

Covid 12/16: On Your Marks

The main action continues to be at the Omicron post. There’s still some background developments and near term developments worth noticing, but for now nothing that seems as important or that seems terribly urgent, so read that first.
Executive Summary
We might not do much about it until far too late.
And that’s probably better than the alternative.
Also some other stuff, like Will Eden’s excellent tweetstorm below.
Let's run the numbers.
The Numbers
Predictions
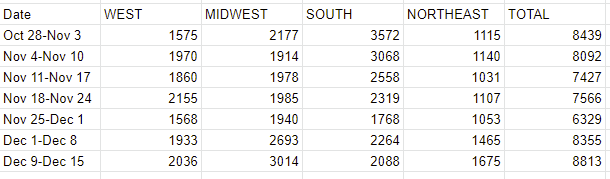
Prediction from last week: 750k cases (+2%) and 8,800 deaths (+5%).
Results: 747k cases (+2%) and 8,813 deaths (+5%).
Prediction for next week: 862k cases (+15%) and 9,050 deaths (+3%).
Those were some pretty good predictions. Don’t count on it happening again any time soon. Stuff’s about to get weird.
The case growth depends on how far along we are in Omicron taking over, and when those tests results will come in and how many people will get tested if the cases are mild. If we take the 2.9% for the period ending 12/11 seriously, we now are moving ahead 12 days, I’ll guess the true general doubling time is 3 days, so for the sample we’ll get it’s going to be something like 18% (+12% from previous levels) Omicron, and cases of Delta likely remain roughly level, with more upside than downside for the count. It’s already at or last that level in the specific places we’re measuring, but it makes sense that they’d be ‘ahead’ of other areas with much larger populations. And we’ll likely see some mitigation. So I’ll go with +15%, but the error bars are wildly higher than before. So many variables.
Deaths
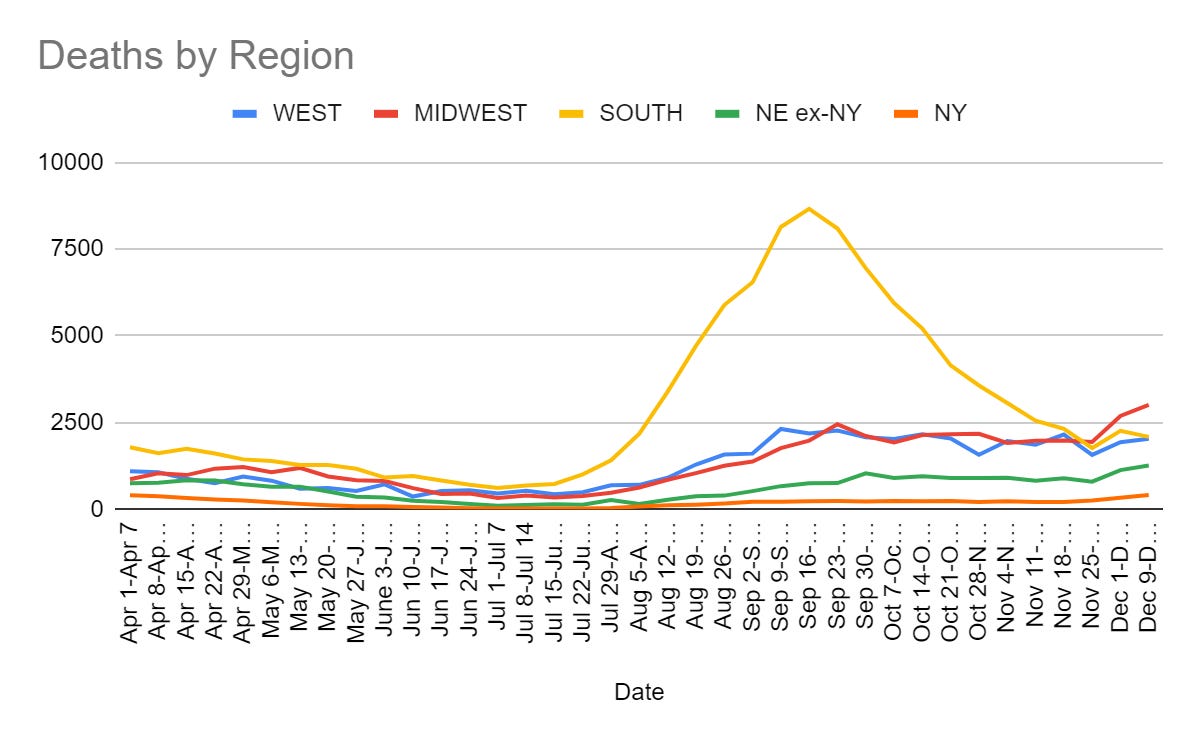
Deaths are straightforward, no reason to expect major change. Paxlovid remains illegal, Omicron isn’t here yet for long enough.
