The traditional action for New Year’s Eve is to go to a party, stay up until midnight and watch the bell drop, and the traditional song is Auld Lang Syne.
I’ve stopped doing any of these things.
My traditional action is now to watch a bunch of great college football games that are the cumulation of the year’s season, and maybe have a few friends over.
As for songs, I have two. First, to look back on the year and the ways one is stuck, and think about and motivate what one might change, Anastasia’s Same Old Story. Then, to remind that life is awesome and my life is awesome, Jewel’s This Way.
I work at a large teaching hospital in the UK, but outside London. I’ve been isolating for a while (very mild if any symptoms, but was undergoing regular testing at work). Prior to my isolation, there were rising numbers, but they were still using respiratory beds for ‘Incidental Covid’ types. Anecdotal observation supported the idea that staff isolation and the need to isolate from vulnerable Covid-negatives was more of a challenge at that point than any influx of very unwell Covid pneumonitis types.
I’ll aim to update when I’m next in work.
…
I’m back in work now. There’s a small uptick in actual respiratory admissions but most of the increased Covid capacity the hospital has put together is being filled by geriatrics patients who happen to have Covid. A friend who works at a nearby hospital reports that she has about a quarter of her unit in self isolation for one reason or other.
It’s actually remarkable how few people are coming in with fevers and breathlessness.
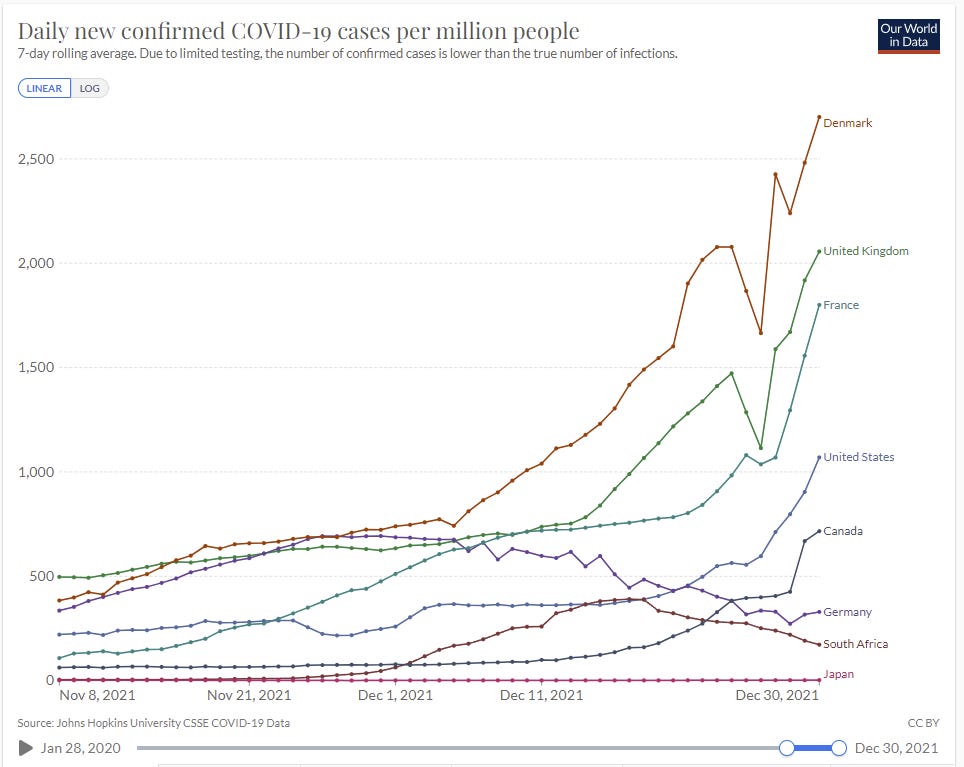
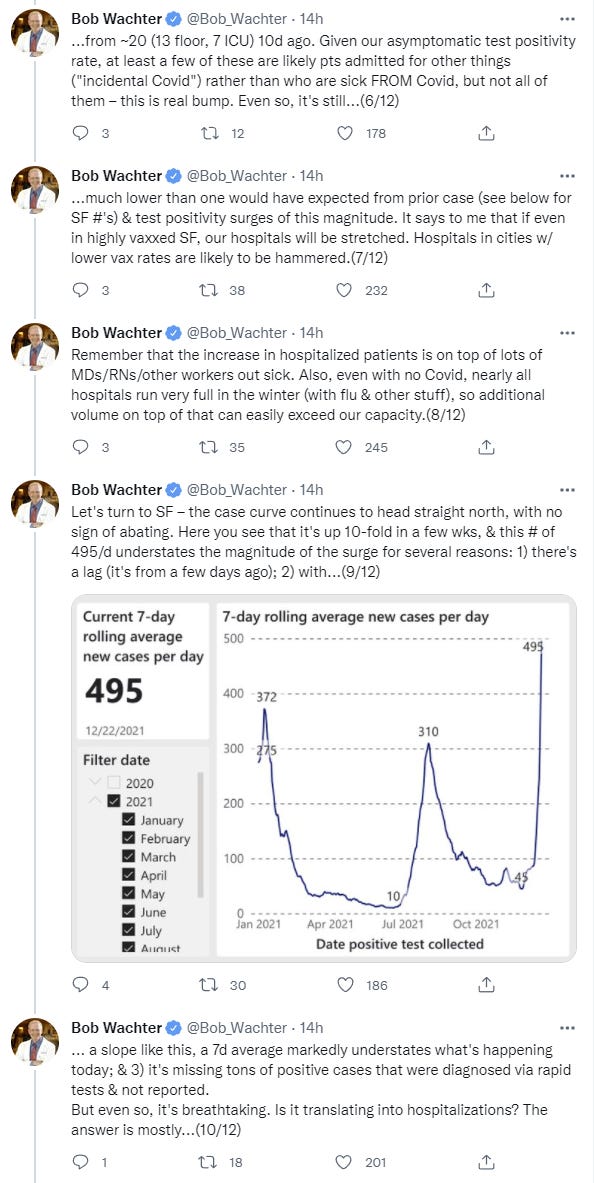
If we do have access to the numbers on any of that, please do share, for now I only know of such numbers in San Francisco.
If we use the black line, the average is now over four times the previous maximum level. If we use the recent data points as an indication, there’s at least one more doubling after that.
This seems roughly right to me. If you have a highly vaccinated population and solid hospital capacity, even with this rapid a storm, we should mostly be able to muddle through, things can only add to 100% (and presumably cap out at more like a total of 80%-90%). If the peak is as high in rural areas with less beds and less vaccinations, I’d be a lot more nervous.
