Omicron Variant Post #2
We know somewhat more now. The speed premium waits for no one.

It’s now been three days since Post #1. The situation is evolving rapidly, so it’s time to check in. What have we learned since then? How should we update our beliefs and world models? There will inevitably be mistakes as we move quickly under uncertainty, but that’s no reason not to do the best we can.
Update Update
What should we look for here and in the coming days?
No news is good news. Omicron is scary because many scary things are possible. The worse things are going to get, the sooner they will make themselves known. When we get news that something has happened, especially news that isn’t the result of a lab or statistical analysis, that will typically be bad news, but we expect a certain rate of such bad news. If we get less than expected, that’s good news.
The pattern of where and how we find cases, and the details of those cases, will give us better insight into how widely and quickly, and in which directions, Omicron has spread. This will tell us how far along things are, and give a better estimate and narrower range of how infectious Omicron can realistically be.
Information on how deadly Omicron is should update us quickly, and matters a ton for how to react, but beware of confounding factors, motivated statements and misunderstandings in both directions, and small sample sizes. Hospitalizations are not a natural category and at this stage deaths will be rare unless things are much worse than we expect. How mild the cases we find are will largely depend on how we are testing. Details matter.
The reaction of various countries, the stock market and others will continue to tell us what they think is going on, what they expect to happen next, and how they respond when such things happen. The general vibe of elite and media messaging also reveals much information, with a focus on what kinds of actions they will try to engineer rather than the ‘facts on the ground.’
Information on immune erosion will come from results from laboratory analysis and other looks at Omicron’s mutations, and other physical detail information, such as testing antibodies, and from statistics on who gets infected or sick once we have enough cases for that to mean something. It also comes from knowing how infectious Omicron is, since if we know how fast it’s spreading and we know how fast it spreads to the immunologically naive, we also then know how immune erosive it is because math. The vaccine reactions will also tell the story - we should expect manufacturers to react to the situation based on what they know, and to some extent governments as well.
A lot of updating is having time to think, and integrate others who also have time to think. There doesn’t need to be new information for our estimates to improve.
It’s been announced that new versions of the vaccines are indeed coming, as they no longer expect the old ones to be fully effective, and are talking about a few months to get the new versions online.
Noah Smith gives his overview of the situation here. It provides a lot of the same links, some good new links, a set of views broadly similar to mine, and is generally reasonable. I do disagree with the conclusion, in that I think on the margin the most valuable focus is now testing and treatment, with further vaccinations vital but not primary. Ramping up vaccine production capacity is still a fantastic idea. I will also be checking out his list of Covid experts on Twitter. A lot of them are not people I am already following.
Here is Weekend Editor, author of many helpful comments and overviews, offering their best take, broadly compatible with mine, including an addendum right at press time. An especially worthwhile note there via Your Local Epidemiologist:
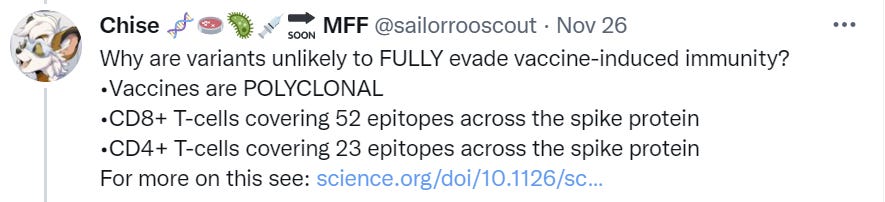
Boosters not only raise the number of antibodies, but also the diversity of antibodies to various spots on the spike protein. [11] So it’s important to get a booster once you’re eligible: you not only get short- to intermediate-term increased immunity from antibodies, you also get long-term increased immunity because your antibodies check more carefully for mutations in the spike protein, giving broader immunity to variants. That’s in addtion to antibody maturation, where your immune system refines the antibodies over time to get better and better; your memory B-cells are busy.
This set of slides is mostly a good summary with some exceptions, such as (in the mind of my instinct viewer) incorrectly associating the current winter wave of Delta with the emergence of Omicron, when they are two completely distinct things.
Immune Erosion and Transmissibility
Here is the WHO announcement on what we know, in which they reiterate all the things they would have said last week but deny that it’s possible to know things under uncertainty:

An article on Stat News is a reasonable summary, and adds one key bit of information I hadn’t seen at the time:
The WHO said Saturday that early evidence indicated the variant was causing reinfections at higher rates than other variants in South Africa, suggesting some ability to get around the immune response.
As a reminder, when the majority of people in your country are not vaccinated, this kind of observation very much isn’t news:
Joe Phaahla, South Africa’s health minister, said Friday that breakthrough infections were occurring in the country, but the majority of hospital admissions remained among people who were not vaccinated, suggesting that vaccines were still maintaining some level of protection against Omicron. But, he acknowledged, “it’s still early days in terms of this particular variant.”
It’s possible that this is uncharitable and he was making a more meaningful observation, but he’s not claiming to have done so here.
Science offers a similar article, of the ‘this is scary but we don’t know anything for sure yet’ variety, emphasizing that the rate of growth combined with the mutations are the reason we are so concerned at this early stage, but that the growth rate could mostly be a coincidence.
Here’s a similar thread of a lot of ‘we don’t know’ strung together. It’s good to caution against overconfidence, but also important not to respond to uncertainty with only ‘we don’t know.’
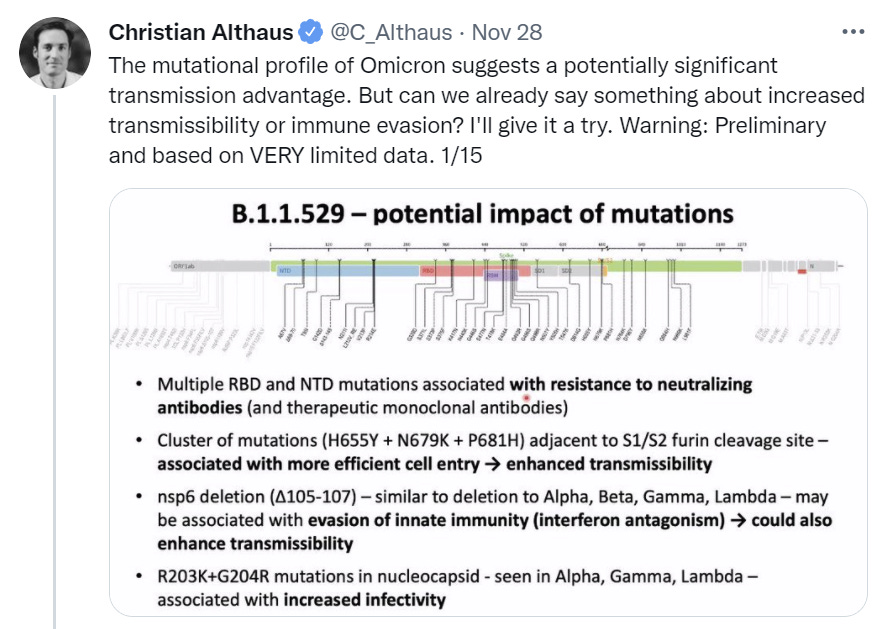
Here is a thread from Christian Althaus asking what we can say about Omicron’s potential advantages.



