not be emulating, to the point of considering lowering the status of high-profile such folks. That level has to be very high before it becomes a dominating factor, but it is real.
Gamers Gonna Game Game Game Game Game
PlayStation will end selling of physical discs for new games in January 2028. There is a vocal minority that wants physical copies, often due to fear of content being taken away. While that does happen, the decay rate in value of games is severe and revocations are very rare. In practice this is fine.
Claim I saw: The new generations don’t really ‘game’ at all, not at scale. When they do ‘game’ usually they use things like Roblox that are endless multiplayer slop machines without off ramps, and now everyone wants a Roblox clone. The ‘game’ part is terrible but few seem to care.
Conrad Bastable (abridged):
TL;DR -- Millennials are the new boomers, Halo is Woodstock, WoW is the iPod, Dad gamers are the only “gamers” left by their own definition (& they don’t have time to play anymore), the kids are all cracked out on Live Service Slop platforms that they can’t escape and don’t want to, competition is dead, E-Sports is dead, creative content is dead, screaming down the mic is dead, couch co-op with your friends is dead, couch co-op with your Dad is dead, AAA games are dead, consoles are dead, Game Pass is dead.
… supporting industry stuff: - industry publications say average gamer is now ~37, up from 29 in 2004 - they also note that kids <12 have seen the largest drop in videogame engagement post-pandemic of all age ranges (-6%) - Pew’s 2008 report says “Fully 97% of teens ages 12-17 play computer, web, portable, or console games”, whereas their 2024 report says “the vast majority of U.S. teens (85%) say they play them. Just 15% say they never do” - Gen Z’s favorite games are Minecraft, CoD, GTA, Fortnite, and Roblox
…
- Newzoo has a 2026 report saying only ~13% of gametime went to new releases! - 2/3rds of gametime went to >6 year old games!
@deepfates: this is an awesome analysis of massive changes in the “gaming” industry. But I think it’s missing a key point in calling Roblox, Minecraft Fortnite, etc. “live service slop with games attached”
The reason everyone is in those places is because they are WORLDS. not games at all.
you can’t actually build anything or have any fun in the real world, especially if you’re a kid, but there’s infinite virtual space to transform and infinite games to play, in a programmable reality with ontological hardness that you and your friends can hang out in 24/7. Fuck Halo
Michael Davis-Wilson: I think this is what everyone hoped about these spaces, but based on my observations of The Youth, the bulk of their relationships to said spaces are accurately described as “live service slop”
@deepfates: yes, and 99% of everything is crap and 90% of everybody is lurkers. even if you don’t ever create anything. We’re hanging out in a world called Twitter. The point is that it’s a world you inhabit together and that’s real to all of you
I think most game time going to old games is great for players. Why not play games that have stood the test of time, are fully finished and expanded, and probably a lot cheaper? The best games will be evergreen. Alas, it is bad for the business model.
The good news is that the best local or singleplayer digital gaming experiences are still there, and mostly far easier to access than they used to be. You can return.
There is much more at the link.
There are those who speculate that the future is AI-generated customized games on demand. I think mostly this is not the case at least for a while. Playing a hand crafted game that matches a fixed experience is far more satisfying on many levels.
I think Deepfates point is well taken. There is a great need to create and build in interactive ways, so if we take that away in the real world, if we don’t even easily let kids physically visit each other, then they will need some sort of ‘virtual world’ substitute, no matter how slopified.
I Was Promised Flying Self-Driving Cars
You either die the anti-regulatory hero or grow the business enough to become the villain, many such cases.
Also, the blind are not the primary reason to want self-driving cars everywhere, but they are one very good reason, and if that’s what it takes then your offer is acceptable.
Timothy B. Lee: The likely next mayor of DC, Janeese Lewis George, asked some perceptive questions at this morning’s DC council hearing on autonomous vehicles.