Note that San Francisco’s positive rate is somewhat lower than the national average, so it’s probably missing a slightly lower percentage of its cases than other places.
21% of the NYPD was out sick Thursday in what outgoing Police Commissioner Dermot Shea said was the highest level of sick employees he had ever seen. 17% were out a day earlier.
"When you look at March 2020 we peaked at 19.8%, we hit 21% today," said Shea during a briefing on security for New Year's Eve festivities in Times Square.
I still don’t know how to properly translate a 16% positive rate into an expected percentage of cases being missed, but this will likely be the best way to tell now whether things have actually peaked or not. We previously peaked at around 23% on this chart early in the pandemic, with 50%+ rates in New York City, on vastly less testing.
Vaccine Effectiveness
A commenter on the last post notes that in Canada, while measured vaccine effectiveness in preventing infections dropped to zero or below (I continue to think this is a rural/urban effect in large part), against hospitalization it’s still strong. Graham thinks the essential story is that vaccine protection against severe outcomes is holding but doesn’t believe that Omicron is much less virulent than Delta (to continue to note that opinions on this differ.)
Using Alberta, Canada numbers. The current rate of those hospitalized who were vaccinated is 3.68/100k, and among the unvaccinated it is 20.17/100k. On December 4 it was vaccinated 3.84/100k and unvaccinated 26.69/100k. Since the rise of Omicron, the rate of hospitalizations has actually gone down in both populations, but the vaccinated now have a slightly higher relative rate of hospitalization than they did pre-Omicron. (Vaccinated rate was 14.4% that of the unvaccinated rate 3 weeks ago, and now it is closer to 18.2%.)
The FDA uses the magic weasel words and claims rapid tests ‘may have reduced sensitivity’ to Omicron. Given the nature of what ‘may’ be true, such statements are always technically correct, and also always the ‘may’ mostly gets translated as ‘do’ or at least as ‘probably.’
I translate it that way too, because that’s the claim they’re effectively making. If you don’t have a very good reputation for your words having meaning, I’m not going to let you pull this transparent a weaseling that doesn’t deserve the dignify of being called a motte-and-bailey.