Cases
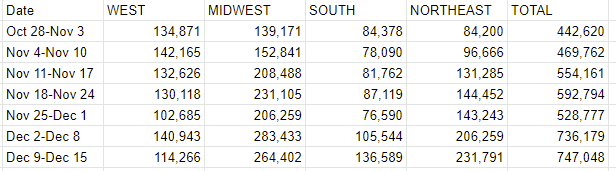
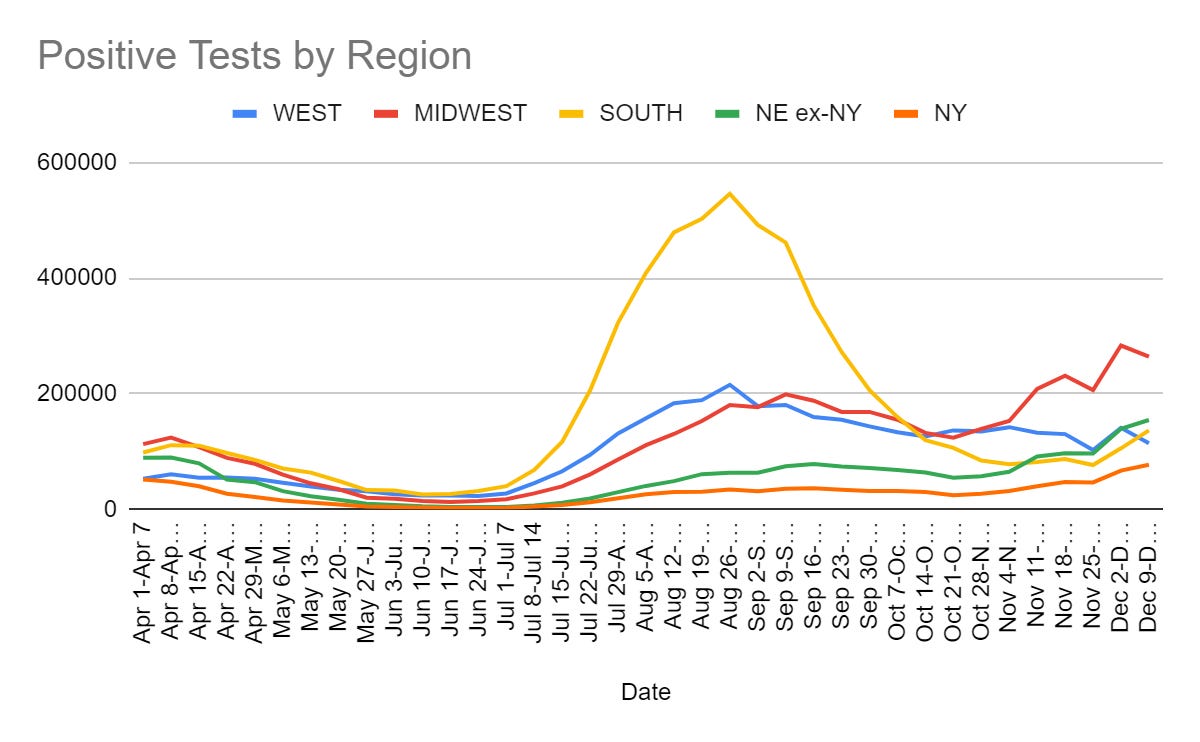
This is the question. We saw some regional movement last week, it’s probably largely random reporting fluctuations, except that the rise in the Northeast is very real. Going forward it’s all about Omicron. It’s super hard to time it, and what comes up on tests is several days behind what’s actually happening (e.g. a full doubling time) but my guess is that we’re already above 10% and increasing fast. London is our future, it’s merely unevenly distributed for a limited time.