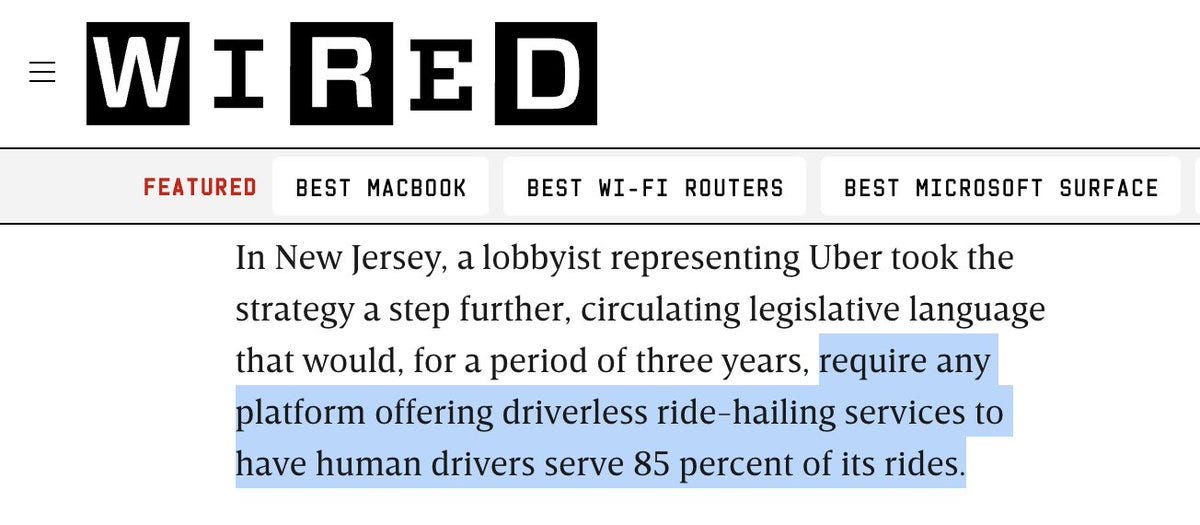
Uber seems to be in rent-seeking mode as they lobby the council to require AV companies to participate in “hybrid networks” (like, um, Uber) that offer both AVs and human-driven vehicles. So far @charlesallen doesn’t seem to be buying it.
Blind advocate Claire Stanley: “The first time I took an autonomous vehicle in Phoenix, I experienced freedom... I did not have to deal with drivers who would deny me because of my guide dog. I did not have to drive with a driver who made me uncomfortable.”
Stanley says federal law guarantees the right of blind passenger to travel with their guide dogs, but despite this that she has been denied service on multiple occasions due to her guide dog.
Ethan McKanna: Uber is doing everything they can to slow down autonomous vehicles. This is absolutely absurd and will cost lives
They want autonomous vehicle services to have human drivers serve 85 percent of rides???
Matt Bateman: The de Blasio Uber view—where Uber users in NYC got a tab that showed few cars, high prices, and massive wait times under a hypothetical de Blasio regulatory limit—was one of the best, proudest anti-regulatory campaigns of all time.
How the mighty have debased themselves.
roon (OpenAI): uncs remember what feels like just yesterday when uber was the anti regulatory hero, crusading across the metropoles of the world against rent collection of taxi services. I remember when uber was a real player in ai research too. life comes at you blindingly fast
Patrick Hedger: A huge shame to see a company that pioneered necessary disruptive competition turn to regulatory moats.
If I was Uber, I would not obviously be that keen to force Waymo temporarily into offering their services on Uber or Lyft. That is good for short term business, as you can seek rent, but that is direct marketing to your best customers. What happens in three years?
Nor do I think they would have much chance at making this permanent. Once people experience Waymo, they become advocates, and the ‘safety’ concerns quickly die out.
The ‘right’ answer is clearly around 4.5, except that football is weird and its points are scored more than one at a time. If you get to 114, you’ve gone too far.
Lord Hollyhock: pro sports ranked by points: cricket: 150 basketball: 114 rugby: 24.5 football: 22 tennis: 4.80 formula 1: 4.590 baseball: 4.5 hockey: 3 soccer: 1.5 chess: 0.50 golf: -1.5
America still sucks at futbol, it turns out. We handled the group stage but the moment we had a Worthy Opponent with real stakes we fell apart. Why do we suck? The obvious reason is that we send our best talent to football, basketball and baseball.