This is 0.38 to 0.43 advantage per day. That’s a gigantic transmission advantage if anything like it holds up. Definitely well over 100% advantage the way it’s typically measured.
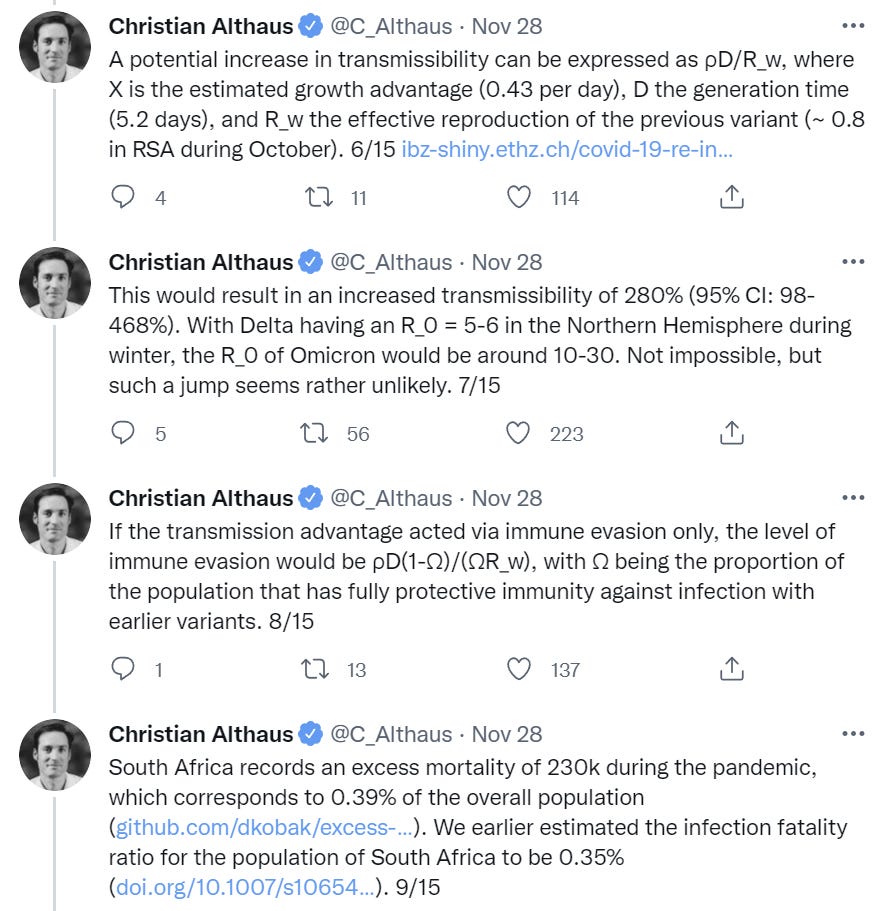

I am skeptical of ‘almost everyone.’ I can believe an IFR of 0.35% on its own, but some numbers: 89k confirmed deaths in South Africa out of 2.95mm confirmed cases, overall population 59.31mm. If almost everyone is infected then we’re talking about missing >90% of all cases, and about half of all deaths, and the IFR remaining 0.35%, excluding reinfections, at that level of care. Still, I am willing to buy that we’re missing a large majority of infections.
The WHO is saying that it looks like Omicron is ‘causing reinfections at higher rates’ but if almost everyone has already been infected in South Africa, then that’s not the observation it sounds like it is. It’s instead a statement that those previously diagnosed are getting infected more often than those who previously had milder cases that went undiagnosed, which is very different in its implications. It also seems like evidence that South Africa hasn’t mostly already been infected.
I like how this points out the relationships involved and how different numbers need to relate to each other. Those relations don’t change that much based on the share that had immunity, so long as that share was ‘large.’ It does emphasize that there’s too many free variables, and for now we can’t draw conclusions off an analysis like this, only constrain the set of possible worlds.
Several people pointed me to this Times of India report:
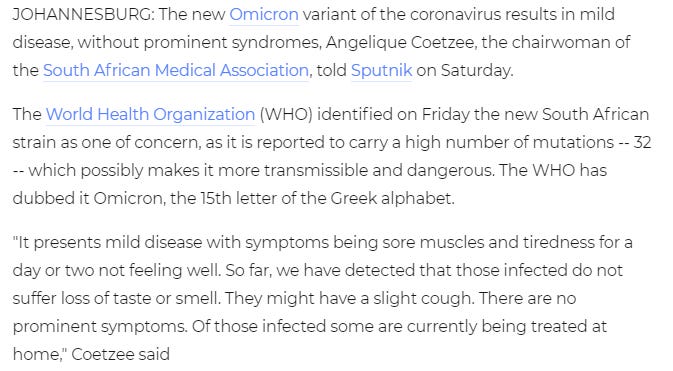
That would be the best case scenario. If Omicron only results in mild infections, we should welcome our new Omicron overlords as opposed to imposing new restrictions. However, it’s way too early for that, and the cohorts involved seem like they were younger and healthier. Here’s what I believe is another take on the same statement, from Haaratz:
According to the report, omicron patients tended to be younger, and the variant was not found as often among the older population. Those infected with the variant mainly experienced fatigue and body aches. Still, it is still unknown what effect infection has on the older adults with underlying medical conditions such as diabetes or heart disease.
Prof. Dror Mevorach, head of the coronavirus department at Hadassah University Hospital Ein Karem, said the preliminary reports on the clinical condition of people infected with the new variant are encouraging. “If it continues this way, this might be a relatively mild illness compared to the delta variant, and paradoxically, if it takes over, it will lead to lower infection rates,” and it will be easier to deal with globally.
Here’s another report, this time from the Telegraph. Once again, cohort young and healthy, but symptoms more mild than would have been expected given that.
Goldman Sacks endorses that the vaccines will keep working, does not recommend portfolio changes.
Travel Restrictions
Inevitably we are seeing a lot of this:
All-or-nothing arguments continue to be depressingly common. Either the vaccinations ‘prevent infection’ or they don’t, either something is safe or it isn’t, and so on.
As I noted last time, travel restrictions have zero chance of stopping Omicron, but they will be effective at slowing down Omicron so long as there is a large asymmetry in Omicron’s presence in different areas. I do think the time will come relatively soon when the restrictions stop accomplishing anything, but that time is not today.
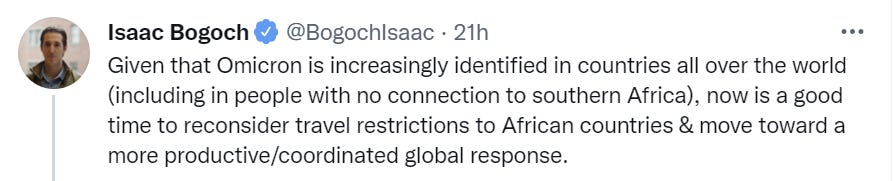
This makes both ends of that even clearer, that it is both too late, and vital to slowing down spread if that is something you value:
I do think it is important to show our support for South Africa, its testing and its openness. They did a heroic job and right now it’s being effectively punished. What we don’t want to do is make that reward ‘lift the restrictions,’ we want to send them other forms of aid instead, both direct help and cash and hopefully better trade and other relations, which together leaves everyone better off.
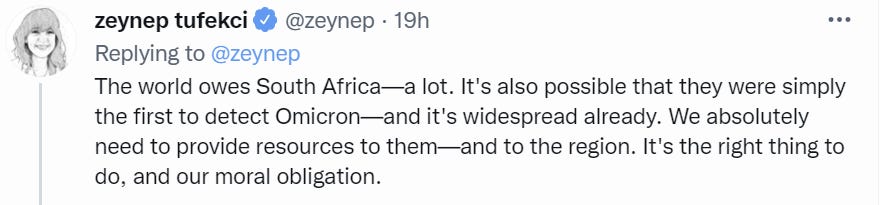
So strongly agree with this:


Meanwhile, mainstream sources say things like this with straight faces.

Yeah, travel bans are one thing but it is really really not too soon to cancel your own trip.
Merlin recommends that travelers have a back up plan, suggesting trip stacking as a potential strategy. He said travelers should follow the news closely for updates on the omicron variant and resulting restrictions — not just for Africa but for parts of the world experiencing coronavirus surges, like Europe.
I am no travel expert but your backup plan right now should very much be ‘stay home for a while’ or at least something not international.
Vaccinations and Boosters
If you’re worried your booster shot is interfering with other people’s access to the vaccines, or with ‘vaccine equity,’ please stop. You’re not doing that, except to the extent you having less and someone else not getting more means more ‘equity.’ Link to article Alex links to. South Africa in particular has a surplus, the same as we do.

If there is a new Omicron vaccine, there will once again be scarcity, but right now the bottleneck is distribution and not supply. If you’re not taking up scarce distribution, go for it.
Lockdowns
Be very afraid of this attitude.
Americans need to be prepared to do “anything and everything” to fight the omicron Covid variant, U.S. infectious disease expert Dr. Anthony Fauci said Sunday.
Still, it’s “too early to say” whether lockdowns or new mandates will be appropriate, Fauci said on ABC’s “This Week.”
Anything and everything is an appropriate response to an existential threat. I still have some probability mass in Omicron being deadlier than Delta, but almost none that it is sufficiently deadly that ‘anything and everything’ would make any sense. That kind of rhetoric is laying the foundation for very poor trade-offs whose advocates are not doing any sort of cost-benefit analysis. It’s important to be ready to push back.
Similarly, notice rhetoric where lockdowns are punishments for non-compliant populations who have sinned against public health, rather than a tool to accomplish a goal. Here’s CNN, note the headline about ‘the virus is in control’ framing the situation as being about who is in charge and who is or isn’t following orders properly:
The new Omicron variant might prompt a return to stricter Covid-19 measures if not enough people get vaccinated or boosted, health experts say.
…
"It ought to redouble our efforts to use the tools that we have, which are vaccinations and boosters -- and to be sure we're getting those to the rest of the world, too," Collins told CNN on Sunday.
"It also means we need to pay attention to those mitigation strategies that people are just really sick of, like wearing masks when you're indoors with other people who might not be vaccinated, and keeping that social distance," he said.
…
"I think we may, indeed, be in for a phase of many more masks, much more social distancing, and more restrictions and obligations for vaccination going forward," Schaffner said.
That doesn’t mean there are no scenarios where a very short term lockdown would pass a cost-benefit test to ‘flatten the curve’ or buy time for treatment supplies, but the bar on that is high and the chance of an appropriately timed response is low. Locking down or taking other extreme measures too early is quite bad, as is maintaining lockdown for too long, and conditional on lockdown I expect both.
The scariest signs are coming here in New York, where I am worried I am going to start missing Andrew Cuomo and I do not even slightly miss Andrew Cuomo.
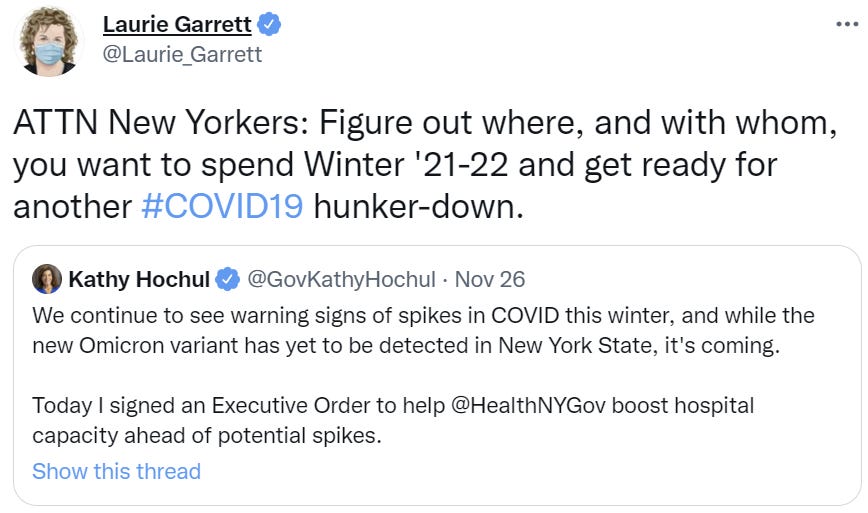
Kathy Hochul has no idea how exponential growth works. Clearing hospital capacity now and stopping elective surgery now is exactly the opposite of any reasonable procedure. Even in the worst case scenarios, Omicron won’t have much impact on case numbers for several weeks. After that, however long we have, we will need all the capacity we can get. The time to get other stuff out of the way is now.
The Timeline
Once again, I’ll use BNO’s important Omicron-related headlines in chronological order to tell the story. Here’s a link to BNO’s patreon, if you’d like to help them out.

Once again, a reminder that the majority of South Africans are unvaccinated.

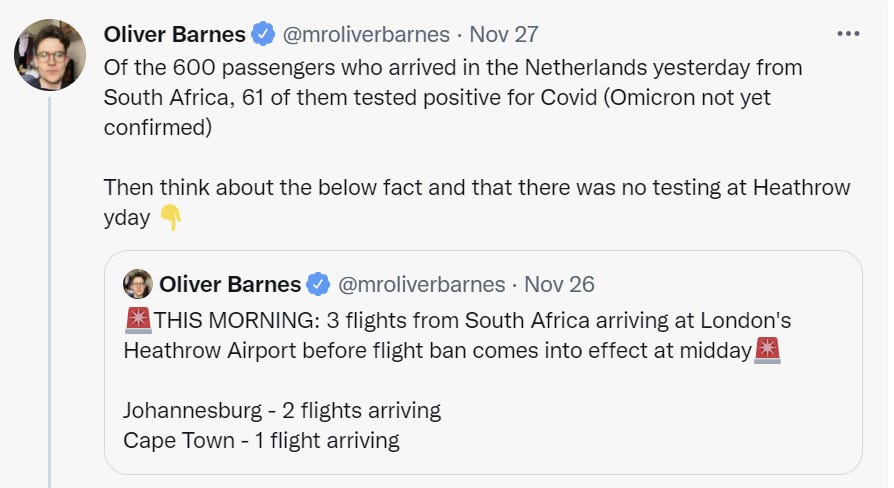
That last one slightly out of order, happened after the next two updates. The positive test rate went down somewhat but held at 10%, much higher than the positive test rate in South Africa according to Our World In Data. Travelers presumably are exposed more than non travelers, but still, especially since in SA who gets tested in based largely on who has symptoms.