So, how about Paxlovid? Can we hurry?
Paxlovid Remains Illegal
The final numbers are in, and they look good. Efficacy holding steady at 88%, no deaths in the treatment group, actively fewer ‘side effects’ in the treatment group compared to controls (presumably because controls had Covid-19, which causes a lot of ‘side effects’).
So now we have four questions:
When will Paxlovid become legal?
How much Paxlovid will be available?
While supply is limited, who gets that supply?
When supply isn’t limited, how do we get it to people in time?
The answer to when is around the end of the year. As of writing this the prediction market now again has it as a favorite at 55%, I hope some of you are making yourselves some money. There isn’t that much uncertainty here at this point, as I understand it, and we’ll almost certainly have Paxlovid by mid-January.
That brings us to question two. There are going to be enough doses this year for 200,000 patients. That’s two days worth of known cases right now, one day by year’s end, so indeed going forward production (as crippled by worries about approval) will be the central limiting factor. Pfizer will have 80 million treatments available next year, of which the US Government has bought 10 million. We don’t have information on the rate at which this can ramp up, which will be important because the bulk of the cases in 2022 are probably going to be in the first two months, and that’s also when we need to use Paxlovid to reduce pressure on hospitals.
Weekend Editor expects a narrow authorization:
Still, I’m betting on a narrower FDA Emergency Use Authorization. The risk of ritonavir interacting with other drugs is high (though known, so physicians have to check before prescribing), and the more widely an antiviral (or, for that matter, antibacterial) is used the more likely resistance mutations happen. So probably it’s going into the highest-risk populations first.
I have a very hard time believing that we’re going to deny Paxlovid to people who have tested positive because we’re worried about it causing resistance, even if that was wise. I also have a hard time believing we’re going to have abundant supply and hold it back from some population for ‘risk’ reasons, in the sense that this is so obviously insane even after all this we aren’t actually that insane right? Right? Oh no, at least half the time I type those words the answer is not what I’d like?
What I do expect is for this to be used as a de facto rationing method, with at least one period where there’s a surplus of supply that is sitting unused for a while, which brings us to the next question.
Given supply will be limited at crunch time, who gets that limited supply?
Presumably we should reserve doses for the elderly, whether or not it’s worth adjusting for conditions that constitute additional risk factors, because Paxlovid is even more effective in those cases and those cases have much higher baseline risk. There will be fights over geographic distribution, no doubt, but after that this part’s easy.
Then there’s the big problem. There’s two 70-year-old women, each positive for Covid-19. There’s only one difference between them, which is that one is vaccinated and the other is not vaccinated. You have one set of doses. Who gets it?
The argument for treating the unvaccinated patient is obvious. She’s at much higher risk. Can you imagine doing otherwise?
Yes, because the argument for treating the vaccinated patient is also obvious. Who is going to get vaccinated if it means you won’t get treatment? What would reaction be like if we were rewarding the unvaccinated with life saving medicine over the vaccinated? When that medicine was about as effective as vaccination? Can you imagine?
In other contexts, this choice has already been made in favor of the vaccinated, but this makes it that much more stark. My preference would be to announce the policy now, especially if it’s going to be vaccinated first. If you’re going to go for motivation and good incentives over the in-the-moment saving of lives, make it count.