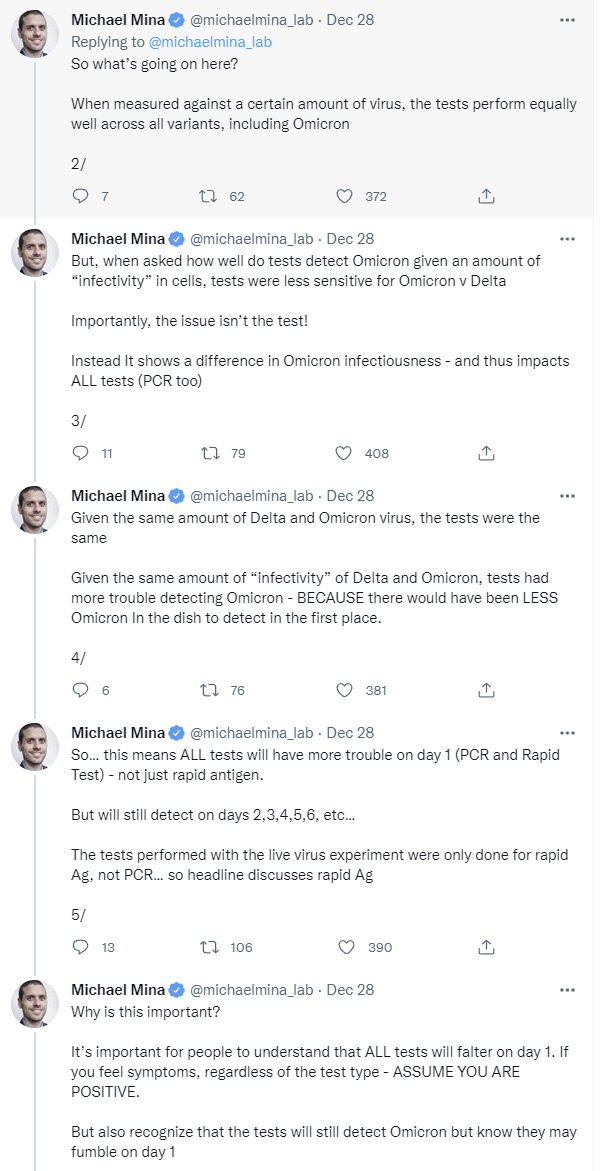
Mina’s prior seems right to me, but that interpretation doesn’t mean everything is fine. This still means that a rapid test is less effectively sensitive for knowing if you’re infectious. Which is what they’re for, so there’s still a problem whether or not the test is technically less sensitive. What matters is the practical utility of the test, and what it tells you.
I do agree that giving out vague ‘may be less effective’ warnings based on preliminary data is a good way to completely freak out a lot of people in an unhelpful way, without much in the way of upside.
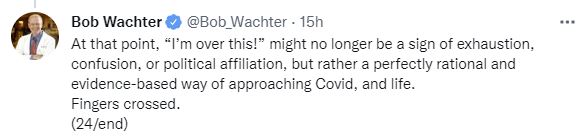
One can see this as the ‘less action’ camp versus the ‘more action’ camp, and there’s something to that. But it’s also important to notice that different actions make sense in different circumstances. The CDC reduced isolation requirements because conditions got worse, and it was necessary. That doesn’t contradict taking more precautions in other ways, nor does it require having an attitude of moving on.