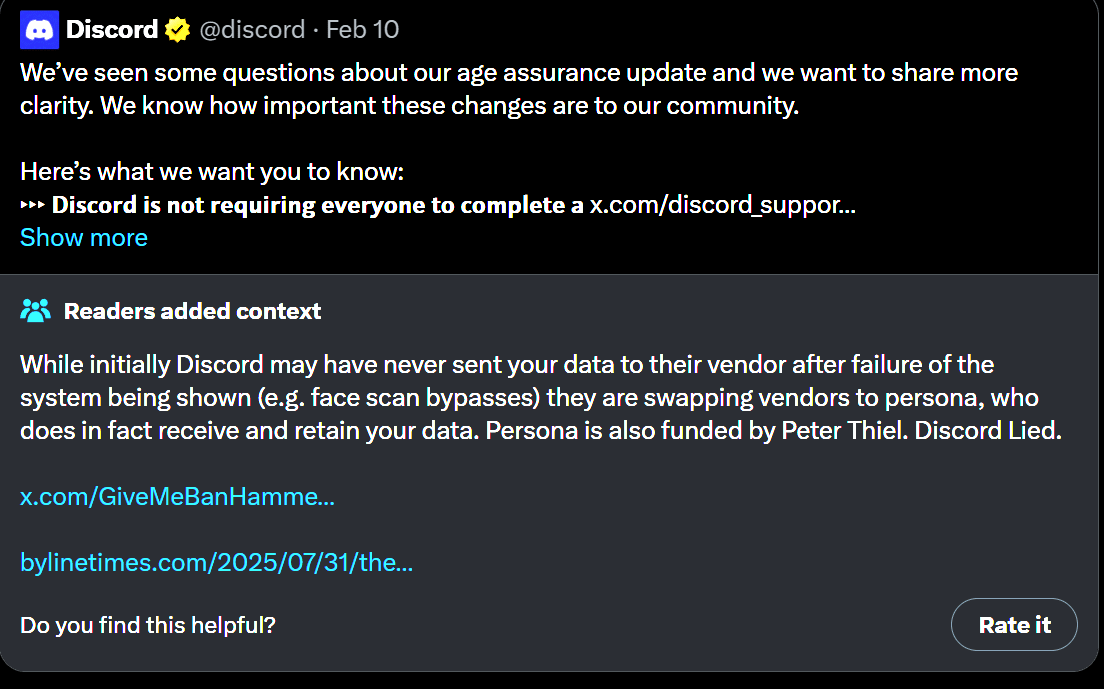
This was, let’s face it, deeply stupid, and if it held up it would go to very bad places. Adam Thierer here predicts a wave of lawsuits against players large and small. I instead predict and hope that juries are stupid, and this gets reversed on appeal, or that Congress steps in to fix this, although it would likely extract some stupid price like age restricting social media access along all the damage that comes with, or that some way to create a liability shield is found moving forward. Meta and Google have indeed both filed their appeals.
Perma Banned: “Facial scans never leave your device, and Discord and vendors never receive it.”
Meanwhile people discovered you are using Persona service.
A service that specifically requires a person’s face or ID scan to be sent to Persona’s databases.
Caught lying again, Discord?
Government Working
The UK is moving to ban children from using VPNs, as in you have to use ID to use a VPN, although for now this was voted down. This would be rather high on the ‘you were warned you are now living in a police state’ and ‘are we the baddies’ scales. It also presumably won’t fully work, since VPN providers are not especially interested in respecting such rules, but most people especially on a phone are not going to be that resourceful in getting around barriers, the same way that the Great Firewall of China is easy to overcome if you care a lot but hard enough to overcome that most people don’t do it.
The new EU policy of applying customs duties to tiny e-commerce parcels is remarkably close to a de facto ban on such small parcels. Some might say the system is working as designed.
Ursula von der Leyen: From today, customs duties apply to e-commerce parcels worth up to €150 entering the EU. 30 million Europeans work in retail; it’s our our largest private-sector employer. And the surge in low-value online imports has put our retailers at an unfair disadvantage.
Too many of these products also fail to meet EU safety standards, putting consumers at risk. Today’s change is about restoring fairness for European businesses and better protecting our consumers.