Vaccine Effectiveness
Previous infection also works, and quite well, and all that, says study.
For vaccine effectiveness against Omicron, see the Omicron posts.
Vaccine Mandates
What counts as ‘fully vaccinated?’ That’s changing in many places, with a lot of Europeans being reclassified as effectively unvaccinated until they get their boosters, which in many places severely limits the ability to live a normal life. Then it’s going to periodically happen again.
It’s important to be ‘fully vaccinated’ or you’ll lose access to important services.

Private groups can get in on the act. The Metropolitan Opera here in New York is requiring boosters.
Another problem is that even if you’re convinced that you want a booster, our logistical systems aren’t up to the task. Everyone from the elderly to children is having trouble getting vaccine appointments, despite plenty of supply. If we want to get back to levels we had early in the year, we’ll have to actually be professionals and talk logistics.
The flip side of this is that if you don’t understand why NHS (healthcare) workers need to be vaccinated, you’re not going to make it.
It’s one thing to think there’s two sides to this, but how tone deaf do you have to be to call it ‘totally wrong’?
NPIs Including Mask and Testing Mandates
Colorado Governor Jared Polis lifts mask mandate, promises not to institute a new one for Omicron, someone should open a prediction market on whether he’ll be eating his words by March. Which he might well have to do, but in the meantime you have to love the explanation.
Colorado Gov. Jared Polis, a Democrat, declared in a new interview that the COVID-19 emergency is “over” and that he won’t be implementing another statewide mask mandate in response to the spread of the Omicron variant, explaining that if people aren’t vaccinated at this point, it’s their “own darn fault” if they get sick.
“Everybody had more than enough opportunity to get vaccinated,” Polis told Colorado Public Radio on Friday. “Hopefully it’s been at your pharmacy, your grocery store, a bus near you, [or at] big events. At this point, if you haven’t been vaccinated, it’s really your own darn fault.”
“Those who get sick, it’s almost entirely their own darn fault,” he continued. “I don’t want to say that nobody [will get the virus if they’re] vaccinated, but it’s very rare. Just to put it in perspective, of the about 1,400 people hospitalized, less than 200 (or 16 percent) are vaccinated. And many of them are older or have other conditions. Eighty-four percent of the people in our hospitals are unvaccinated, and they absolutely had every chance to get vaccinated.”
I strongly agree with the sentiment that this is an excellent compromise. Instead of imposing stupid restrictions as a Sacrifice to the Gods and blaming it on those who we claim did us wrong, we tell those people they’re being morons and that what happens to them is their own darn fault. It’s a deal.
There is a catch. If Omicron wasn’t about to hit us I’d be fully on board with this, but given it’s hitting about (check notes) right now I am deeply curious how far ahead he has thought this through.
Meanwhile, Governor Hochul in New York has instituted her new indoor mask mandate. Saratoga County has declared they will not enforce the order. Neither will Nassau.
Reactions were mixed, here’s the first reply and its first reply in turn:


Ah, choices and markets at work.
Or an alternative interpretation from Alex Tabarrok.
If you want a test in New York you do not want to go to CityMD. There’s another two screens worth of this line, and it matches my experiences, and these resources are needed for other medical issues. Instead go to one of the places at this link, or one of the in-street tents. I got a test last week, it was free, I didn’t even have to give insurance, I was done in five minutes and got it back the next day.