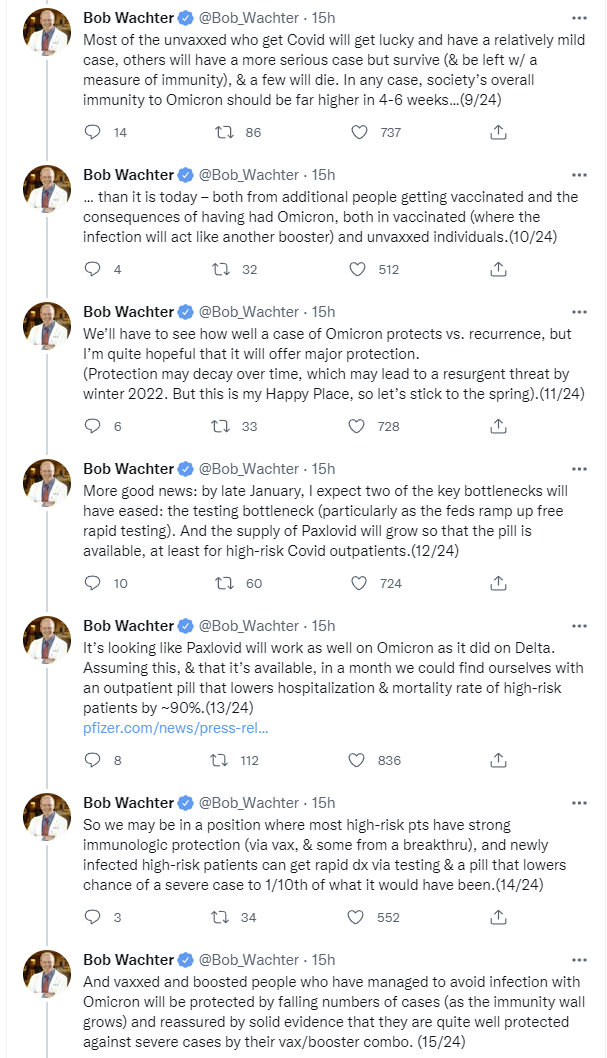
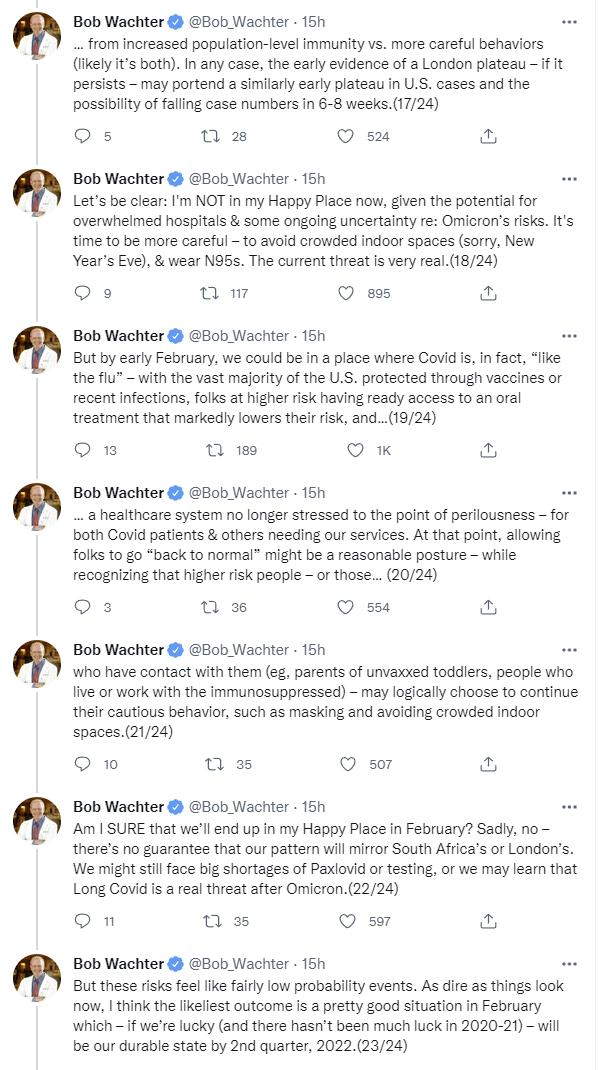
Three or four weeks with the promise of light after that seems highly survivable. That’s an accelerated timeline and it could easily take longer, but the restaurants should be fine not too long from now, if people use their heads.
The thing is, if you have already had and recovered from Omicron, restaurants are fully open for your business. About one in ten Londoners had the virus at one time this past week. All those people, or least the ones that are aware of it, can then fully exit their lockdowns. A month later, half the population can be partying like it’s 2019, on top of the ones who already didn’t much care, even if things haven’t fully died down yet.
It’s a good question. Some of the confusion is that ‘collapse society’ is not a well-formed concept here. There are different levels of sacred value, and things we are and aren’t prepared to accept, as things get more dire, and trade-offs are being made. If the situation were different and worse, it would require different trade-offs.
Letting the original strain rage freely would not have collapsed society. It would have killed a lot of people and scarred pretty much everyone, but most of us would have survived and moved on. Forcing everyone with Omicron into extended isolation would shut down a lot of things over the next few weeks (with little upside to compensate) and if this included hospital staff it likely kills more people rather than less people. But we can survive those kinds of disruptions, it would be quite bad but the unthinkable now becomes the thinkable tomorrow.
But maybe that’s wrong? If we’d suffered a 4% death rate in the first half of 2020, what happens? What about if the supply chain problems hadn’t turned around?
The other perspective is that perhaps we really are a society on the brink of collapse, that can no longer be resilient in the face of threats, and we’re now dodging civilizational collapse on a rolling basis until at some point we fail to dodge it. In this model, the close calls we’ve had recently were actually remarkably close and could easily have gone in other ways.