It seems clear that a substantial percentage of those who fly out of South Africa are infected with Omicron, and this was mostly true the day before they started checking.

This is the kind of half-measure that will slow things down a little but isn’t pretending to want to fully work.

I am curious about the details of this.

Boom. As I noted last time, this is the only policy with any chance of fully working.

I wonder what will happen when we check travelers that aren’t coming from Africa?

What’s weird is that it was listed as probable above?

Situation in South Africa continues to escalate super quickly, after we all started panicking so it’s out-of-sample data.

Well, ****. Presumably they found it first because they were looking.






Morocco is an unexpected twist. Maybe worth keeping an eye on them.


The positivity rate continues to rise, so fall in case count presumably is about lack of testing on weekends.



This is covered earlier. A lot of ‘no evidence’ talk, since it’s WHO, but at least not actively getting in the way.

The border closing order has a lot more to do with geography, trade and culture than suspending some flights. The contrast is interesting.


That last one is interesting. Going to hold off updating much on it yet, but if true then why didn’t background sequencing pick anything up?
Other New Information
There is some worry that Rapid Antigen Tests might not work on Omicron based on the sequence, but it looks like they will continue to work. Presumably ‘run actual tests and see what happens’ is the way to find out, looks like we found out.
Early sign of political reactions that were inevitable, but whose magnitude is not.
Some amount of this is inevitable and also necessary. There are those who really would have us in permanent midnight, and there’s a chance they will win, and they would happily use variants to make that happen regardless of whether it is appropriate.
Current Model
Chance that Omicron has a 100% or bigger transmission advantage in practice versus Delta: 30% → 35%.
Omicron is spreading at an alarming rate, but my confusion about what claims were being made is gone, and this is a huge transmission advantage. The counterargument is that we are seeing a lot of Omicron in a lot of places, in large numbers, very quickly, and that an advantage in Africa need not translate to a similar advantage elsewhere and we’re asking here about the advantage that will hold in the United States, but also there’s probably immune erosion which will matter more here than it does there. Given that this is ‘in practice’ which incorporates immune erosion, I’d say I’m slightly more concerned on net.
Chance that Omicron will displace Delta: 70% → 80%.
The spread and cases we are seeing clearly indicates that Omicron is spreading fast, but there have been previous variants that have taken over in some places and failed to take over other places, so that’s still on the table as well. The pattern of cases we are seeing implies that Omicron is already in a lot of places, but it will take a while to be confident. Still, given my estimate of how likely it is to be immune evasive, it seems like I should be moving up my chance it eventually displaces Delta if no other variant emerges first.
Note that this probability is conditional on no other variant emerging first, and that a bunch of this probability involves a slow rather than fast transition, depending on the size of the transmission advantage.
Chance that Omicron is importantly more virulent than Delta: 25% → 10%.
Chance that Omicron is importantly less virulent than Delta: ?% → 40%
We’re seeing early reports that Omicron might be less virulent than Delta rather than more. It didn’t come directly from Delta, and also we’re seeing cases show up that came from various different countries without it already having been detected, which is also evidence for it being potentially less virulent. Even more than that, it seems like evidence against it being more virulent.
Also Zeynep points out explicitly a point that’s easy to miss, which is that being immune erosive will lower average severity because breakthrough cases are less severe, so Omicron will probably look less virulent even if it isn’t.
I still think the baseline scenario is that this is similar to Delta until we hear more, but the signs are promising.
Chance that Omicron is importantly immune erosive, reducing effectiveness of vaccines and natural immunity: 50% → 80%.
This is looking likely, both in terms of what we’re learning and as I get a better understanding of what our information means. The monoclonal antibodies look like they will no longer work, new versions of the vaccines are likely coming. It’s still early and I don’t want to get too overconfident, but yeah, this is probably happening.
Chance that Omicron means the vaccinated and previously infected are no longer effectively protected against severe disease until they get an Omicron-targeted booster shot: 5% → 4%.
Immune erosion against infection makes me more worried, but as far as I can tell that is fully consistent with protection against severe disease holding up fine. Every biological analysis and expert sees no reason to doubt that protection against severe disease will hold up.