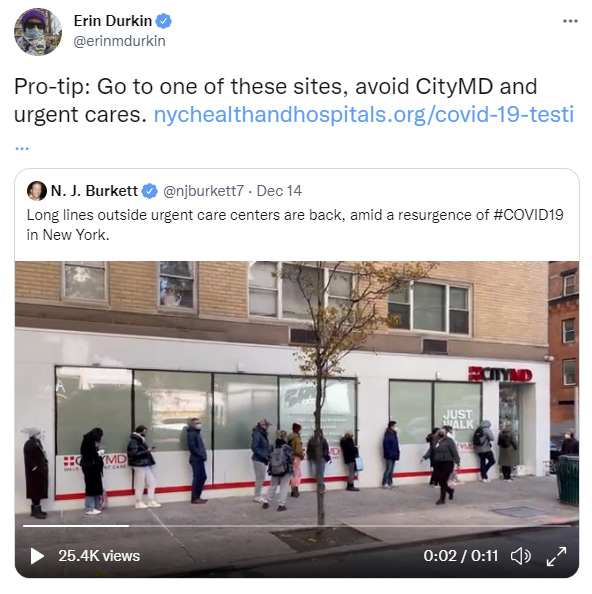
If you get to urgent care before they open, you have a shot of getting urgent care in a timely manner. If you otherwise need urgent care, you won’t be getting it all that urgently.
I’m guessing this is similar in many other places, but I don’t know for sure.
So why don’t we have all those free at-home tests? Tell it to me straight, doc.
And there’s this, I mean I have a suggestion or two I could make but what else is there to say:
Just 13 companies are authorized to sell over-the-counter tests in the U.S., though many more are still waiting to get green-lighted by the FDA. Even amid fears of a Covid-19 resurgence, Biden officials fretted that intervening now would stifle competition and discourage newer test makers from scaling up their manufacturing.
“It would’ve capped the market and not done anything to drive prices down,” a senior administration official said.
Instead, the official added, the administration is betting that staying out of the way “gets more players into the market, which gets more tests in the market, which drives down the cost.”
They also note how many tests are available.
The current supply of over-the-counter tests is also a practical barrier. The number of at-home tests being manufactured per month is expected to reach 200 million this month, 240 million in January and 300 million in February.
I have a feeling that if the government started buying tests at good prices, and/or didn’t make many potential Covid-19 tests illegal (including many that are used a lot in Europe) that we would see expanded supply.
It’s also worth noting that a lot of the tests we do have are being used on very low-value things, like testing four year olds once a week. If we don’t have enough for people who have reason to think they might have Covid-19, we should think about to what extent such policies are making things actively worse.
NFL Players Association calls for a return to daily testing. They’ve been advocating for this all season, and are reiterating this call. They’re right, this is a high value place to use our tests, and we should use them here. Kudos to them. No football, no peace.

This is a very non-representative sample, of course, but another data point:
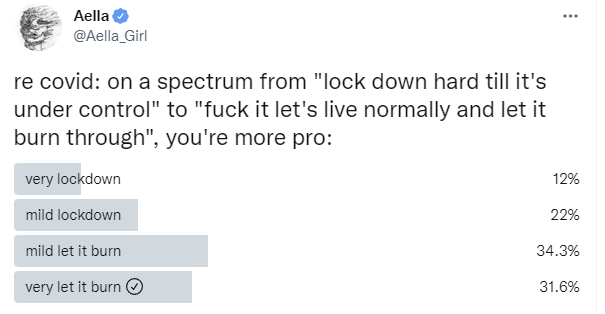
Before, support rose and fell largely based on how bad things were. But even before Omicron, things were starting to get worse. Yet support for countermeasures was falling. There’s a general sense of having had enough, even more so than before. The question is, will that matter when the logic of exponential growth starts hitting like a truck?
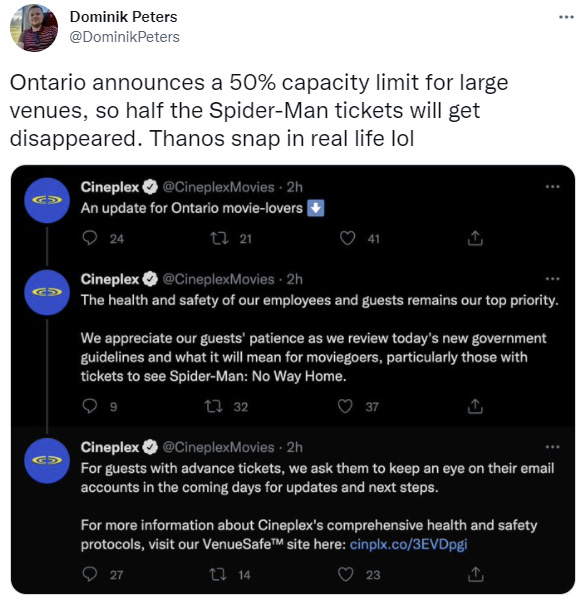
On the lighter side, from Ontario, the very definition of a half-measure.