@levelsio: As someone who lives in Portugal which already stops every single package you get from outside EU with no exceptions for a decade or more:
I can tell you how this will go
From now on if you receive a package from outside EU, it’ll first go missing for weeks and nobody will know where it is, then you’ll receive an email from your country’s customs agency
They’ll make you login to some extremely unusable and outdated web portal which breaks half the time and where you have to classify your shipment in one of 10,000 confusing category codes
Depending on the category code you’ll pay a different tax rate, sometimes it’s 5% sometimes it’s 60%
Then you have to pay the customs duty in some archaic way that will also be broken half the time
And then you’ll finally receive your package from outside EU after months
Experiencing this for a few times you’ll realize you will never ever try to order or receive anything from outside EU ever because the ordeal is too painful and expensive
I get asked a lot here by people from US to test out new products (like the guy who made the Minimal Phone) and it’s just literally impossible for me to receive it even for testing. I tried to classify it as samples for testing but you need to go through a bureaucratic process of insane lengths to get that through so I just gave up
Realistically all this does is make Europeans live even more in the stone ages, as now they can’t use modern AI, nor get modern products from outside EU because it’ll be too much hassle to order
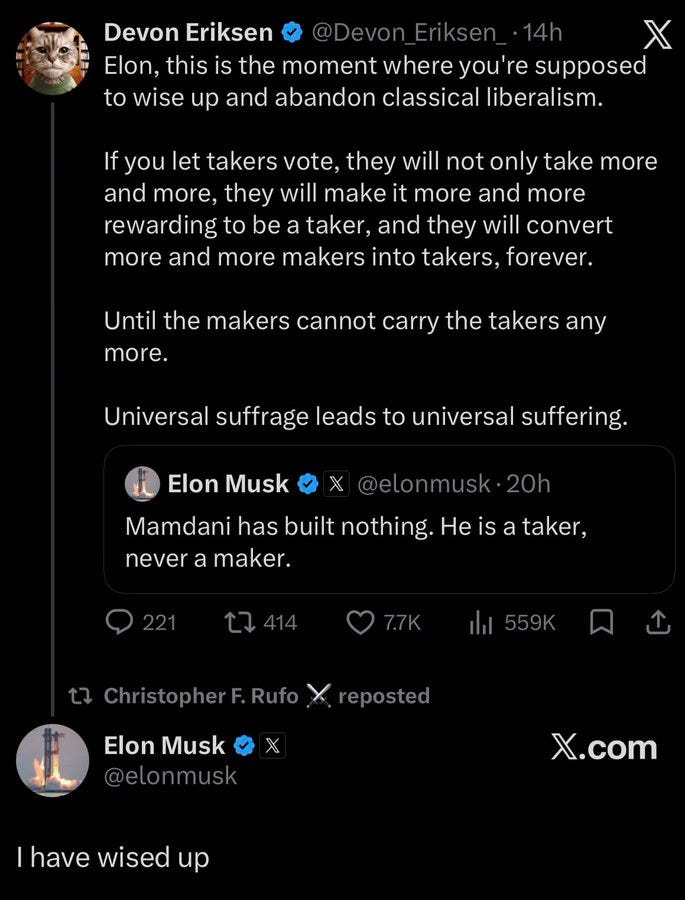
Derek Thompson: ~trillionaire celebrates America’s 250 by saying poor ppl shouldn’t vote~ sounds like a tawdry satire of plutocracy and yet
Someone is attempting to community note Derek Thompson, saying Elon Musk didn’t say poor people shouldn’t vote, which is technically true, he said by implication that takers shouldn’t be allowed to vote. Very different, of course.
Jones Act Watch
The Jones Act waiver worked to the extent things were waived, more stats are in.
Colin Grabow: Jones Act waiver update: ~31% more crude oil and petroleum products have been moved by water to the West Coast/Alaska/Hawaii from the Gulf and East Coasts in less than 100 days than what typically gets moved in a year (2020-25 annual average).
Speaker of the House can only get 52 GOP signatories for a Jones Act waiver revocation request. More than half of the 52 are in districts with at least one ‘Jones Act beneficiary company’ which is code for rent seeker.
The bottom line on the Jones Act continues to be that it is supposed to be a tradeoff of accepting higher costs to get shipbuilding capacity and maritime crews, but we’ve run the experiment and all it did was destroy all three.
Scott Lincicome: It really is amazing: the govt is openly considering using Korean shipyards to build NAVAL DESTROYERS, but it’s supposedly a NATIONAL SECURITY THREAT if the Jones Act were reformed so that US companies could buy/use Korean container ships for US-based trade.
Highly Effective Altruism
I am highly excited by this project, spending $500 million to solve respiratory infections, in particular via either broad-spectrum preventatives or air cleaning technologies.
These are clearly highly neglected areas with huge upside, where technological solutions seem highly feasible. Even in ‘normal mode’ we lose an average of weeks per year to such things, and every now and then there’s a pandemic, potentially in the future an AI-enabled engineered pandemic or worse.
I would not say this is my top use of $500 million, but it is vastly better than almost all uses of $500 million. Excellent show all around.
tautologer: this is obviously a biorisk defense project in a thin disguise. preventing the common cold and flu is nice; but the real goal is to prevent what comes next.
oh yeah they just say this outright in the blog post 😅
i wish i phrased this in a less conspiratorial way that’s not really what i meant. i don’t think it’s “disguised” per se i just think that people don’t want to scare the public/hyperstition by talking too much about biorisk
Yes and no. Preventing what is next might be far more important, but common colds and flus really are a big deal.
Sheel Mohnot: A+ philanthropy from Stripe, Anthropic, OpenAI, Gates, Jane Street.
$500M toward making everyone less sick.
We treat illnesses like they are inevitable, but they’re not. Colds, flu, RSV, COVID, etc. cost the world hundreds of billions and make ppl miserable.
Let’s end them!