In this case, I think we know the answer, because there was a lot of uncertainty about severity, and Bruno’s scenario was very much on the table until a week or two ago. It seems clear we were pretty committed to this course of action either way, and we’d have had to accept the consequences.
What about if we go to the next hypothetical? What if Omicron was more infectious by default and had also rendered the vaccines completely ineffective on all levels? At that point, I do think we have a real crisis where all the choices seem impossible, because we really can’t actually contain this thing under those conditions, but letting it rip would have unthinkable consequences and we’d be forced to try to slow things down, even though it would be a mistake - we wouldn’t be able to do enough slowing to have that much marginal effect.
At that point, the correct reaction really would be a ‘protect the vulnerable as best we can’ style reaction, while actively letting things go as quickly as possible otherwise to give that strategy a chance. I don’t think we’re capable of implementing that. But it’s important to note that we don’t know, and won’t until we are forced to run the experiment. The wartime generals are available if things get bad enough for the phone to ring.
This seems like wishful thinking with regard to testing capacity, and also Paxlovid availability in the short-to-medium term (it’s also explicitly labeled wishful thinking, which is fully allowed.) My guess is London won’t peak until this coming week, but it’s impossible to tell because at such high levels you’re in the Fog of War and the official numbers aren’t helpful. Medicine and logistics are different magisteria.
But the rest is most of it and doing most of the work, and it checks out, so long as one reads February as the end of the month.
The current shortage in hospitals, WaPo reports (no paywall), is not equipment or beds but health care workers, because so many are sick and everyone is burnt out and stretched to the limit already after two years. Short term we’ve lowered isolation requirements, but there’s little we can do. Long term, the obvious solution is to expand supply by lowering the regulatory barriers that create artificial scarcity.
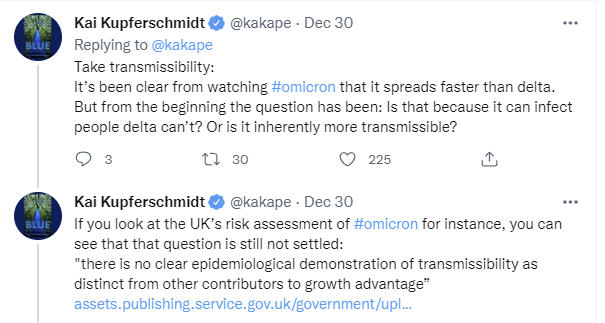
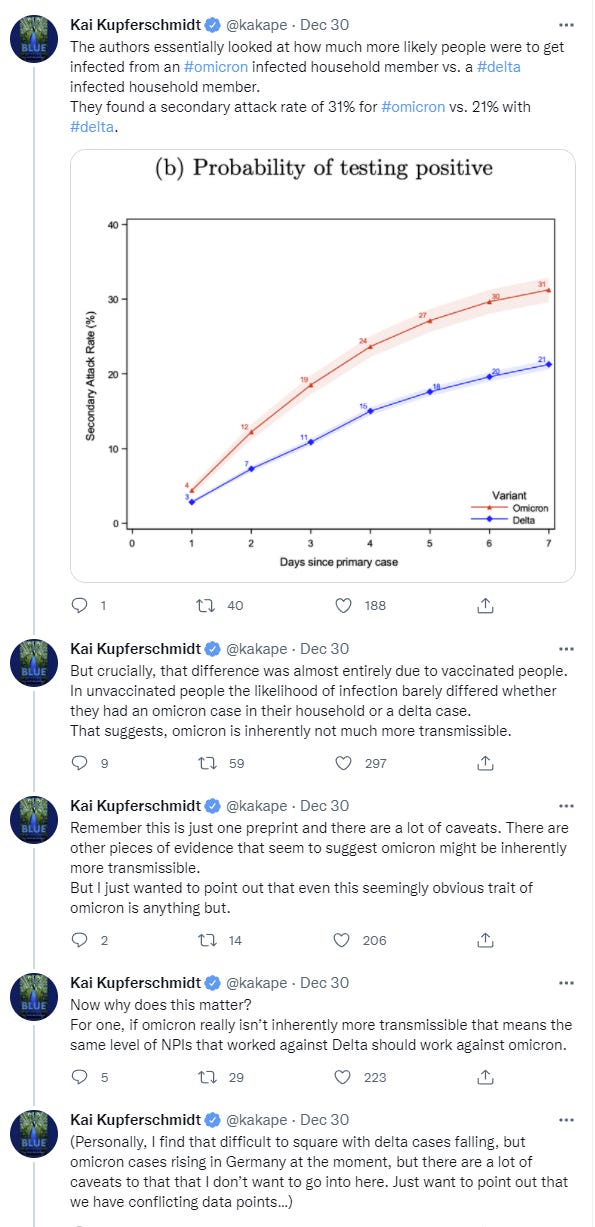
Kai looks at the question of how much of increased transmissibility is evasion, versus being more infectious (I’d add versus there being a shorter generation time, as well).