The focus on more vaccinations now is additional evidence in favor of them holding up against severe disease, to the extent that it would vary based on the physical situation. If there were more serious doubts, I would have expected to start seeing much more loud calls for considering rushing the new versions of the vaccines and of considering holding off on additional vaccinations. That could be me still being naïve, though, so I’m holding onto some model uncertainty.
Chance we will be getting boosters modified for Omicron within 6 months of our previous booster shot: 15% → 30%.
They look like they are going to make Omicron booster shots, so the question is whether those already boosted will still be told to get them. Note that I consider this ‘the authorities tell you to get a second booster this quickly’ rather than ‘I personally choose to get one this quickly.’
Chance that Omicron is less vulnerable to non-antibody treatments like Paxlovid or Fluvoxamine: 5% → 3%.
No one seems to be worried about this or have any biological basis for it, and no news is good news, so I’m going down further, but I have too much model uncertainty to go lower faster than this.
Chance we are broadly looking at a future crisis situation with widely overwhelmed American hospitals, new large American lockdowns and things like that: 20% → 15%.
There’s been explicit threats and even some current emergency measures, which raises the chance that there will be large lockdowns whether or not they make any sense. In the other direction, the chance that this will be a deadlier variant has gone down and the chance it is less deadly has gone up. If we do get that kind of scenario, it’s going to be much harder to justify extreme measures, and they would face more resistance. Also, the really really bad scenarios are generally less likely due to no news being good news, and I’ve had time to think, so I’m a little lower here.
Final Thoughts
The last few days have made it more likely that Omicron is real and is coming, although it is still too early to know for sure. They have made it more likely that immune erosion is largely responsible for Omicron’s spread, as opposed to spreading more among those who haven’t been infected or vaccinated. That’s the bad news.
The good news is that it’s more likely Omicron is milder, and less likely that Omicron is more severe. And we’ve reinforced that most of our treatments still work, and that vaccine protection against severe disease should hold. We’re not going back to square one.
As an individual, the situation has not changed much. Be prepared for what might happen, and get ready to be more prepared as we learn more. If possible, get boosted. If you have things to do, do them now, while you still can, rather than prematurely locking down and doing less too early. That would only backfire.
What are the most important things to do now more broadly?
More vaccinations and booster shots help, but I believe what matters most will be our ability to:
Manufacture as much Paxlovid as possible as quickly as possible.
Get testing that will allow those with symptoms to get tested and found reliably and quickly. We still haven’t fixed this. FIX IT!
Get a distribution system ready that’s either better than or similar to the ones that exist in some states, to ensure that those who need Paxlovid and other treatments can get them quickly, without taking up too many system resources, while they will still work. If this is the kind of emergency it seems to be, once supply is adequate, you should be able to walk into a pharmacy with a Covid test you bought there, and walk out with Paxlovid, or do something damn near that. Again, FIX IT.
I will continue to monitor developments, and bring additional updates when it seems appropriate to do so.
Once again, I emphasize that I’m doing the best I can under uncertainty in a rapidly developing situation. I will make mistakes, including mistakes of thinking, and I definitely will miss important information.
I’m not looking to make any actual wagers, but I’d encourage those who have thought about things enough to have probability estimates to leave comments where you give your own current probability estimates, and explain ways in which your reasoning on them differs from mine.
Random "helpful suggestion," magnitude likely smaller than "get boosted" by substantial degree -- it still amazes me how many folks who stack all their other protection bonuses as much as possible use cloth masks instead of KN95s, and how many folks don't have tests at home despite availability via Walmart, etc.
It may be worthwhile to consider add a "I'm already vaxxed and boosted, how can I level up" section in future summaries -- even if you see it explicitly as lower ROI, it may be useful to give folks a place to put their stress energy that does have some marginal benefit, instead of them putting it in counterproductive places.
Is it really the case that WHO statement regarding reinfections is based on any non-public information, though?
Perhaps they are just inferring it from combination of things we already know, namely, 1) omicron seems to be spreading rapidly in South Africa, dominating delta, 2) lots of people in South Africa had covid, most of them "off the books", and 4) genetic makeup of omicron looks like something that could evade immunity.