Nan Ransohoff: Today we’re launching Intercept: a $500M philanthropic initiative to make respiratory infections, like the common cold and flu, a thing of the past.
We treat respiratory infections as a minor nuisance, but that’s really not the case. Most of us will spend 5% of our lives (!) sick from these viruses, they kill 1M people a year, cost $600B annually in productivity, and periodically threaten civilization through pandemics.
So, if they’re such a big problem, why haven’t we dealt with them yet? Last year we convened ~40 leading scientists, pharma R&D leaders, biotech investors, and regulatory experts to better understand that.
We heard two main reasons: (1) First, it’s just technically very challenging: respiratory viruses represent hundreds of distinct, mutating strains across several families. Fortunately, recent breakthroughs make this newly possible. (2) Second is a lack of funding: broad-spectrum solutions have historically been underfunded, in part because they’re not a great fit for most philanthropic or commercial funding (and while COVID generated a burst of activity around preventing and understanding respiratory infections through an influx of new funding, that hasn’t been sustained).
We think that with enough focus and funding, this might be solvable. Intercept is a $500 million philanthropic initiative that will take advantage of new tools to catalyze the development and deployment of two types of products: broad-spectrum preventatives and air cleaning technologies.
This problem is undoubtedly difficult. But it’s more tractable now than it’s ever been. We think we should give it our best shot.
We’re enormously grateful to our anchor funders: @stripe , @AnthropicAI , @TheFluLab , @FoundationOAI and individuals from Jane Street.
And, I’m very excited to be building this with @incredutility and the rest of the team.
Sholto Douglas (Anthropic): I (and a bunch of my colleagues) donated to this. I think it is a really excellent initiative. TLDR: - Equity investments in broad spectrum preventatives that are ready to get to phase 2 within 4 years - Grants for basic research that isn’t yet ready for commercial viability - Prove out air cleaning tech (like far-uvc), and make it extremely obvious whether it should be adopted in schools, workplaces etc.
Why we found this a good project to back: It is an incredibly noble goal (end respiratory disease) - with extremely diffuse benefits that are hard to capture (so tricky for existing captial markets), with specific uses of money (fund/prove out xyz tech categories). In the best case - it becomes self sustaining because the equity investments are right, but it doesn’t need to be if that’ll be the most effective use of the capital for the goal.
Jakeup: you should set up a donation option that charges me $100 every time I catch a cold so I’m reminded how often it is (two kids in preschool) and feel that I’m fighting back
Variously Effective Altruism
The race is on to figure out ways to quickly and wisely deploy donations from Anthropic and OpenAI employees, who are collectively going to be giving out at least tens of billions. A lot of that money is going to be deployed according to Effective Altruist (EA) principles, for a variety of traditional and non-traditional cause areas.
The linked story centers on Lighthaven, which has become the gathering point for many who seek to make this new source of money go well, including many of those who will soon be sources of that money.
My worry is that by default a lot of that money is routed and captured by the semi-formal EA ecosystem, mostly in ways that are not so relevant to my interests, and thus in my view to varying degrees effectively wasted and also rather distortionary. With little time to think about what to do with the money, the default is looking for donor advisors like those written about in the article. And that a lot of the rest will get blindly shoved out the door into far worse institutional structures.
The worst case is that a lot of it is not only wasted but is effectively eaten by predators, similar to how things work in the existing broad philanthropic ecosystem.
Andrew Fedorov: EAs remember the grifters who superficially adopted their frameworks when the FTX money started flowing. They want to avoid that this time.
FTX was operating in a mode one might call griftmaxxing. Everything about them screamed ‘come over here and grift.’ So that was a worst case scenario. But the default case is pretty bad as well. I think it was largely good that we didn’t try to optimize for this event too hard or too far in advance.
But yes, this level of money is inevitably blood in the water, and there is nothing that is going to fully stop this train.
Andrew Fedorov: “You really don’t want to say to a bunch of people, ‘Hey, there’s going to be a bunch of money in this space very soon,’” said Keller Scholl, a longtime effective altruist and contractor with effective-altruist organizations. “The longer you can put that off, the safer you are from some of those corrosive effects.”
But their efforts haven’t been entirely successful. “I can definitely see a certain schmooziness showing up again, where it’s like, ‘Oh yes, I think very seriously about AI,’” said former effective altruism D.C. head Andy Masley. “I know that that’s a signal for, ‘Fund me.’”
I am working a few angles to try and improve the situation as best I can, to help ensure that people make good decisions according to their own priorities, world model and values, and yes I stand ready to help the new donors figure things out if they ask.