Think of the Children
In Other News
Words of wisdom from my old friend William Eden on how we’ve navigated the pandemic, and the choices facing us going forward. Here’s Eric Weinstein’s endorsement, and then the since I would tell you to read the whole thing, sure why not, here’s the whole thing.

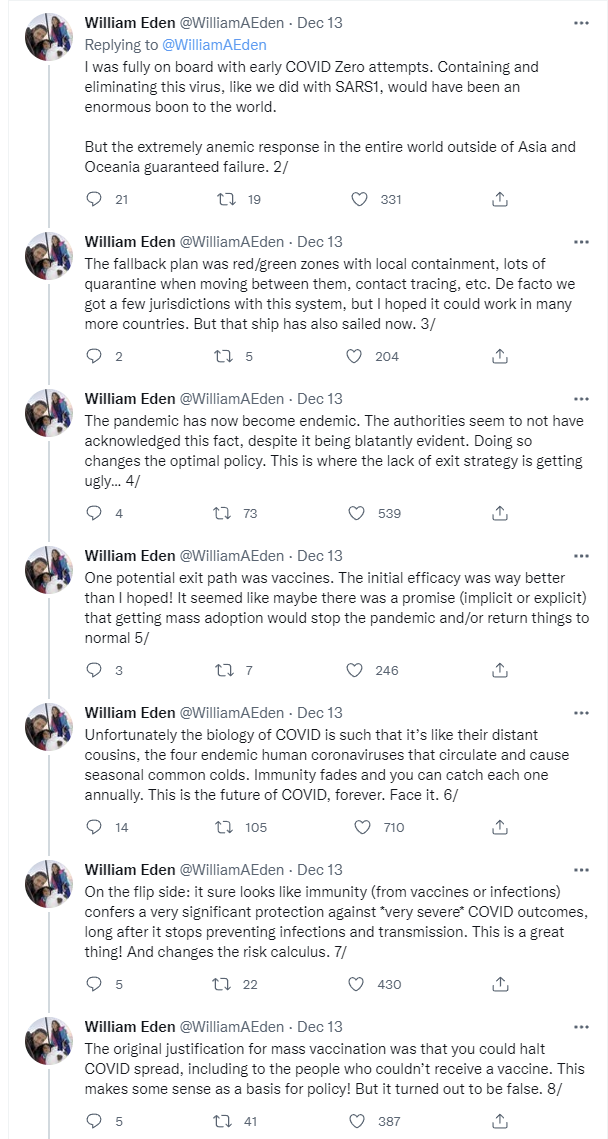
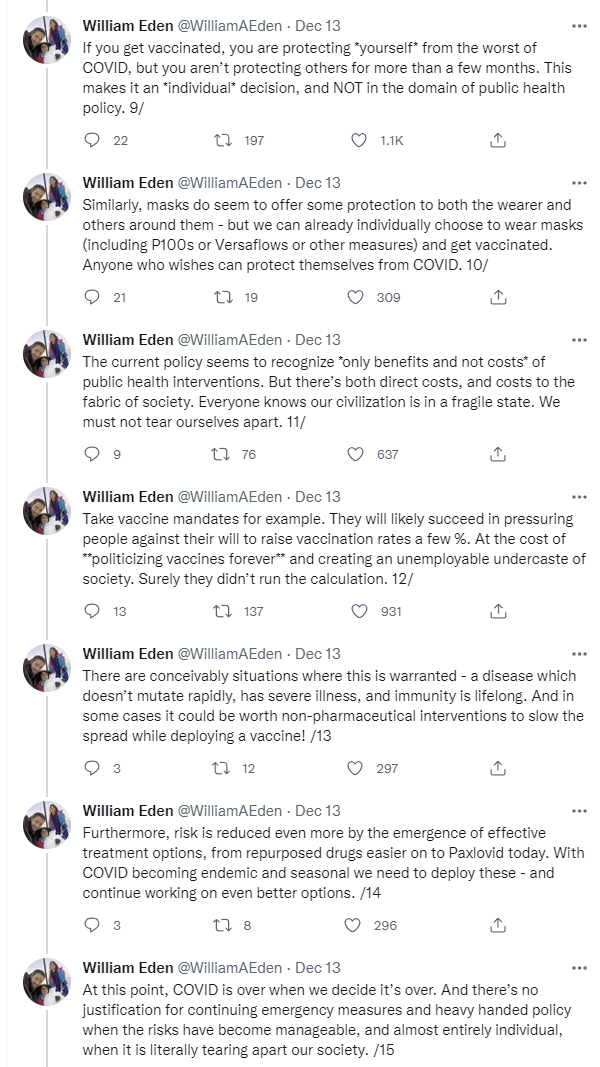
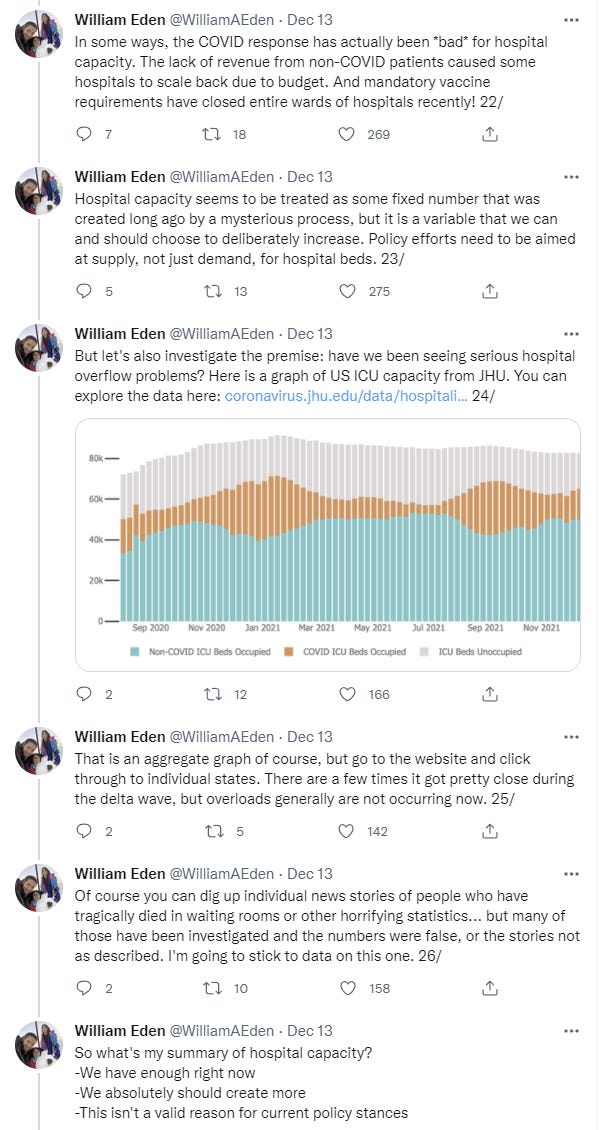

I could quibble but mostly I’m on the same page. The exception is that Omicron is about to come on stupidly fast, and that’s one curve that there could be a lot of value in flattening this (hopefully last) time, including to buy time for Paxlovid, but it doesn’t look like there’s that much capacity coming in time, the Omicron boosters are way too slow to make a difference, and generally the few ways to use the time we might buy have been ignored. It’s time to accept that it’s over.