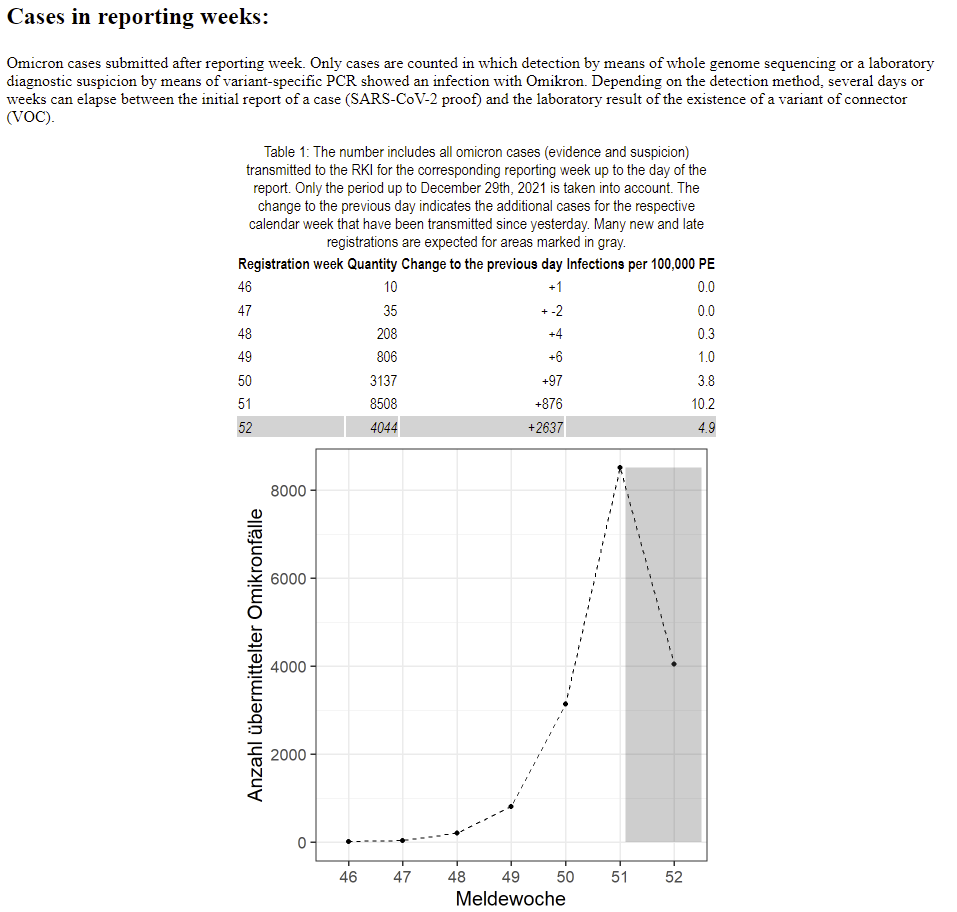
It’s worth noting that such official reports are often rather far behind, and a ‘no clear epidemiological demonstration’ type of statement from such a report means little.