In the past I’ve participated in what are now four rounds of the Survival and Flourishing Fund, and I hope that related mechanisms can help, as well as hoping that I can apply what I learned directly during that process.
Build a better game. It’s a rough assignment. This level of money flooding in breaks basically every existing related group and institution’s ability to process the necessary information and manage the incentives.
I worry the most about the risks to the high-trust epistemic and social environments that I and others can currently rely upon in such places.
Oliver Habryka: Inasmuch as there’s a scene here at Lighthaven, that scene will be very drastically disrupted. It will be like a major force of nature that will suddenly change a lot of the vibes … attracting an infinitely large pool of grifters. People trying to come to terms with that — somehow — I’m pretty in favor.
I’m less excited by the people who are just going through the motions of how can I position myself in front of the infinite money spigot, which is a kind of thinking that, I think, will ultimately be responsible for a lot of the damage.
… The default thing for billionaires to do is to dip their toe into trying to give away their money. After a while, you become cynical and are like, ‘Fuck this. I don’t know how to have relationships, because everyone is clearly trying to hang around with me to see whether that results in them getting $10 million.
I very much want to avoid a version of this happening to me, which is one reason I am determined to keep my primary focus on the blog and avoid this kind of ‘direct’ optimization. I would love a $10+ million personal check and have ideas on how to use one, but am determined not to spend (almost) any optimization pressure seeking one.
These dangers are especially severe in the space of mitigating AI existential risk, where it is very easy for money to go to things that waste time without helping, or even become actively counterproductive. That is indeed my primary cause area, and that of many at Anthropic. The whole Anthropic shtick is recognizing that AI is going to get super powerful and might kill everyone.
Andrew Fedorov: Ironically, the thing that many effective altruists want to do with their AI wealth to do the most good is fund organizations working to make sure AI is developed responsibly.
If anything, it is remarkable that so much Anthropic money might flow to anything else. Even if you care about (for example) animal welfare, if you work at Anthropic you should understand that the way to improve animal welfare is to first make AI go well, as if it doesn’t things turn out badly for the animals too, and if it goes well then making things go well for animals should be easy.
That doesn’t mean entirely give up on funding good things in other spaces, but such considerations seem secondary.
Depending on your point of view, you might see MacKenzie Scott as having done a lot of good, or having tried and failed to do a lot of good, or as having done great harm, or as trying and failing to have done a lot of harm.
What you think depends on how you think about the typical cause areas she funds, how effective you believe she has been in either encouraging the growth of such fields, making them more parasitic or making them more effective, and what you think this does to the world at large.
What you definitely cannot do is say ‘well she did not directly save that many lives.’ That is true, but missing the point. She wasn’t trying to do that. You can’t ignore the actual impacts she had, whether or not you like them.
If your methodology says MacKenzie Scott can be summarized as ‘inefficient’ on this basis, then your system of evaluation does not work and you need a new one.
I do agree that if your goal is purely to spend money to advance short term global health and QALYs, GiveWell has a reasonable case, and MacKenzie Scott does not.
Max Ghenis (incorporating his later correction into OP): I built an interactive model from her own gift database: ~70,000 QALYs weighting each study by causal credibility, ~200,000 taking every effect at face value.
Her blended portfolio: $148k per QALY. @GiveWell ‘s program averages ($4,000–5,500 per life saved) convert to ~$200 per discounted QALY. Handicapped like-for-like, the frontier still buys ~500× more health per marginal dollar — a few hundred× at portfolio scale. Most of the health comes from the ~5% delivered abroad.
Nathan: Comparing MacKenzie Scott’s giving to if the money had gone to @GiveWell . Her donations bought about 1500x less improvement per $ than the marginal GiveWell $
Oliver Habryka: I am confused, it seems very unlikely from my perspective for her donations to not have caused enormous amount of net harm. How does this calculation arrive at a positive number at all?
Richard Ngo: +1 except I’m not claiming to be confused.
Trying to sum up such wildly disparate impacts into a single number is so misguided that we should interpret it primarily as a move in the game “pretend we’re all trying to help people, but actually support existing power structures”.
Here [Nathan] and [Max] are doing politics on GiveWell’s behalf not truth-seeking.
Gustaf: “the model puts no probability on zero or harmful effects” and “This model is deliberately scoped to health.”
Oliver Habryka: Sad. I think cost-effectiveness analysis without the left tail is pretty harmful to the epistemic commons. It’s usually more important in the context of trying to show positive effects. It’s easy to arrive at large positive effects by just ramping up the variance and cutting off the left tail.
Nathan: I guess as a point of norms, I generally like some numbers more than none. Like I am not quite sure what norms should be here.