Words of wisdom from Taleb on vaccine safety, for those who need them.
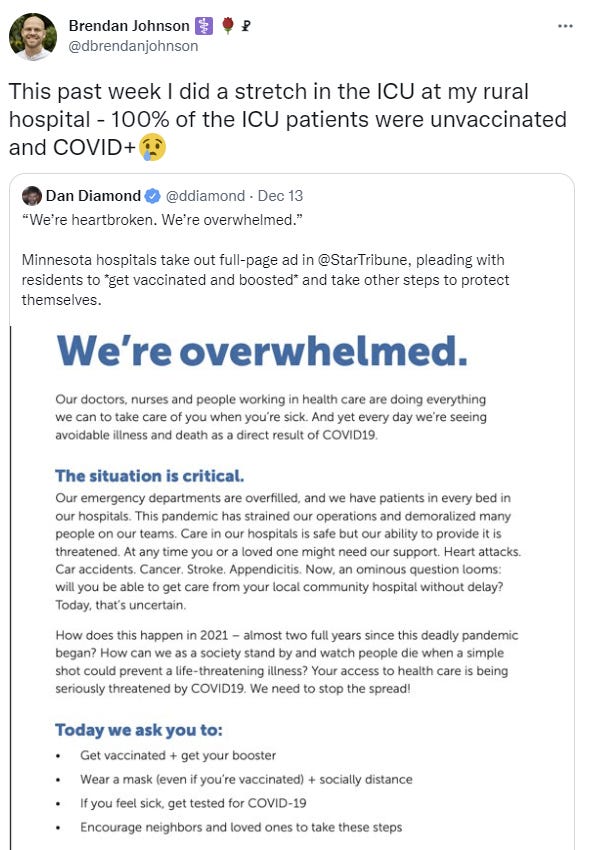
Hospitals in Minnesota already overwhelmed, and things are about to rapidly get much worse.
Thread discussing media coverage of the lab leak hypothesis, and in particular even now continued attempts to use frame manipulation on the social level to hammer people who don’t fall in line and agree to treat this highly plausible hypothesis as conspiracy theory, even as it was quietly removed entirely from the semi-official graphical conspiracy theory pyramid.


I strongly agree with Kelsey’s perspective here. Whether or not the virus came from a lab (and whether or not Omicron came from a lab), the gain of function research going on is stunningly irresponsible and we’re doing nothing to address this. Except it’s not merely a project that risks ‘millions of lives,’ it’s an existential risk that could potentially wipe out humanity or civilization. The next virus might not be this mild.
Meanwhile, this week there was a lab leak of Covid out of a BSL-3 lab in Taiwan.
That Atlantic article about how no one in someone’s town cares about Covid. It opens like this:
In November, my wife asked me whether I had seen an article with the remarkable headline “Is It Safe to Go to Thanksgiving Dinner?”
“Is that from last year?” I asked.
“No, it’s a few days old,” she said, her voice sinking to a growling murmur. “These people.”
These people, indeed.
Not Covid
Also Covid, but general and important:
FDA will make hearing aids less illegal, which is expected to increase availability while decreasing price, who knew? So in this case, the FDA has indeed stopped beating its wife. Which is good.
A bit on how they calculate hospital prices to put maximum pain on anyone foolish enough to show up without insurance but with money they can collect.
As the Prophet Zvi foretold
> Except it’s not merely a project that risks ‘millions of lives,’ it’s an existential risk that could potentially wipe out humanity or civilization. The next virus might not be this mild.
I think it's a slight exaggeration? I mean, we're not doing much to actually fight against the pandemic, in absolute sense. I assume if there was a _really scary_ virus (smallpox?) things like FDA obstructionism would be abolished under the pressure. Also, people would actually do the social isolation thing.
Technologically, we had working vaccines even before anyone outside China was infected, so...