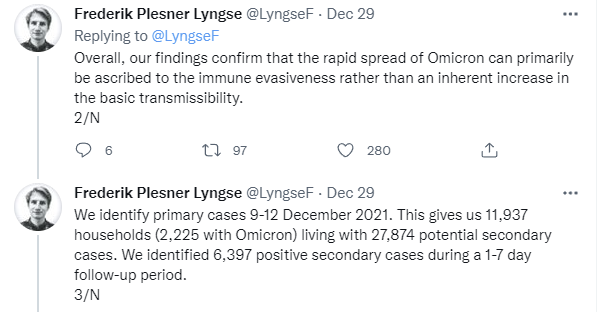
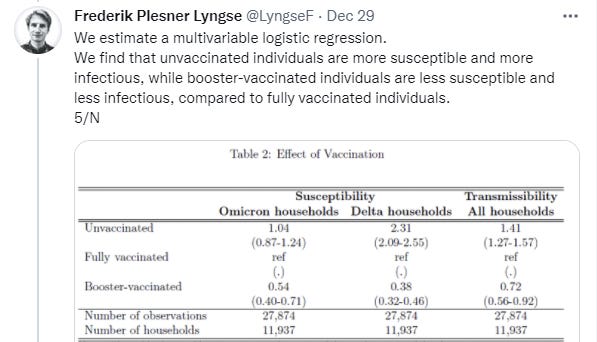
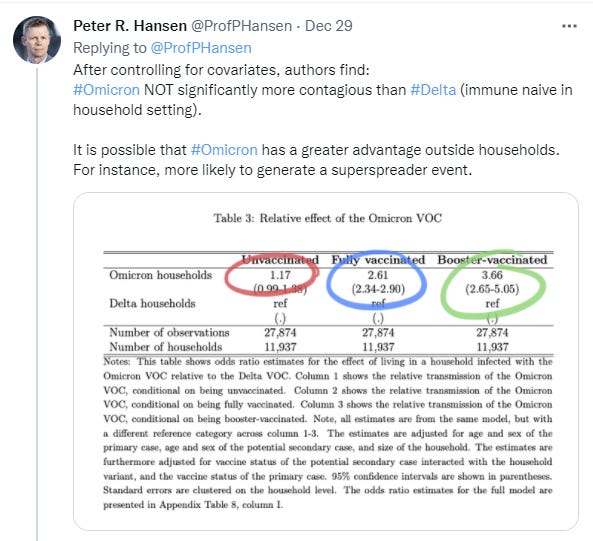
Comparing households infected with the Omicron to Delta VOC, we found an 1.17 (95\%-CI: 0.99-1.38) times higher SAR for unvaccinated, 2.61 times (95\%-CI: 2.34-2.90) higher for fully vaccinated and 3.66 (95\%-CI: 2.65-5.05) times higher for booster-vaccinated individuals, demonstrating strong evidence of immune evasiveness of the Omicron VOC. Our findings confirm that the rapid spread of the Omicron VOC primarily can be ascribed to the immune evasiveness rather than an inherent increase in the basic transmissibility.
I do find this to be strong evidence that the transmission advantage is more heavily weighted towards immune evasion, which in turn suggests a lower generation time in order to make the whole picture work.
I’m updating in that direction based on the study, although the 17% inherent increase here (whether or not it’s ‘significant’) is still a substantial push on its own given we were already being pushed to the limit, I take the 17% seriously as far as it goes, and I agree with Hansen that in other contexts the edge could easily be far bigger.
Focus on vaccination still seems like the best approach. I agree that it’s less good at ‘stopping it from spreading’ but that’s no longer on the table. Western countries could not have contained Delta without vaccinations, so ‘the same NPIs that contained Delta’ are doubly not an option. We couldn’t do again what we did before even if it would work, and even if we did it again somehow anyway, they wouldn’t work.
This helps clarify what is happening and project things forward, but in the central case it changes things very little.
Other Omicron News
If you want the ‘oh no everything is terrible we are doomed’ perspective in relatively credible form, my attention was just drawn to Tatiana Prowell, who is good for an endless stream of terrible data points if that’s something you are interested in. Things definitely aren’t going to be fun in many places over January.
I didn’t find the ‘look for all the scariest possible data points’ data stream to be especially more or less scary than I expected it to be, so I didn’t update much, but it’s good to have it in one’s mix, and to know that some people are making predictions like this:
I don’t think that’s right, but if there are key supplies like prescriptions you need over January, yes, definitely get them now. Make sure you can weather some supply chain disruptions in case they happen, just in case. Better to play it safe, 10% is not 0%.
If we assume that the exposure to SARS-CoV-2 was on the evening of the gathering, the incubation period was short, ranging from 2 to 6 days, with a mean incubation period of 3.24 days (95% CI 2.87- 3.60). Time to resolution of symptoms varied, and at the end of follow-up, five individuals still reported symptoms, while the rest reported symptoms lasting 1 to 9 days.
A ‘near miss’ with severe symptoms is disappointing, but in the most important sense this is still another 0 for 21.