Celene is in Seattle!: I’m unfamiliar with her donations; why have they caused net harm?
Oliver Habryka: She spent a huge amount of money on pretty crazy and radicalized advocacy groups. A few things I remembered was a bunch of pretty radical tenant-rights stuff, a bunch of labor rights advocacy, a huge pile of pretty radicalized social justice advocacy, etc.
… I list examples in the other tweets! Go to all the people who are claiming random positive effects and demand the same burden of proof and then come back.
They want to call this ‘illegal’ and ‘market manipulation’ instead of ‘lol you bet on a prediction market for George Santos based on his public statements.
I mean, yes, he lied and manipulated the market and also if you were on the other side of these bets then there is a saying about a fool and his money being soon parted, and another about it being a sin to let a sucker keep his money.
The Lighter Side
Self driving… toilets, for people with limited mobility? Imagine how much we can save by not letting our toilets sit idle, with no on sitting on them.
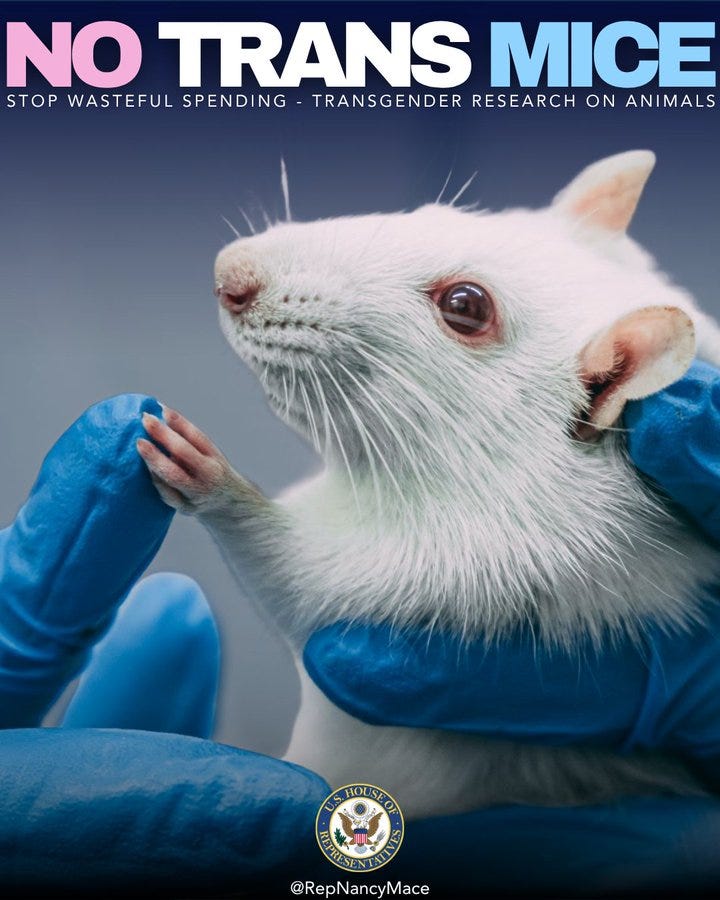
Alex: As someone who works with transgenic mouse models for cancer research, this is objectively one of the funniest things I’ve seen a real life politician post.
Rep. Nancy Mace: Animals should not be used for radical transgender experiments.
This is not science. This is ideological cruelty paid for by the American taxpayers.
Our TRANS MICE Act ends it. No federal funds may be used to conduct, support, or fund research aimed at altering an animal’s biological sex.
No hormones. No surgeries. No taxpayer dollars spent mutilating animals in the name of transgender ideology.
This legislation brings accountability, ends taxpayer-funded cruelty, and ensures science serves the public, not ideology.
The best part is she doubles down.
Rep. Nancy Mace: This post is not about transgenic mice. It is about federally funded transgender-related experiments on animals.
The bill is called the Transgender Research on Animals Now Stops and Money for Ideological Cruelty Eliminated Act, also known as the TRANS MICE Act.
The Community Note addresses “transgenic mice,” which is a completely different topic. More info on our bill here.
People these days need practical knowledge more than ever.
Misha: A lot of people absolutely hate moving because they don’t know they can hire a bunch of strong guys for a reasonable price
This is known as the hunk cost fallacy
Misha: A lot of people think they can’t afford to raise kids because they think every child needs their own bedroom.
Normally I enjoy lamenting the downfall of video games, but it's hard for me to feel sad about it recently because Slay The Spire 2 has been so much fun.
Especially underrated is the multiplayer mode. If we're living in a world where social relationships are being intermediated by screens, maybe we should accept it and just find really high-quality ways to have our social relationships intermediated by screens. Baldur's Gate 3 multiplayer was also a great experience.
I have a dream. It is automated chart review/data mining for retrospective cardiology studies.
Every physician at an academic medical center has had the unfortunate experience of having to chart review for retrospective studies. This is very labor intensive and a poor use of time for physician-researchers (“I accumulated a mountain of student debt just to do data entry?”) Usually it is outsourced to a medical student or resident who is willing to do scutwork to apply for fellowship or a career in academic medicine. You’re given a list of medical records and have to individually and manually click into each chart and fill out the forms into Redcap (like Google forms but with PHI-protection). It can take an hour or more per patient (in my personal experience). For example, a single variable you’re looking for could be on page 273 of a a 500-page PDF from an outside medical record uploaded to Epic.
If you could link Claude and Epic (the most common electronic medical record), you could do all this work at 10000x the speed. Unfortunately there has been a lack of progress on integrating LLM’s into the medical field in general, with the barriers primarily around dealing with PHI and not wanting to hand tech companies patient data. Reasonable concerns, to be clear! But there are huge impacts if you could integrate.
High impact projects I can think of off the top of my head, that I haven’t had the bandwidth to pursue due to the lack of data entry capability:
Magnesium supplementation and arrhythmia risk in congenital heart patients. There’s a HUGE amount of rhythm monitor data, you just need before and after arrhythmia burden after Mag initiation.
CardioMems (portable pulmonary artery pressure monitor) response to change in diuretic titration and cross compare what uptitration algorithms work best. (HF hospitalizations is one of the biggest medical expenditures so if you can reduce this by even 1% through better early warning and intervention that’s very big).
Fetal heart rate monitoring - take the HR and acceleration/decel strips (often 1-2 days worth for each patient) and cross compare them to C-section vs vaginal delivery rates and fetal outcomes.
All this will probably come one day. Advantages would also be that you reduce intra-recorder variability (ie one researcher interpreting and coding data differently than another, ever a pitfall). But in the meantime I feel like I’m in a field moving glacially while the rest of the world zips by.
If anyone is working on this or has thoughts I would love to hear more! Or be corrected!




Normally I enjoy lamenting the downfall of video games, but it's hard for me to feel sad about it recently because Slay The Spire 2 has been so much fun.
Especially underrated is the multiplayer mode. If we're living in a world where social relationships are being intermediated by screens, maybe we should accept it and just find really high-quality ways to have our social relationships intermediated by screens. Baldur's Gate 3 multiplayer was also a great experience.
I have a dream. It is automated chart review/data mining for retrospective cardiology studies.
Every physician at an academic medical center has had the unfortunate experience of having to chart review for retrospective studies. This is very labor intensive and a poor use of time for physician-researchers (“I accumulated a mountain of student debt just to do data entry?”) Usually it is outsourced to a medical student or resident who is willing to do scutwork to apply for fellowship or a career in academic medicine. You’re given a list of medical records and have to individually and manually click into each chart and fill out the forms into Redcap (like Google forms but with PHI-protection). It can take an hour or more per patient (in my personal experience). For example, a single variable you’re looking for could be on page 273 of a a 500-page PDF from an outside medical record uploaded to Epic.
If you could link Claude and Epic (the most common electronic medical record), you could do all this work at 10000x the speed. Unfortunately there has been a lack of progress on integrating LLM’s into the medical field in general, with the barriers primarily around dealing with PHI and not wanting to hand tech companies patient data. Reasonable concerns, to be clear! But there are huge impacts if you could integrate.
High impact projects I can think of off the top of my head, that I haven’t had the bandwidth to pursue due to the lack of data entry capability:
Magnesium supplementation and arrhythmia risk in congenital heart patients. There’s a HUGE amount of rhythm monitor data, you just need before and after arrhythmia burden after Mag initiation.
CardioMems (portable pulmonary artery pressure monitor) response to change in diuretic titration and cross compare what uptitration algorithms work best. (HF hospitalizations is one of the biggest medical expenditures so if you can reduce this by even 1% through better early warning and intervention that’s very big).
Fetal heart rate monitoring - take the HR and acceleration/decel strips (often 1-2 days worth for each patient) and cross compare them to C-section vs vaginal delivery rates and fetal outcomes.
All this will probably come one day. Advantages would also be that you reduce intra-recorder variability (ie one researcher interpreting and coding data differently than another, ever a pitfall). But in the meantime I feel like I’m in a field moving glacially while the rest of the world zips by.
If anyone is working on this or has thoughts I would love to hear more! Or be corrected!