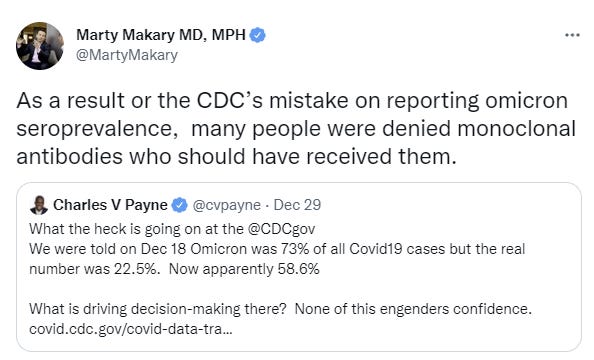
I’d also note that if you have the monoclonal antibodies, even if you think they’re only 27% to work, wouldn’t you use them anyway? I’m pretty sure they’d still pass the cost-benefit test, and next week they’re going to be even less likely to work.
Not Omicron so holding off on the full discussion but if you haven’t seen the thread discussing an attempt to publish a paper with the CDC, you should go ahead and read it now, in a ‘offered without comment’ kind of way, in the meantime.
Probability Updates
I was asked in a comment whether I am measuring my calibration. The answer is that I am not, and I consider that but a small part of prediction evaluation, but if someone else wants to do that (without me anchoring you on how to do that measurement) by all means go ahead.
Chance that Omicron has a 100% or bigger transmission advantage in practice versus Delta: 65% → 70% (EDIT: → 60%)
The new study says 161% in vaccinated people, 266% in the boosted, 17% in the unvaccinated. I originally thought that was more than 100%, but I did the math wrong and it’s not, so I should have adjusted the other way, but one does not edit prediction probabilities cause that’s cheating.
Chance that Omicron is importantly (25%+ in the same person) less virulent than Delta: 80% → 85%.
Chance that Omicron is vastly (75%+ in the same person) less virulent than Delta: 20% → 20%.
Didn’t get much new evidence and thus not much additional clarity, but if there wasn’t at least the 25% level we’d expect to see trouble in ways we are not seeing, so we can get more confident there.
Chance we will be getting boosters modified for Omicron within 6 months of our previous booster shot: 25% → 20%.
Israel floated a fourth shot when it still mattered and pulled back. On reflection I see it as less likely that, in a world where Omicron is rapidly declining, we’ll tell people to get fourth shots this quickly, especially with severe disease protections holding.
Chance we are broadly looking at a future crisis situation with widely overwhelmed American hospitals, new large American lockdowns and things like that: 15% → 10%.
The math seems to indicate that the major city hospitals, under large vaccination rates with good capacity, will hold. If that’s true, even with the rural ones already in trouble now, I don’t see a way for this to be a crisis that makes this true, and everyone is moving towards a ‘life must go on’ position. I’m not ready to call this quite yet, panic can still be a thing, but Washington DC is being hit very hard and mostly not flinching. In another week we can likely mostly write this off, except in the scenarios where we suddenly can’t.
Generation time (serial interval) of Omicron is 3.5 days or less: 85% → 85%.
Didn’t learn much, the superspreader event wasn’t that helpful.
Hold on a minute... Omicron seems to be mainly concentrated in the upper respiratory tract, unlike Delta and the original Wuhan strain.
Evidence that Omicron is displacing Delta comes mainly from sequencing done on PCR tests - but PCR tests are done based on taking swabs from the nose and tonsils, i.e. the upper respiratory tract. So how do we know that there aren't many patients that have BOTH Omicron AND Delta, but with the Delta concentrated in their lungs and the Omicron concentrated in their upper respiratory tract? Couldn't that be the case?
And how do we know that deaths attributed to Omicron aren't actually deaths due to Delta having been in the victim's lungs? Particularly since, as I understand it, previous strains, when they cause fatalities, typically end up killing the patient AFTER the virus has already been pretty much cleared from the body - it's an immune system overreaction!













Hold on a minute... Omicron seems to be mainly concentrated in the upper respiratory tract, unlike Delta and the original Wuhan strain.
Evidence that Omicron is displacing Delta comes mainly from sequencing done on PCR tests - but PCR tests are done based on taking swabs from the nose and tonsils, i.e. the upper respiratory tract. So how do we know that there aren't many patients that have BOTH Omicron AND Delta, but with the Delta concentrated in their lungs and the Omicron concentrated in their upper respiratory tract? Couldn't that be the case?
And how do we know that deaths attributed to Omicron aren't actually deaths due to Delta having been in the victim's lungs? Particularly since, as I understand it, previous strains, when they cause fatalities, typically end up killing the patient AFTER the virus has already been pretty much cleared from the body - it's an immune system overreaction!
What would you estimate is the probability of the CDC identifying Omicron as a Variant of High Consequence?